Health risk factors and behaviours
Figure RISK.1: Consumption of fruit and vegetables, by disability status, age group and sex, 2017–18
Stacked column chart showing whether people, with and without disability, met national guidelines for fruit and vegetable consumption. The reader can select to display the chart by disability status; by age group 2–64, 65 and over or all ages; by sex; and by whether the person met the guidelines for fruit consumption, for vegetable consumption and for both fruit and vegetable consumption. The chart shows people with and without disability were less likely to meet the guidelines for vegetable consumption than for fruit consumption, regardless of sex, age or level of disability.
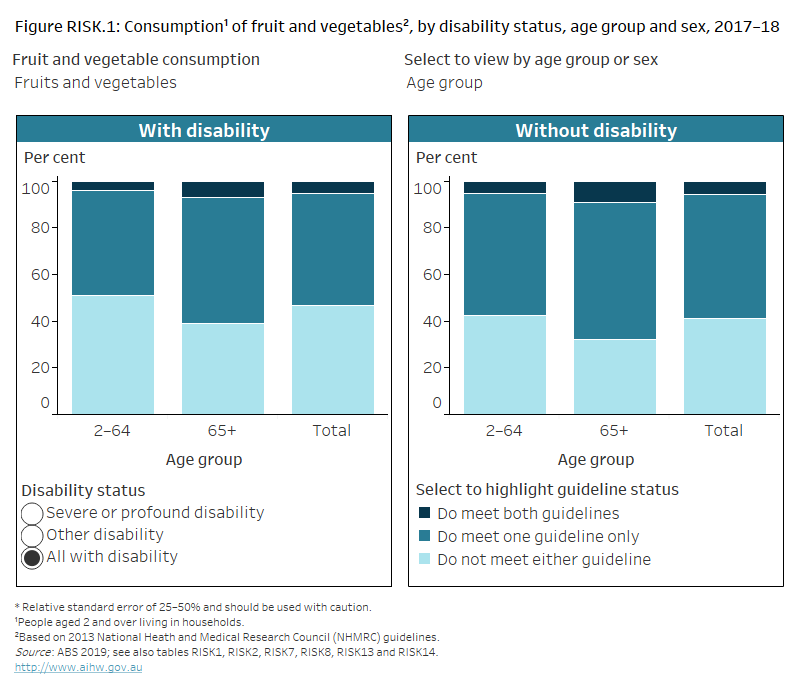
Figure RISK.2: Consumption of sugar-sweetened and diet drinks, by disability status, age group and sex, 2017–18
Stacked column chart showing whether people, with and without disability, daily consume sweetened drinks. The reader can select to display the chart by disability status; by age group 2–64, 65 and over, or all ages; by sex; and by drink type including sugar-sweetened or diet drinks. The chart shows males with disability are more likely (16%) to consume sugar-sweetened drinks daily than females (8%).

Figure RISK.3: Body Mass Index (BMI), by disability status, age group and sex,
2017–18
Stacked column chart showing 3 categories of body mass index for people with and without disability. The reader can select to display the chart by disability status; by age group 2–64, 65 and over, or all ages; and by sex. The chart shows females with disability are more likely (69%) to be overweight or obese than those without disability (48%).
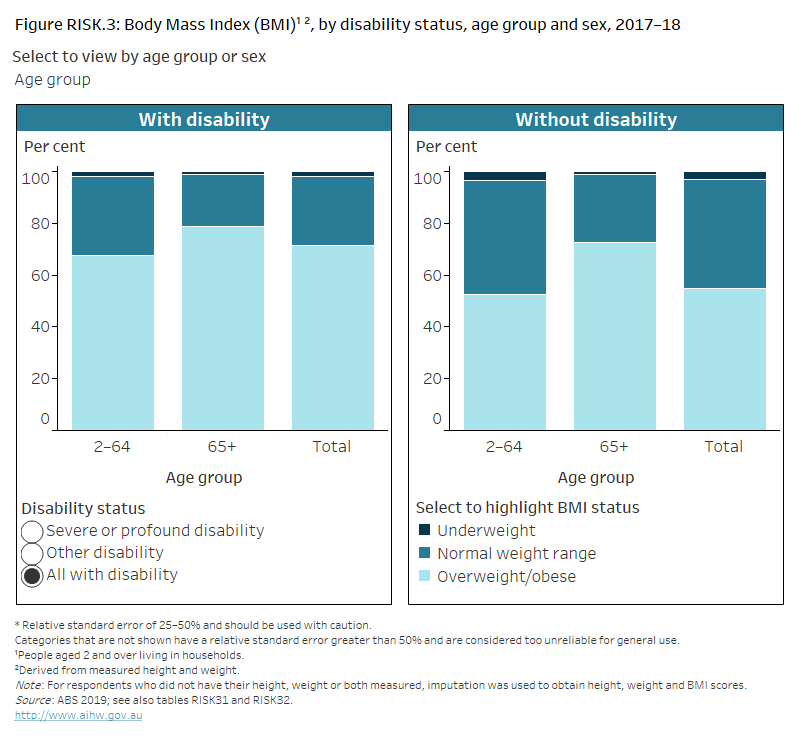
Figure RISK.4: Waist circumference, by disability status, age group and sex,
2017–18
Stacked column chart showing 3 categories of risk of developing chronic conditions, based on waist circumference, for adults with and without disability. The reader can select to display the chart by disability status; by age group 18–64; 65 and over, or all adults; and by sex. The chart shows men with disability are more likely (51%) to have substantially increased risk of developing chronic conditions than those without disability (32%).
