Antipsychotics and other medications dispensed to people with dementia
Figure 8.6 is a bar graph showing the percentage of people dispensed dementia-specific medications who were also dispensed other medications in 2021-22, by medication type and sex. The medications are grouped at the highest Anatomical Therapeutic Chemical classification level. Around three-quarters of men and women who were dispensed scripts for dementia-specific medications were also dispensed medications for the cardiovascular system, and nervous system. Men were less likely than women to be dispensed nervous system medications, anti-infectives for systemic use, musculoskeletal system medications, and systemic hormonal preparations. However, men were more likely than women to be dispensed medications for the cardiovascular system, alimentary tract and metabolic, blood and blood forming organs, sensory organs, dermatologicals, respiratory system, genitourinary system and sex hormones and for antineoplastic and immunomodulating agents.
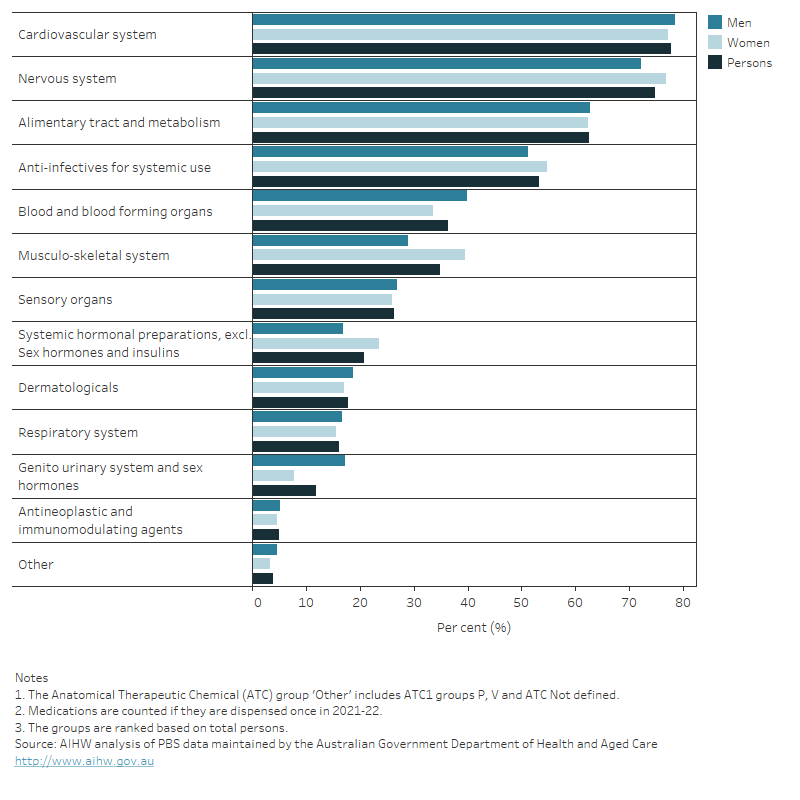
Figure 8.7 is a bar graph showing the percentage of people dispensed dementia-specific medications who were also dispensed other medications in 2021-22, by medication type, age and sex. The medications are grouped at the second highest Anatomical Therapeutic Chemical classification level. Over half (52%) were dispensed scripts for psychoanaleptics, which are used for depression and other neurological and mental disorders. Half of people were dispensed scripts for antibacterials for systemic use, which are used to treat a range of bacterial infections. Men were more likely than women to be dispensed scripts for lipid modifying agents, agents acting on the renin-angiotensin system, psycholeptics, antithrombotic agents and drugs used in diabetes. However, women were more likely than men to be dispensed scripts for psychoanaleptics, antibacterials, drugs for acid related disorders, analgesics, and opthalmologicals. While the majority of medications were dispensed to greater proportions of older people who were dispensed dementia-specific medications, psychoanaleptics were dispensed to a larger proportion of those with younger onset dementia (aged under 65) compared with people aged 85 and over.
