Coronary heart disease
Page highlights:
How many Australians have coronary heart disease?
- In 2017–18, an estimated 580,000 Australians aged 18 and over (3.1% of the adult population) had coronary heart disease at some time in their lives.
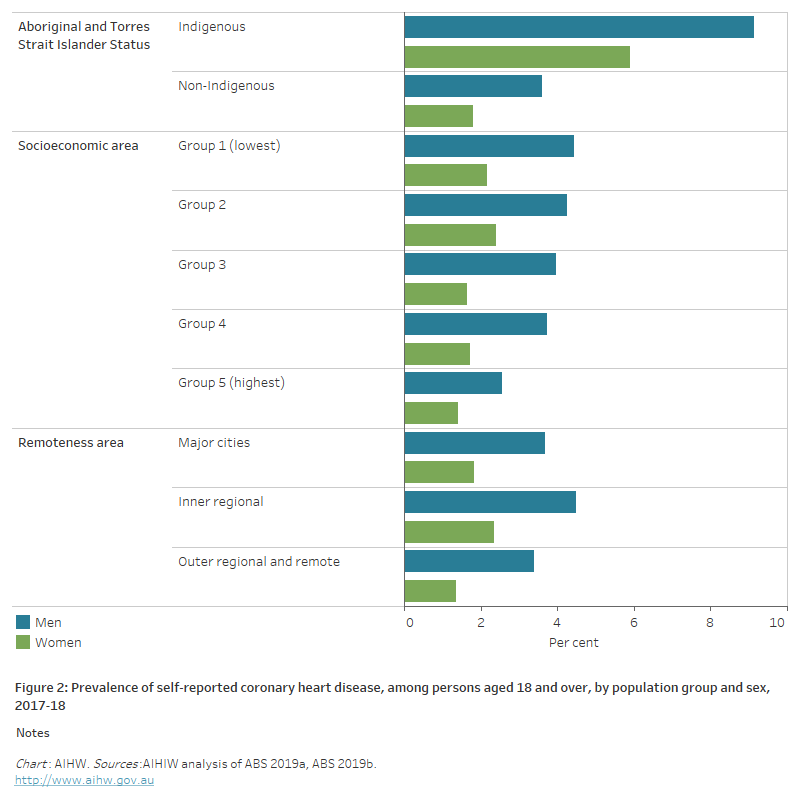
- The rate of coronary heart disease among Indigenous adults was more than twice that of non-Indigenous adults.
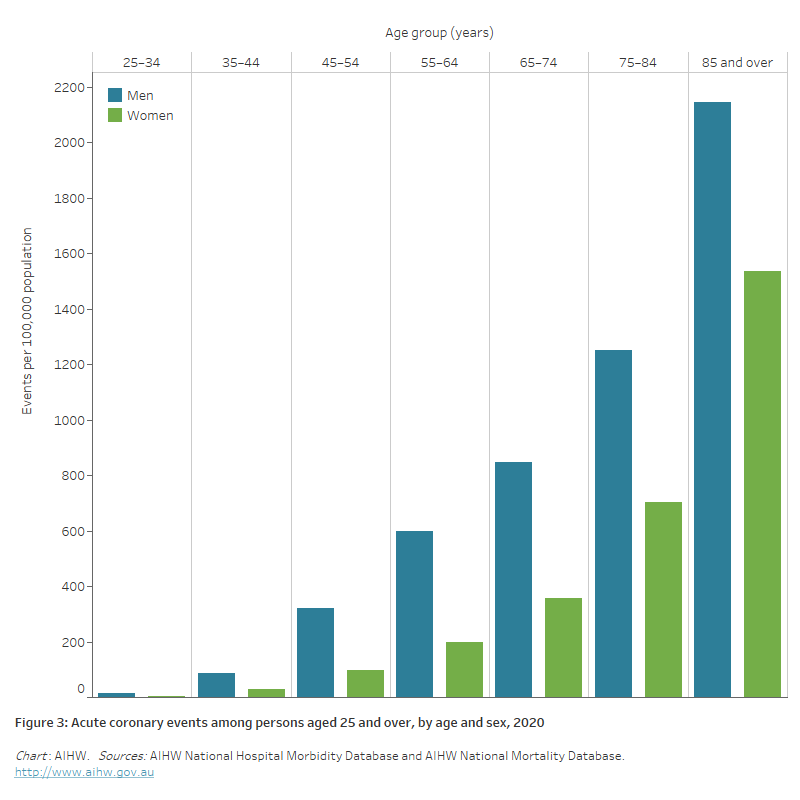
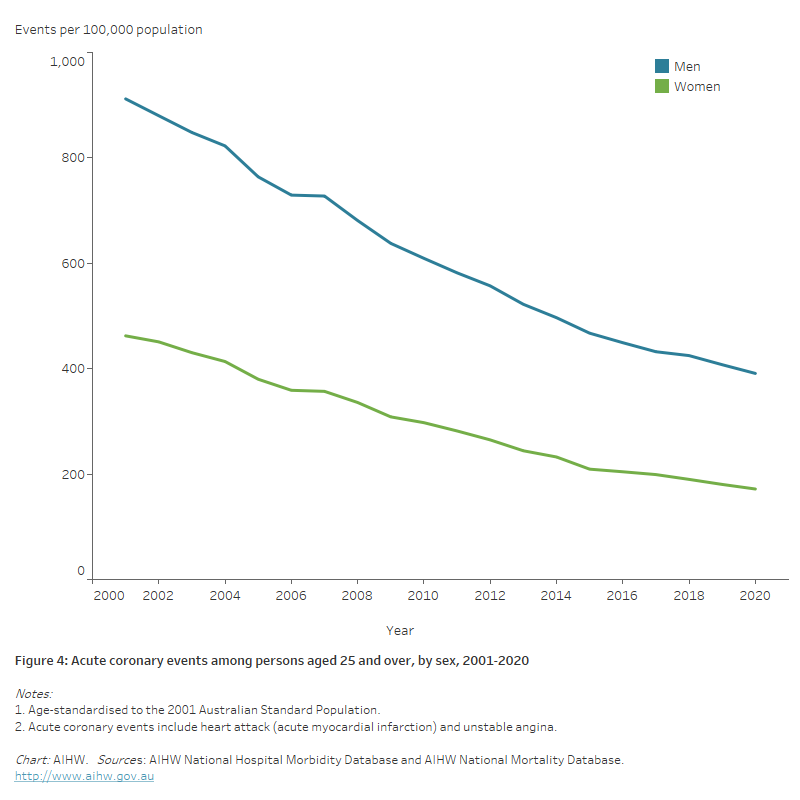
- In 2020, there were an estimated 56,700 acute coronary events among people aged 25 and over–equivalent to around 155 events every day.
- In 2020–21, there were 160,000 hospitalisations where coronary heart disease was recorded as the principal diagnosis, equivalent to 1.4% of all hospitalisations, and 27% of all cardiovascular disease hospitalisations in Australia.
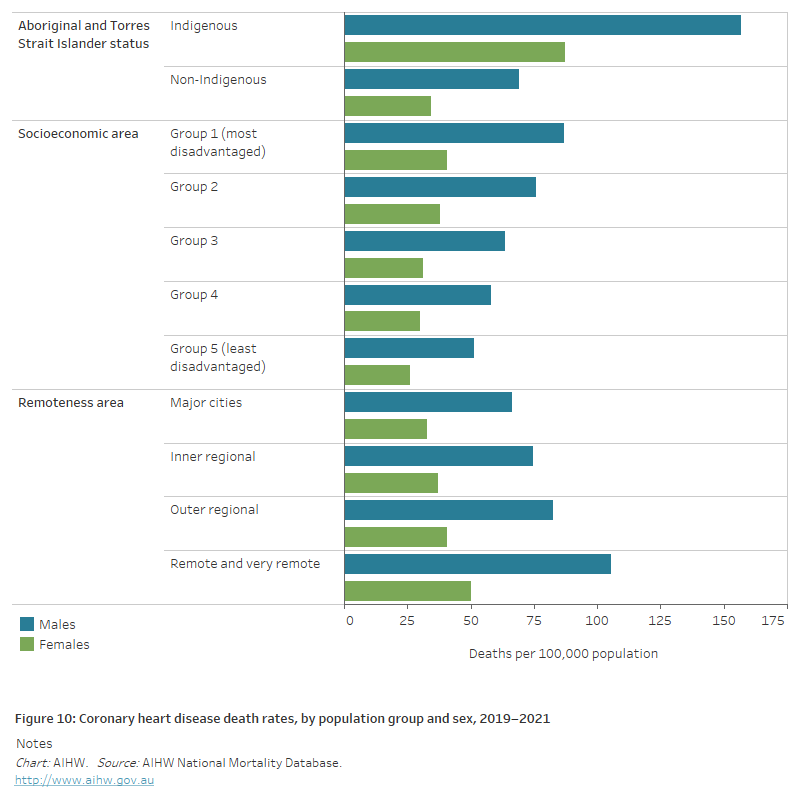
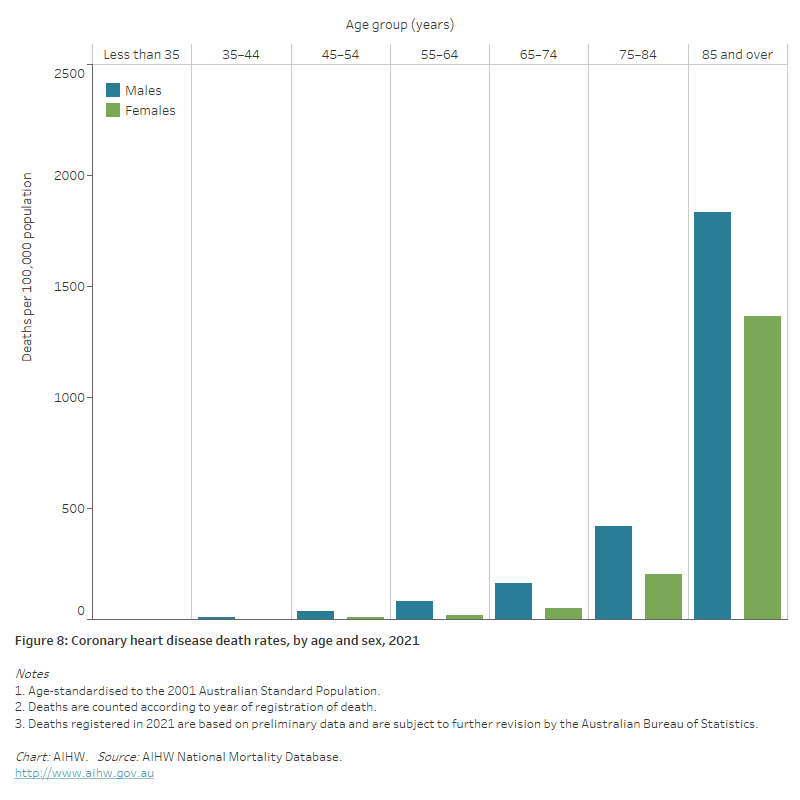