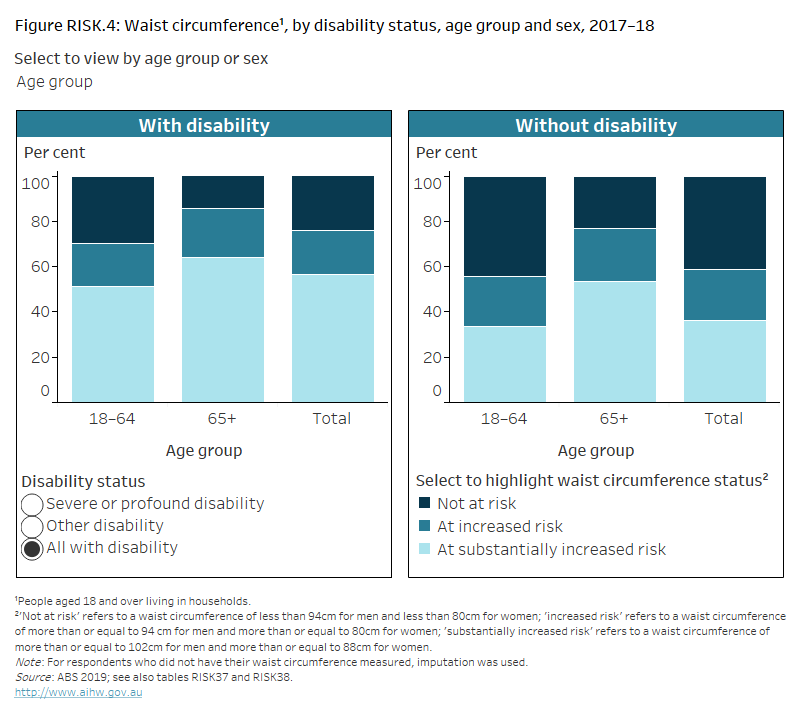
Figure RISK.5: Physical activity, by disability status, age group and sex, 2017–18
Stacked column chart showing whether people with and without disability met national guidelines for physical activity. The reader can select to display the chart by disability status; by age group 15–64, 65 and over, or all ages; and by sex. The chart shows people with disability aged 65 and over are less likely (17%) to meet the physical activity guidelines than those aged 15–64 (35%).
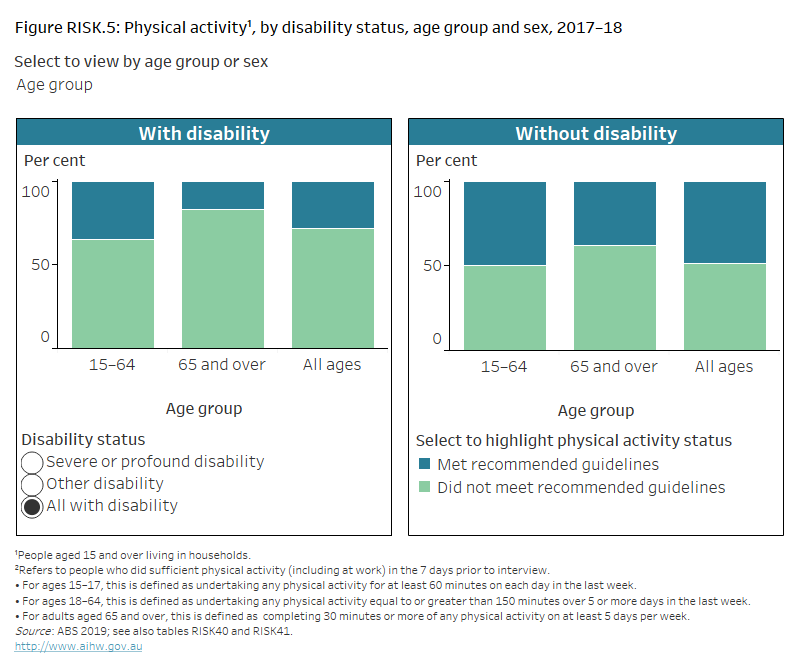
Figure RISK.6: Blood pressure status, by disability status, age group and sex,
2017–18
Column chart showing 3 categories of blood pressure status for adults with and without disability. The reader can select to display the chart by blood pressure category, including controlled blood pressure, uncontrolled blood pressure and all with hypertension, by disability status; by age group 18–64, 65 and over, or all adults; and by sex. The chart shows adults with disability aged 65 and over are more likely (78%) to have hypertension than those aged 18–64 (38%).
