The onset of the COVID-19 pandemic has had an impact on Australia’s population and health care system in multiple ways, including on economic expenditure, mortality, disability, health workforce and disease surveillance. The next web page explores the impact of COVID-19 in Australia for people living with chronic kidney disease (CKD).
Data available on CKD across the COVID period are limited by the availability of data on the continuing pandemic period, as well as the lack of longer term data.
There will likely be long-term impacts of the COVID-19 pandemic on people with CKD, even on those who do not become infected with COVID-19, due to delays in care for chronic conditions such as CKD, diabetes and cardiovascular disease (Yende and Parikh, 2021).
Kidney transplants in Australia
Organ donation numbers and transplants have declined as a result of the COVID-19 pandemic (OTA 2021). In response to COVID-19, adult kidney transplant programs were suspended from 24 March 2020 to mid-May 2020.
Pauses in transplant surgery particularly affected those with CKD, as more than half of transplanted organs are kidneys. In 2020, there was an 18% drop in the number of kidney transplants from deceased donors compared with 2019 (704 and 857 transplants, respectively). 2021 saw a decrease of 6.8% compared with 2020 (656 transplants) (OTA 2020, 2021).
Donations from living donors are classified as elective surgery; therefore, pauses in elective surgery affected the number of transplants from living donors. There was a 24% drop in living kidney donors in 2020; in 2021, the number of living kidney donors rose by 12% compared with 2020 (202 and 182 donors) (OTA 2021).
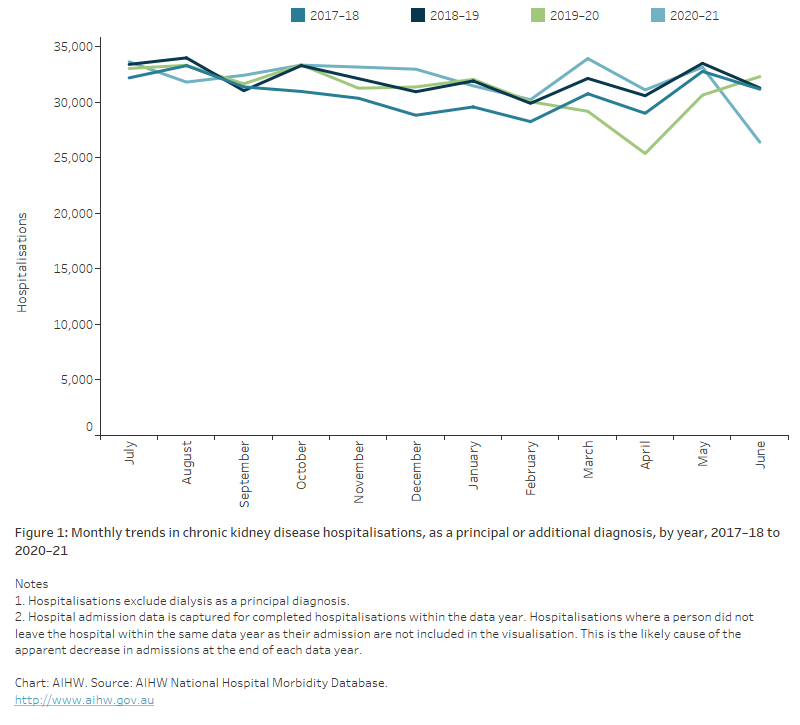
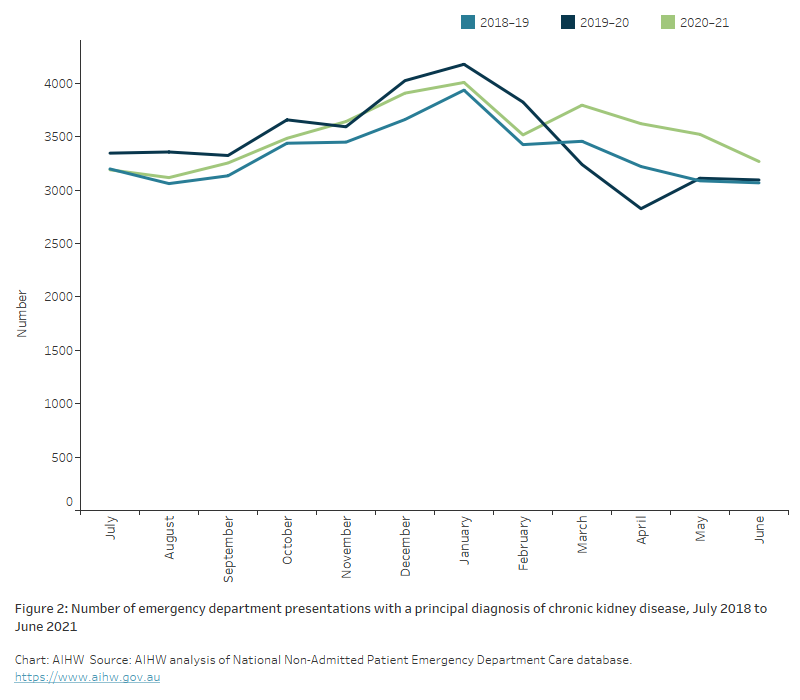
Chronic kidney disease hospitalisations
In 2020–21, there were over 4,700 hospitalisations involving a diagnosis of COVID-19 in Australia. Of these, 394 (8.4%) had CKD recorded on their hospital admission; 64 (16%) of these required a stay in the intensive care unit, 48 (12%) required continuous ventilatory support and 113 (29%) died in hospital, the third-highest death rate for comorbid conditions after chronic obstructive pulmonary disease and dementia. This includes type 2 diabetes (19%, 188 deaths) and cardiovascular disease (20%, 189 deaths), which are often comorbid with CKD. The death rate for people with CKD and COVID-19 was also higher than for people with multiple comorbid conditions who were hospitalised with COVID-19 (26%) and people with no comorbid conditions (4.7%) (AIHW 2022).
Hospital admissions for people with CKD fell sharply between March and April 2020, when lockdown measures were introduced nationwide by the Australian Government. In April 2020, CKD hospitalisations declined by 16% among males and by 18% among females, compared with figures for April 2019 (Figure 1(b)).