 In 2021, coronary heart disease was the underlying cause of 17,300 deaths (10% of all deaths).
In 2021, coronary heart disease was the underlying cause of 17,300 deaths (10% of all deaths).
Coronary heart disease (CHD), also known as ischaemic heart disease, is the most common cardiovascular disease. There are 2 main clinical forms – heart attack and angina.
![]()
Heart attack – or acute myocardial infarction (AMI) – is a life-threatening event that occurs when a blood vessel supplying the heart is suddenly blocked, threatening to damage the heart muscle and its functions. STEMI (ST segment elevation myocardial infarction) is the most serious type of heart attack. It is almost always caused by a complete blockage of a major coronary artery, leading to a long interruption of blood supply. NSTEMI (Non-ST segment elevation myocardial infarction) is characterised by a partially blocked artery, which severely reduces blood flow.
Angina is chest pain caused by reduced blood flow to the heart. With stable angina, periodic episodes of chest pain occur when the heart has a temporary deficiency in blood supply. Unstable angina is an accelerating pattern of chest discomfort, and is the more dangerous form due to a changing severity in partial coronary artery blockages. It is treated in a similar manner to heart attack.
Both heart attack and unstable angina are sudden, severe life-threatening events. They are part of a continuum of acute coronary heart diseases, and are together described as acute coronary syndrome (ACS).
How many Australians have coronary heart disease?
An estimated 580,000 Australians aged 18 and over (3.1% of the adult population) had CHD at some time in their lives, based on self-reported data from the ABS 2017–18 National Health Survey (AIHW analysis of ABS 2019).