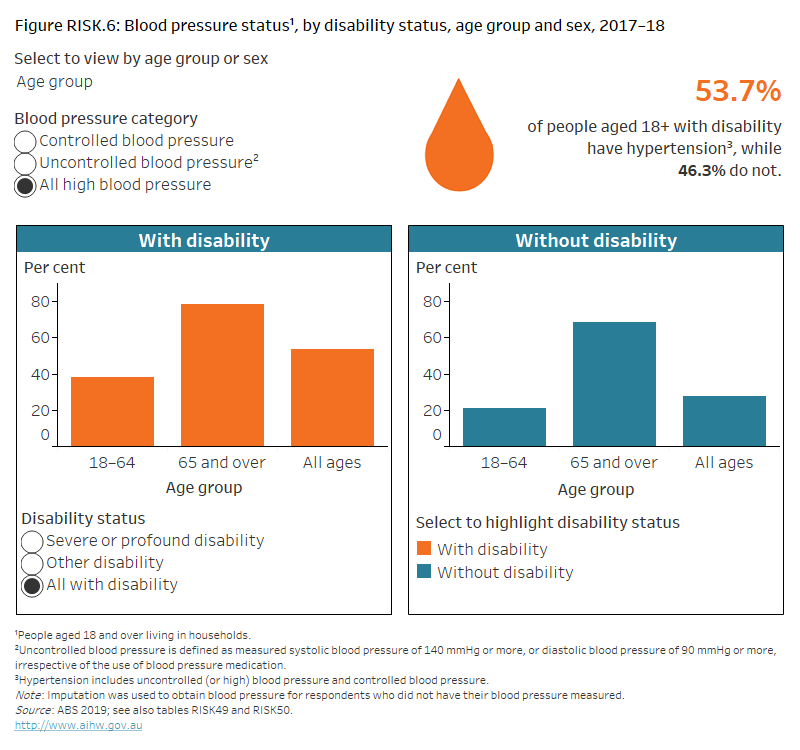
Figure RISK.7: Daily tobacco smoking status, by disability status, age group and sex, 2017–18
Stacked column chart showing whether people with and without disability currently smoke daily. The reader can select to display the chart by disability status; by age group15–64, 65 and over, or all ages; and by sex. The chart shows people with disability aged 15–64 are more likely (25%) to smoke daily than those without disability (13%).
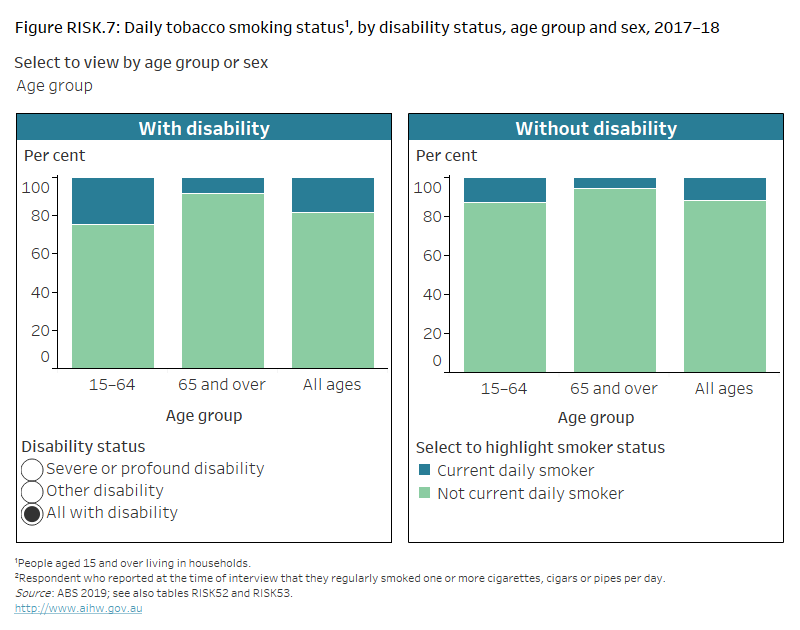
Figure RISK.8: Lifetime alcohol risk, by disability status, age group and sex, 2017–18
Column chart showing the proportion of people with and without disability who exceed the lifetime alcohol risk guidelines. The reader can select to display the chart by disability status; by age group 15–64, 65 and over, or all ages; and by sex. The chart shows females with severe or profound disability are less likely (3%) to drink more than 2 standard drinks per day than those without disability (9%).
