Peripheral arterial disease
Page highlights:
How many Australians have peripheral arterial disease?
- Peripheral arterial disease has been estimated to affect up to 10% of patients in primary care settings, and over 20% when studied in populations aged 75 and over.
- In 2020–21, there were around 59,100 hospitalisations where peripheral arterial disease was recorded.
- The age-standardised rate of hospitalisations of peripheral arterial disease declined by 47% between 2000–01 and 2020–21.
 Peripheral arterial disease was the underlying cause of 1,900 deaths in 2021 — equating to 1.1% of all deaths.
Peripheral arterial disease was the underlying cause of 1,900 deaths in 2021 — equating to 1.1% of all deaths.
What is peripheral arterial disease?
Peripheral arterial disease (PAD), also known as peripheral vascular disease, is the reduced circulation of blood to a body part outside of the heart or brain.
PAD occurs most commonly in the arteries leading to the legs and feet. It is often the result of atherosclerosis, where fatty deposits build up in the walls of arteries. In some people it does not present any symptoms, while others may experience pain at rest or while walking. In severe cases it can lead to tissue loss, and the amputation of a limb.
A notable form of PAD is abdominal aortic aneurysm. This is abnormal widening of the aorta (the main artery leading from the heart) below the level of the diaphragm. It can be a life-threatening condition if the arterial wall ruptures. Surgery is necessary in some cases.
Tobacco smoking and diabetes are primary risk factors for PAD. Type 2 diabetes in people with PAD can accelerate atherosclerosis, and increase the risk of amputation, of other cardiac events such as stroke, and death.
Other PAD risk factors include abnormal blood lipids, high blood pressure, overweight or obesity, and family history of the disease. PAD has increasingly been associated with other chronic conditions such as atrial fibrillation, heart failure, obstructive sleep apnoea and chronic kidney disease.
How many Australians have peripheral arterial disease?
Currently, there are no national data on the number of Australians living with PAD.
PAD has been estimated to affect up to 10% of patients in primary care settings, and over 20% when studied in populations aged 75 and over (Aitken 2020, Conte & Vale 2018). Over half of all people with PAD show no symptoms, leading to under-diagnosis and under-treatment.
Hospitalisations
Peripheral arterial disease often occurs alongside other chronic diseases, so both the principal and additional diagnoses of PAD should be counted when estimating its contribution to hospitalisations.
There were around 59,100 hospitalisations where PAD was recorded as the principal and/or additional diagnosis in 2020–21, at a rate of 230 per 100,000 population. This represents 0.5% of all hospitalisations in Australia.
PAD was recorded as the principal diagnosis in 56% (33,200) of these hospitalisations.
Over half of all hospitalisations where PAD was the principal diagnosis (60%) were for atherosclerosis of the peripheral arteries, while abdominal aortic aneurysm accounted for a further 9%. The remainder was comprised largely of embolisms and other aneurysms.
Age and sex
Where PAD was recorded as the principal and/or additional diagnosis, hospitalisation rates:
- were overall twice as high for males as females, after adjusting for differences in the age structure of the populations. Age-specific rates were higher among males than females in all age groups, except for age 35–44
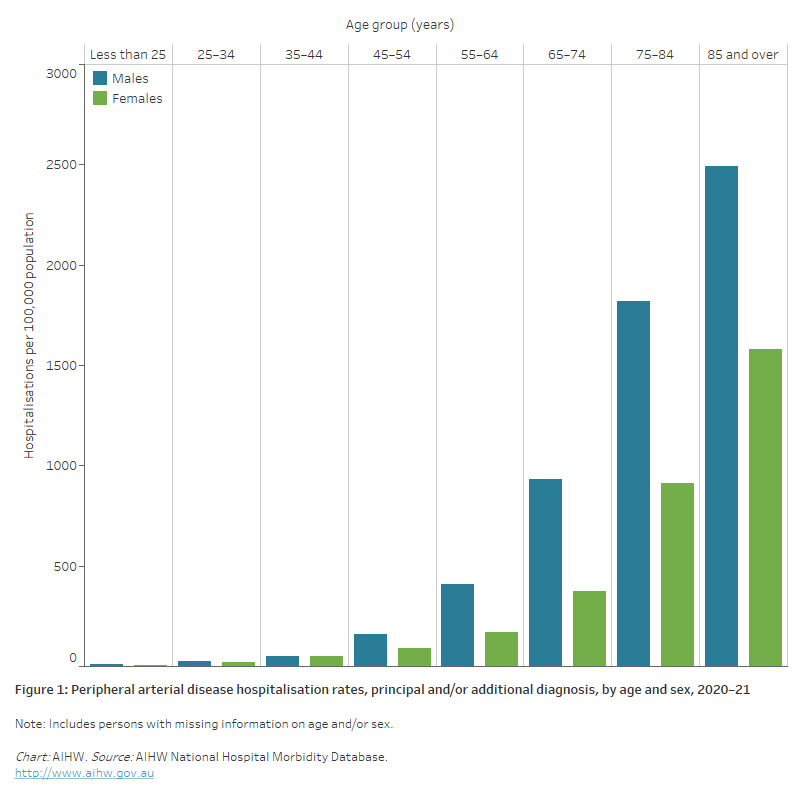
- increased with age, with rates highest for males and females aged 85 and over – at least 1.4 times as high as those aged 75–84 (Figure 1).