Of those with CHD, 227,000 had experienced angina while 430,000 had a heart attack or another form of CHD, noting that a person may report more than 1 disease.
Age and sex
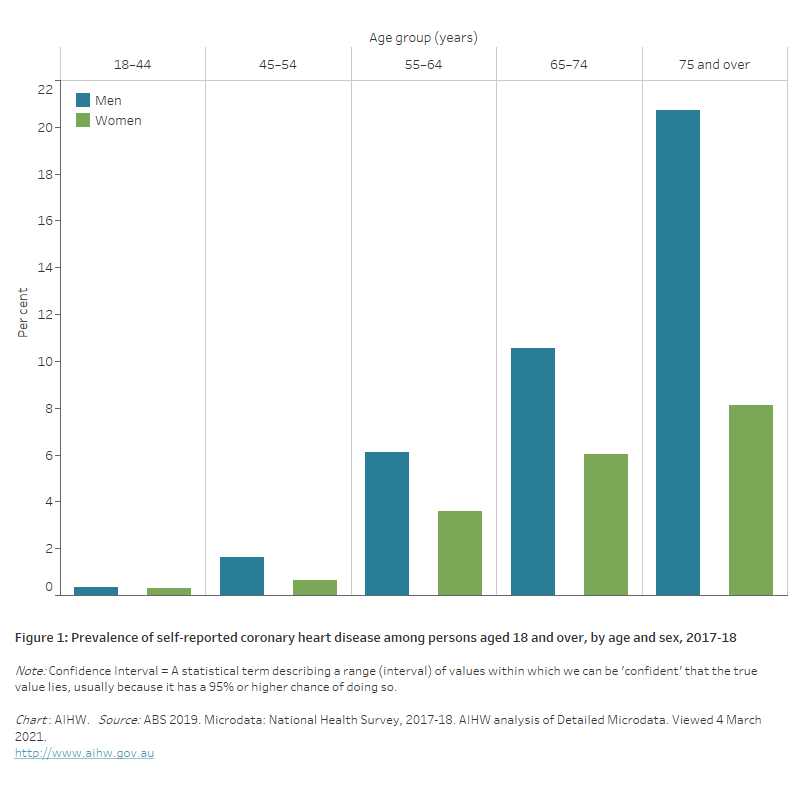
- After adjusting for age, a higher percentage of men (3.8%) than women (1.9%) were estimated to have CHD in 2017–18.
- CHD occurred more commonly in older age groups, increasing from 1.1% in those aged 45–54 to 14% among those aged 75 and over.
- At age 75 and over, there is a marked difference between men (21%) and women (8.1%) reporting having CHD (Figure 1).
Figure 1: Prevalence of self-reported coronary heart disease among persons aged 18 and over, by age and sex, 2017–18
The bar chart shows the prevalence of self-reported coronary heart disease by age group in 2017–18. Rates were highest among men and women aged 75 and over (21% and 8.1%).
The horizontal bar chart shows that the prevalence of self-reported coronary heart disease in 2017–18 was higher among Indigenous Australians and people living in socioeconomically disadvantaged areas, but did not vary significantly by remoteness areas.
The bar chart shows rates of acute coronary events by age group in 2020. These were highest among men and women aged 85 and over (2,100 and 1,500 per 100,000 population).
The line chart shows declines in age-standardised rates of acute coronary events between 2001 and 2020, from 912 to 391 per 100,000 population for men aged 25 and over, and from 462 to 172 for women.