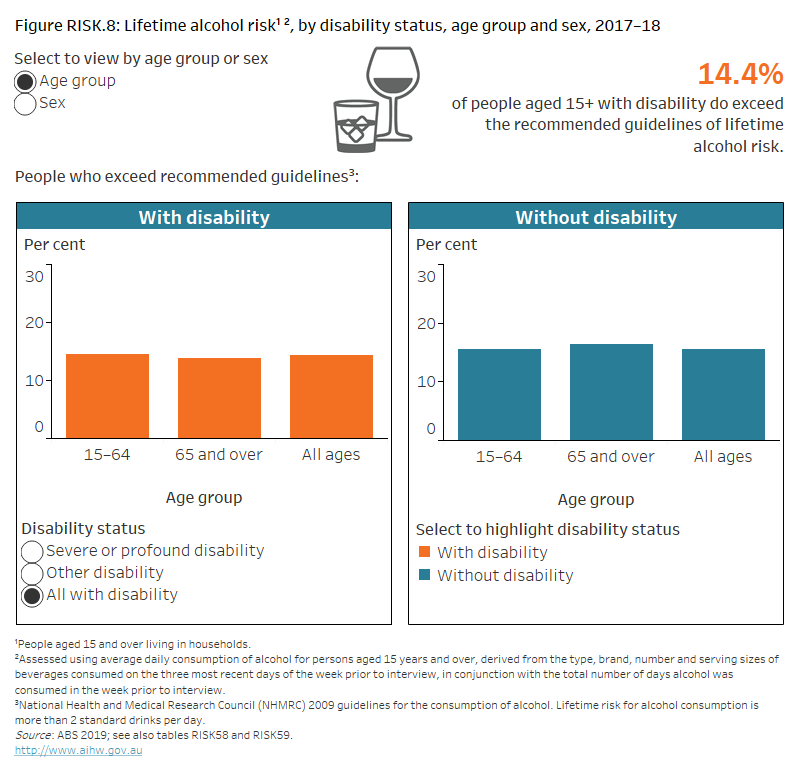
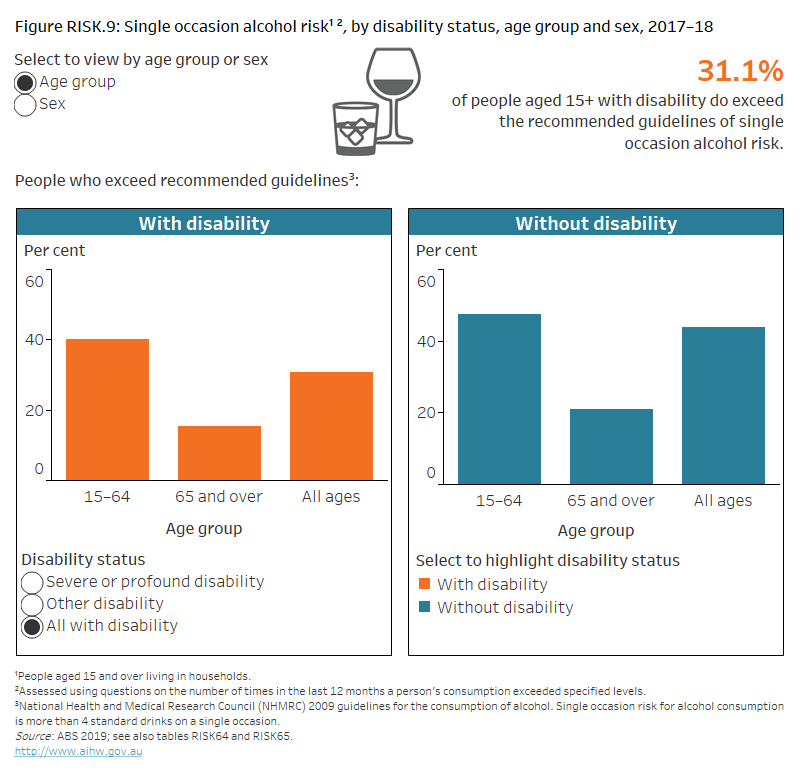
Figure RISK.9: Single occasion alcohol risk, by disability status, age group and sex, 2017–18
Column chart showing the proportion of people with and without disability who exceed the single occasion alcohol risk guidelines. The reader can select to display the chart by disability status; by age group 15–64, 65 and over, or all ages; and by sex. The chart shows people with disability aged 15–64 are less likely (40%) to drink at risky levels on a single occasion than those without disability (48%).