Completion of treatment
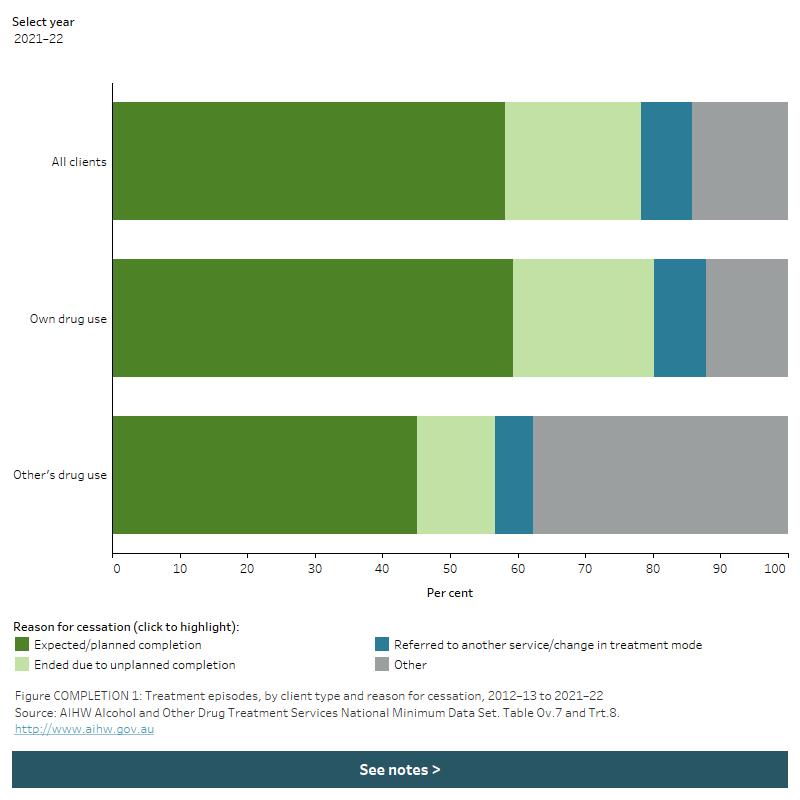
The stacked horizontal bar graph shows that most treatment episodes in 2021–22 ended with an expected/planned completion, regardless of client type. Treatment episodes provided to clients for their own drug use were more likely to end with an expected completion than were episodes provided to clients for someone else’s drug use 59.3% compared with 45.1%, respectively). 37.8% of episodes provided to clients for other’s drug use ended for other reasons, compared to 12.1% of episodes for clients’ own drug use. A filter allows the user to view data for different years.
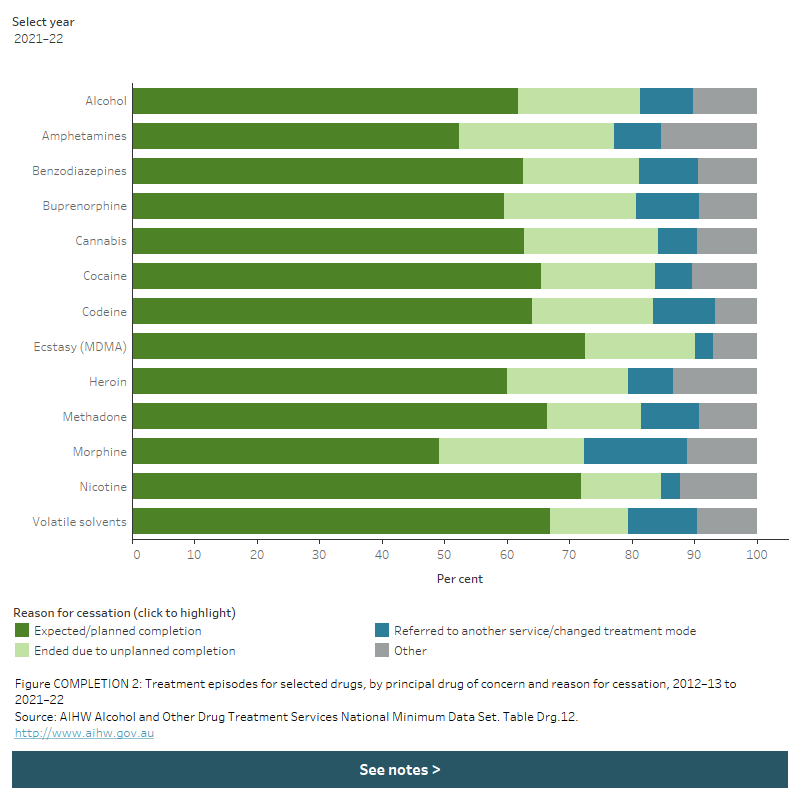
The stacked horizontal bar chart shows that expected/planned completion was the most common reason for cessation in treatment episodes for all selected principal drugs of concern in 2021–22. The proportion of episodes that ended with an expected completion ranged from 49.1% for morphine as the principal drug of concern to 72.5% for ecstasy (MDMA). A filter allows the user to view data for different years.