Figure 1: Peripheral arterial disease hospitalisation rates, principal and/or additional diagnosis, by age and sex, 2020–21
The bar chart shows in 2020–21, peripheral arterial disease hospitalisation rates were highest among males and females aged 85 and over (2,500 and 1,600 per 100,000 population, respectively).
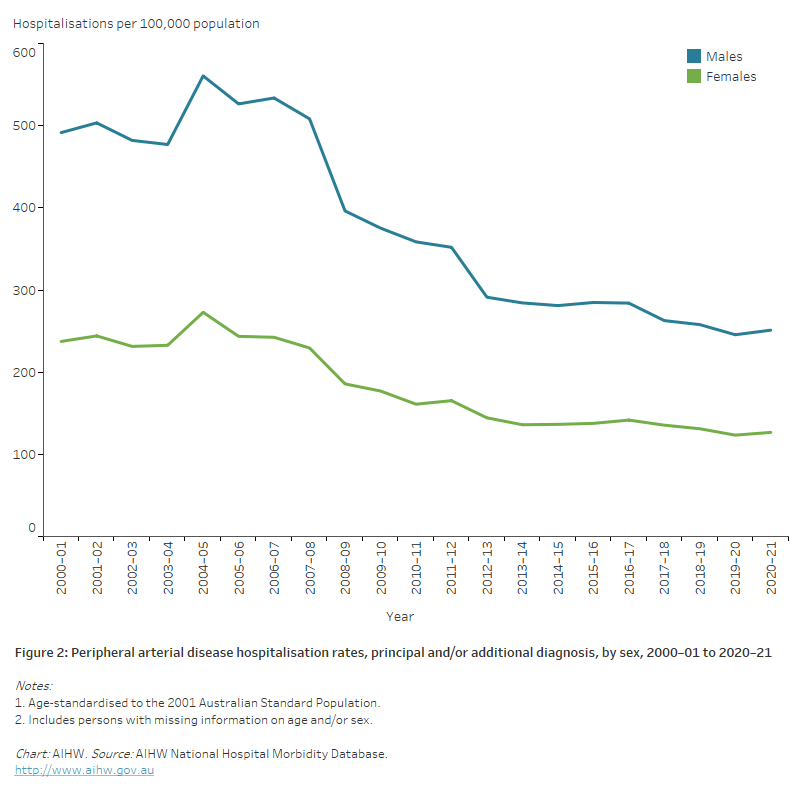
The line chart shows that age-standardised peripheral arterial disease hospitalisation rates declined between 2000–01 and 2020–21, from 492 to 251 and 237 to 127 per 100,000 population for males and females, respectively.
