Introduction
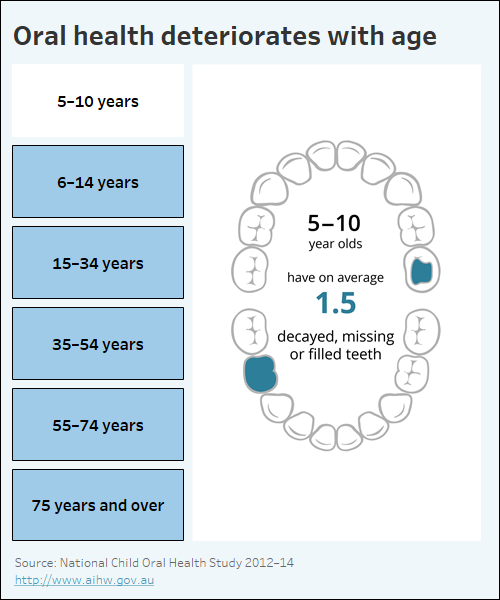
Data visualisation indicating how oral health deteriorates with age.
What contributes to poor oral health?
Many factors contribute to poor oral health (NACDH 2012), including:
- consumption of sugar, tobacco and alcohol
- a lack of good oral hygiene and regular dental check-ups
- a lack of fluoridation in some water supplies
- access and availability of services, including:
- affordability of private dental care
- long waiting periods for public dental care.
What is the impact of poor oral health?
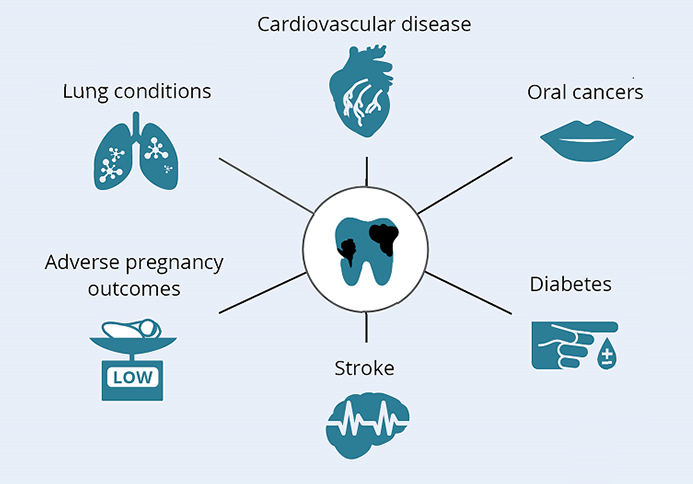
The most common oral diseases affect the teeth (tooth decay, called ‘caries’) and gums (periodontal disease). Oral disease can destroy the tissues in the mouth, leading to lasting physical and psychological disability (NACDH 2012). Tooth loss can reduce the functionality of the mouth, making chewing and swallowing more challenging, which in turn can compromise nutrition. Poor nutrition can impair general health and exacerbate existing health conditions (NACDH 2012). Poor oral health is also associated with a number of chronic diseases, including stroke and cardiovascular disease (DHSV 2011) (Figure 1).
Figure 1: Links between poor oral health and chronic diseases
Poor oral health can also affect a person’s wellbeing. Dental disease can impair a person’s appearance and speech, eroding their self-esteem, which in turn can lead to restricted participation at school, the workplace, home and other social settings (NACDH 2012).
Some groups are at greater risk of poor oral health
The National Oral Health Plan identifies four priority population groups that have poorer oral health than the general population and also experience barriers to accessing oral health care – either in the private or public sector. State and territory governments are the current providers of most public dental services, and access is largely targeted towards people on low incomes or holders of concession cards. Eligibility requirements can vary between states and territories (AIHW 2018).
The four priority population groups identified in the plan are:
People who are socially disadvantaged or on low incomes: This group has historically been identified as those on a low income and/or receiving some form of government income assistance, but now extends to include people experiencing other forms of disadvantage including refugees, homeless people, some people from culturally and linguistically diverse backgrounds, and people in institutions or correctional facilities (COAG 2015). Poorer oral health results from infrequent dental care. Barriers include cost, appropriateness of service delivery and lower levels of health literacy, including oral health (COAG 2015).
Aboriginal and Torres Strait Islander Australians: Indigenous Australians are more likely than other Australians to have multiple caries and untreated dental disease, and less likely to have received preventive dental care (AHMAC 2017). The oral health status of Indigenous Australians, like all Australians, is influenced by many factors (see What contributes to poor oral health?) and a tendency towards unfavourable dental visiting patterns, broadly associated with accessibility, cost and a lack of cultural awareness by some service providers (COAG 2015; NACDH 2012).
People living in regional and remote areas: Overall, this group has poorer oral health than those in Major cities (COAG 2015), and oral health status generally declines as remoteness increases. Rural Australians have access to fewer dental practitioners than their city counterparts, which, coupled with longer travel times and limited transport options to services, affects the oral health care that they can receive (COAG 2015; Bishop & Laverty 2015). People living in Remote and Very remote areas are also more likely to smoke and drink at risky levels. They have reduced access to fluoridated drinking water and face increased costs of healthy food choices and oral hygiene products. These risk factors contribute to this population’s overall poorer oral health (COAG 2015).
People with additional and/or specialised health care needs: This group includes people living with mental illness, people with physical, intellectual and developmental disabilities, people with complex medical needs and frail older people. These people can be vulnerable to oral disease; for example, some medications for chronic diseases can cause a dry mouth, which increases the risk of tooth decay (Queensland Health 2008). A number of factors make accessing dental care more difficult for this group, including:
- a shortage of dental health professional with skills in special-needs dentistry
- difficulties in physically accessing appropriate dental treatment facilities
- the cost of treatment. People with additional and/or specialised health care needs often have their earning capacity eroded by ill health (COAG 2015).
Why does oral health vary across Australia?
People in some states and territories have generally poorer oral health than others. For example, the National Child Oral Health Study found that the prevalence of caries in the deciduous teeth of children was significantly higher in Northern Territory and Queensland than in all other states and territories (Do & Spencer 2016). Oral health status is influenced by a complex interaction of factors, as outlined above. These factors should be considered when looking at results by state and territory. For example:
- all people living in the Northern Territory were located in Outer regional, Remote or Very remote areas, whereas the majority of the Victorian population were located in Major cities in 2016 (ABS 2017)
- the Northern Territory has Australia’s highest proportion of Aboriginal and Torres Strait Islander people (26% of its population) which is much higher than the next highest state, Tasmania (5.4% of its population) (ABS 2022)
- Tasmania has the highest proportion of people living in the lowest socioeconomic areas (37%) (refer to Technical notes for explanation of SEIFA) (ABS 2018).
The variations observed in oral health status between state and territory populations may also be partly explained by differences in individual state and territory oral health care funding, service models and eligibility requirements, which can result in varied patterns of dental visiting among residents (AIHW 2018). Oral health campaigns and policies can also make an impact. For example, water fluoridation coverage in Queensland has reduced since the Queensland Government transferred the decision whether to fluoridate water supplies from state to local governments in 2012, despite evidence that access to fluoridated drinking water has been shown to reduce tooth decay (Queensland Health 2015; NHMRC 2017).