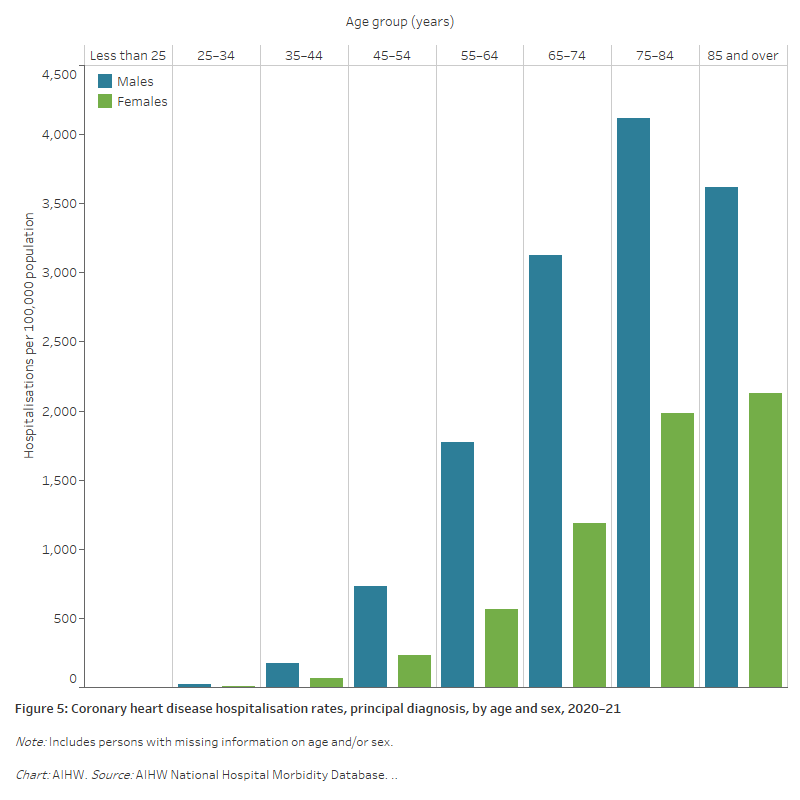
The bar chart shows coronary heart disease hospitalisation rates by age group in 2020–21. Rates were highest among males aged 75–84 (4,100 per 100,000 population) and females aged 85 and over (2,100 per 100,000 population).
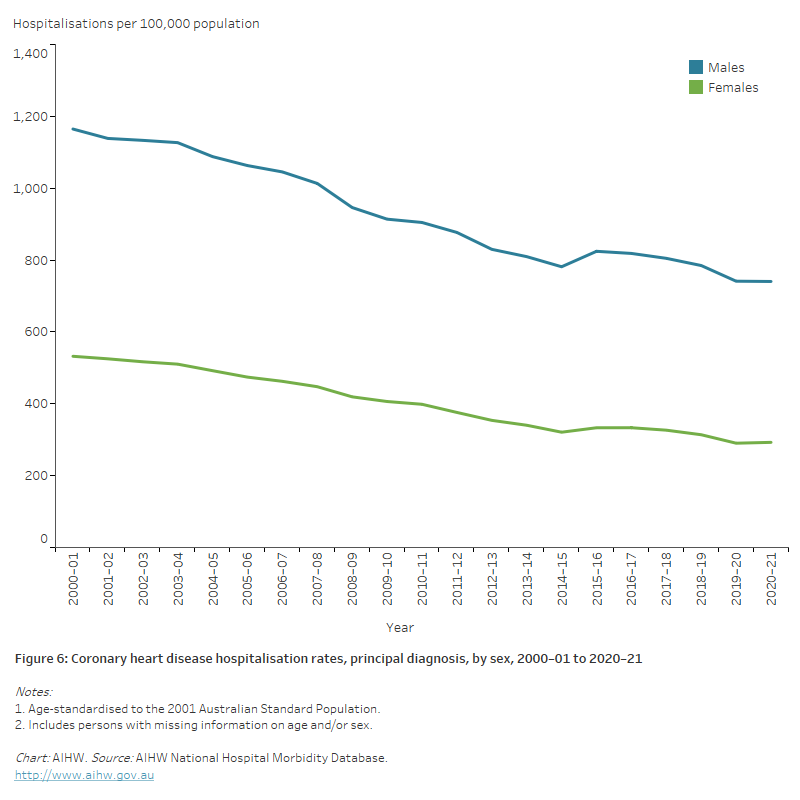
The line chart shows the decline in age-standardised rates of coronary heart disease hospitalisations between 2000–01 and 2020–21, from 1,165 to 740 per 100,000 population for males, and from 532 to 293 for females.