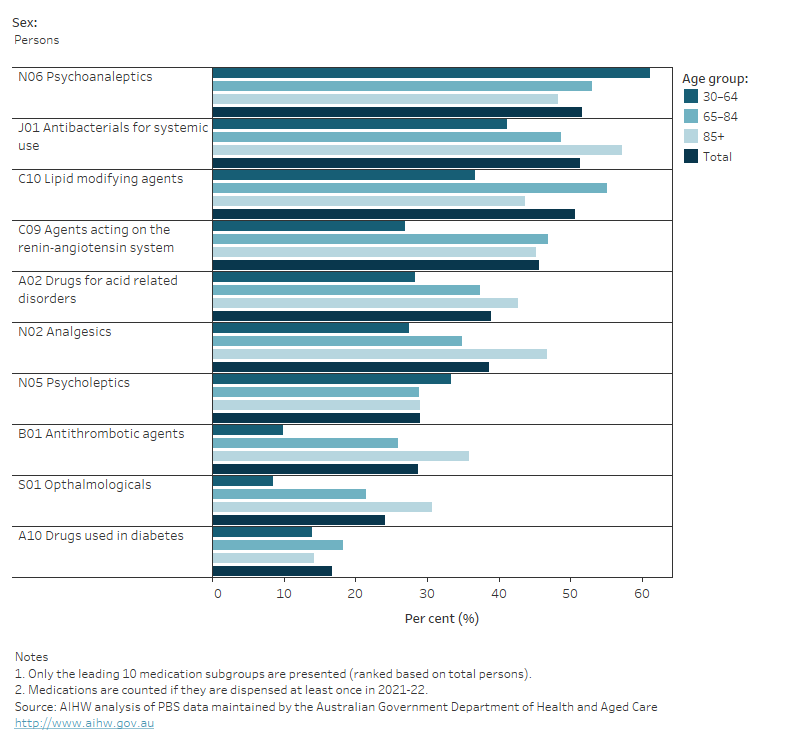
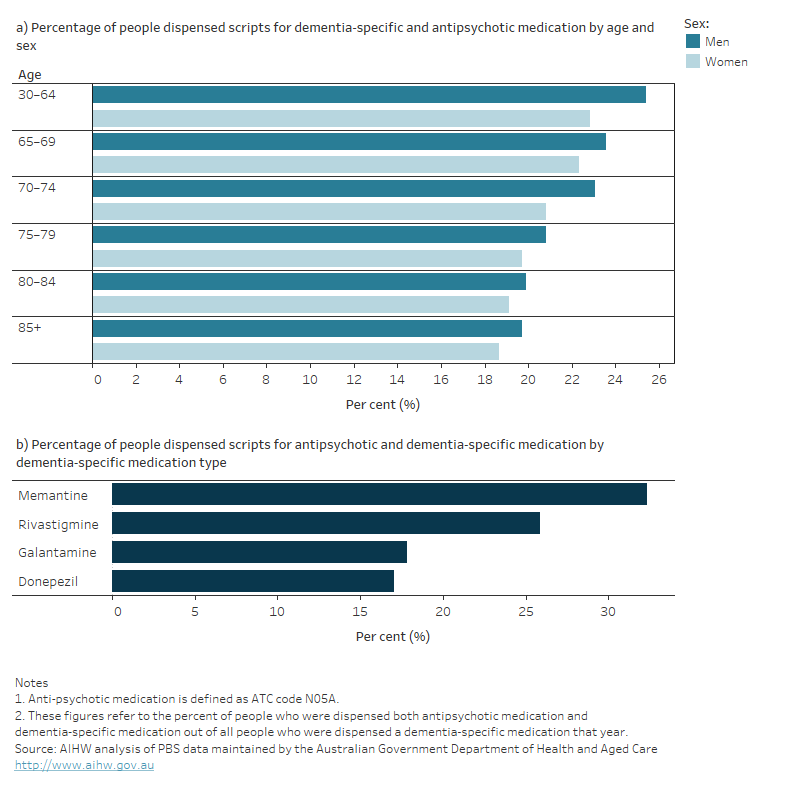
Figure 8.8 shows two bar graphs depicting breakdowns of the percentage of people who were dispensed prescriptions for dementia-specific medications and also dispensed prescriptions for antipsychotic medications at least once in 2021-22. The first graph shows the percentage by age and sex and the second graph shows the percentage by the type of dementia-specific medication they were dispensed. Overall, around one-fifth of people who were dispensed prescriptions for dementia-specific medications were also dispensed antipsychotic medications. The proportion within each age group who were prescribed scripts for antipsychotics decreased slightly with age. Men were relatively more likely to be dispensed scripts for antipsychotics than women in each age group. Antipsychotics were more likely to be dispensed to people who were also taking Memantine, which is the only dementia-specific medication prescribed for moderately severe to severe Alzheimer’s disease.