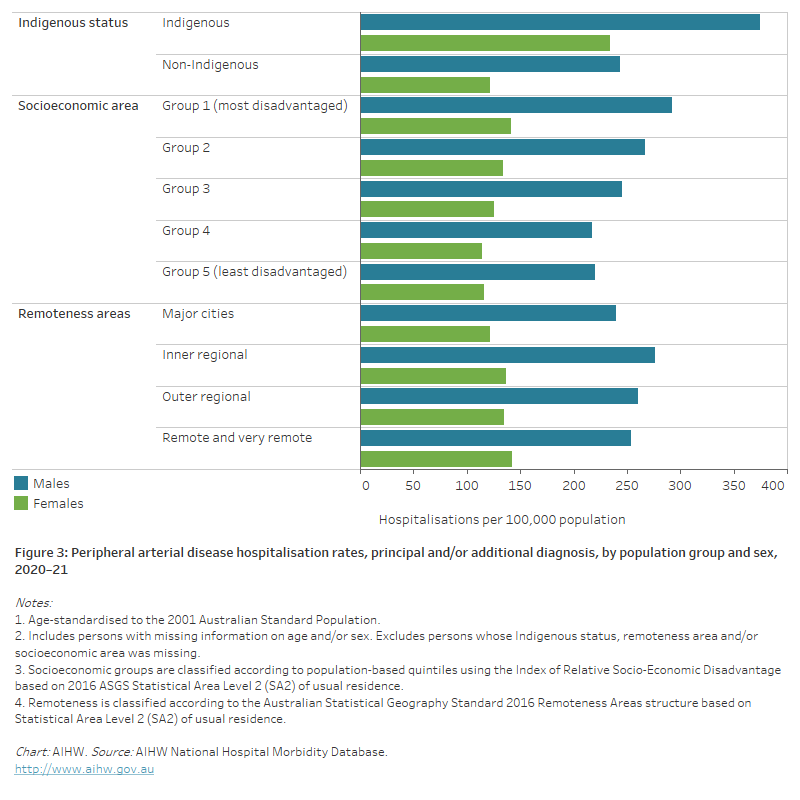
The horizontal bar chart shows that age-standardised peripheral arterial disease hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas and people living in Remote and very remote areas.
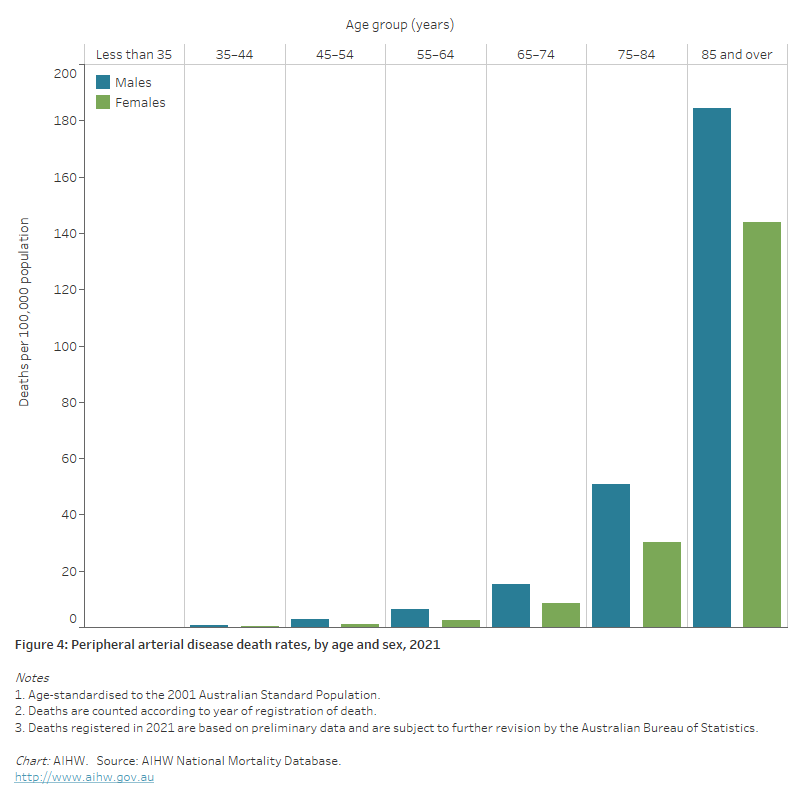
The bar chart shows the age-standardised peripheral arterial disease death rates in 2021 were highest among males and females aged 85 and over (184 and 144 per 100,000 population, respectively).