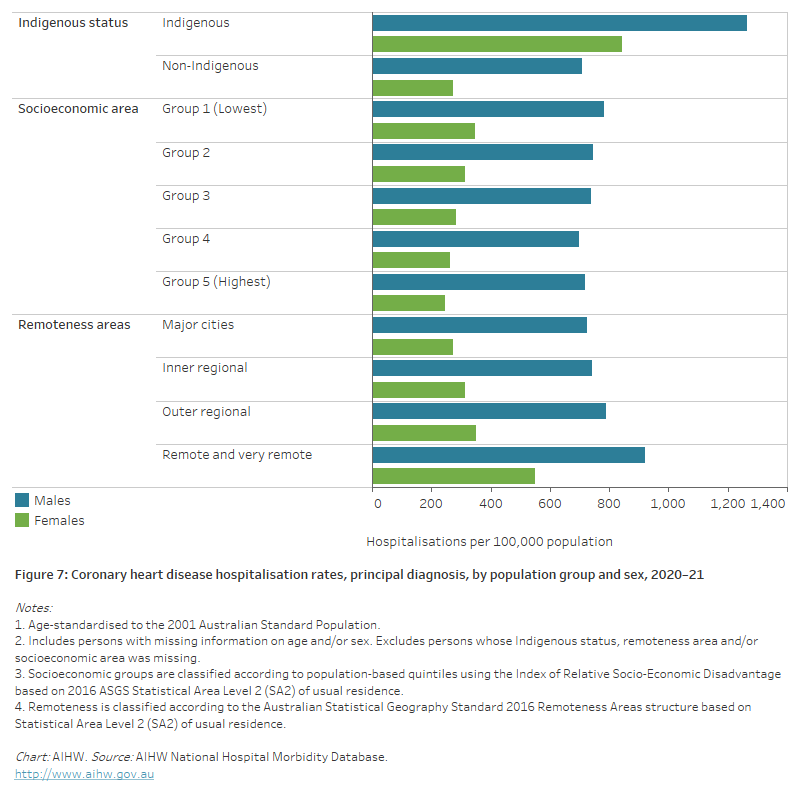
The horizontal bar chart shows that male and female coronary heart disease hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.
The bar chart shows coronary heart disease death rates by age groups in 2019. Rates were highest among men and women aged 85 and over (1,926 and 1,462 per 100,000 population).
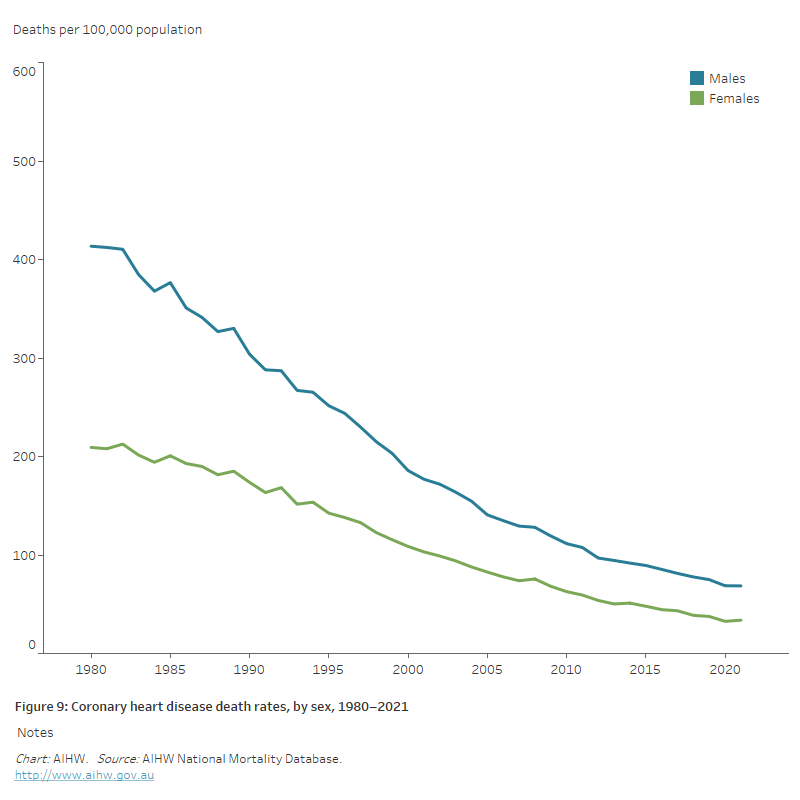
The line chart shows the decline in age-standardised coronary heart disease death rates between 1980 and 2019, from 414 to 73 per 100,000 population for males and from 209 to 37 for females.
The horizontal bar chart shows that coronary heart disease death rates in 2017–2019 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.