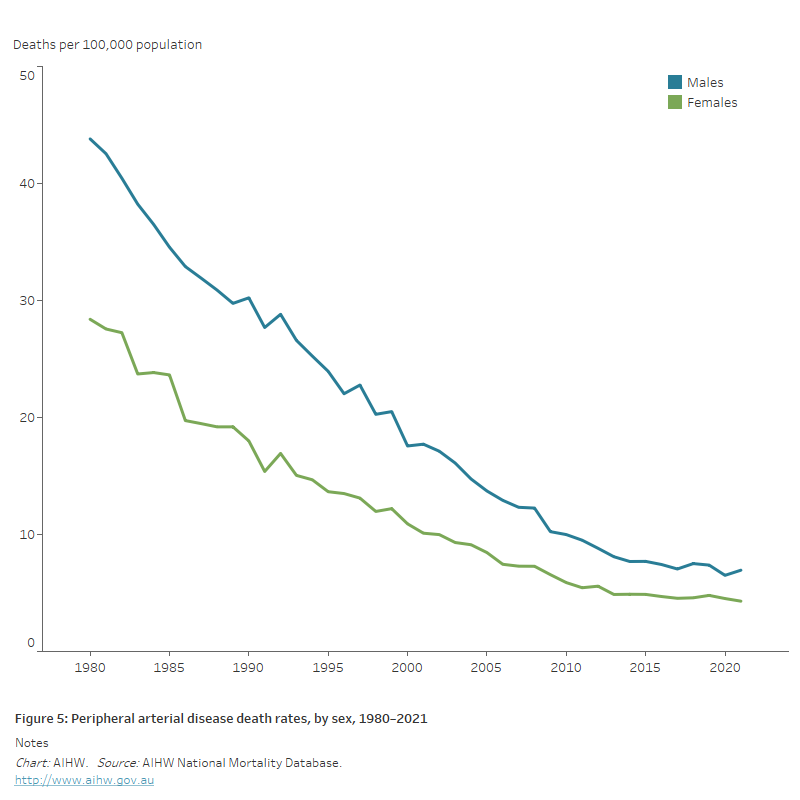
The line chart shows the decline in age-standardised peripheral arterial disease death rates between 1980 and 2021 for both males and females, from 44 to 6.9 and 28 to 4.3 per 100,000 population, respectively.
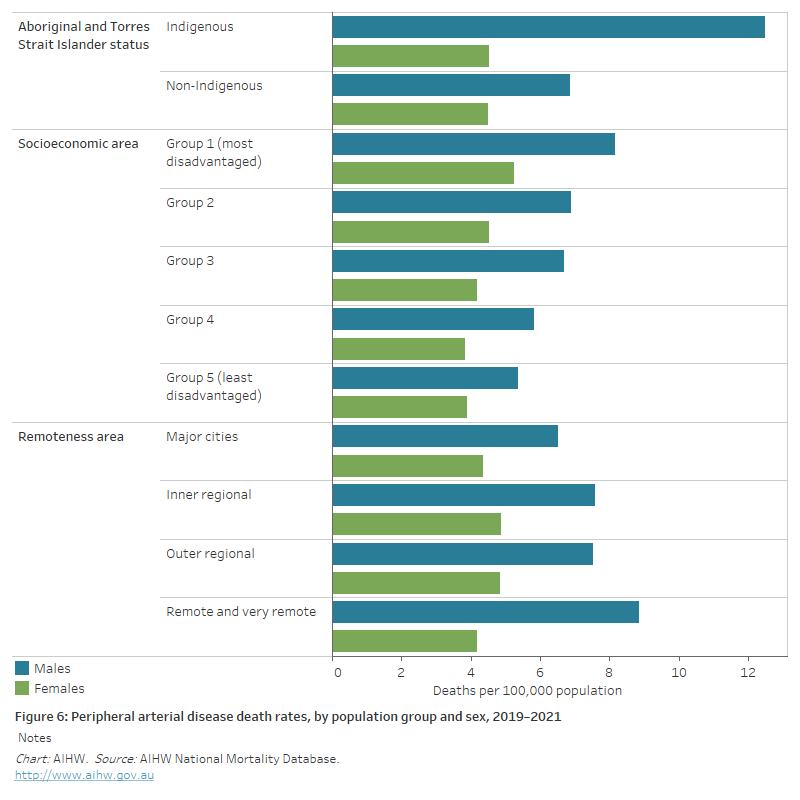
The horizontal bar chart shows in 2019–2021 age-standardised peripheral arterial disease death rates were higher among Indigenous Australians and people living in the lowest socioeconomic areas but did not differ significantly by remoteness area.