
Summary
Each year, there are around 6,500 hospitalisations for injuries known to be related to family and domestic violence (FDV) – encompassing violence that occurs between family members, and violence that occurs between intimate partners (AIHW 2021d). Through the use of longitudinal, national linked hospital and death data from the National Integrated Health Services Information Analysis Asset (NIHSI AA), this project examines, in detail, FDV hospital stays (defined as continuous periods of acute care hospitalisation) that occurred from 2010–11 to 2018–19, including the number of repeat stays, length of time between stays, injuries, diagnoses and the relationship of perpetrator to victim. For this population, it also examines hospital stays for other types of assault, hospital stays for any reason (all cause hospital stays), emergency department presentations and deaths.
To assist with interpretation of the results, analyses are also presented for a comparison group of people who had a hospital stay in the period (matched on age, sex, Indigenous status, year of contact and remoteness area). The comparison of these 2 groups enhances the understanding of the hospital interaction profile for those who experience FDV, those who are at risk of further hospital stays, and the identification of potential undisclosed cases of FDV.
This work increases understanding in how linked data, like the NIHSI AA, can be used to examine service use and outcomes for people experiencing FDV, including the possible role this analysis can have in informing potential service intervention opportunities.
This report examined public hospital data for all Australian jurisdictions except Western Australia and the Northern Territory over the period 2010–11 to 2018–19. The FDV group is anyone who had a FDV stay from 2010–11 to 2017–18, but analysis includes stays that occurred in 2018–19. Over this time period, there were 34,416 hospital stays due to FDV.
Around 29,000 people had at least one FDV hospital stay from 2010–11 to 2017–18
Of these, 2 in 3 were female (68%) and 1 in 3 were male (32%).
Most (67%) were aged between 15 and 44 at their first FDV hospital stay:
- 1 in 5 were 15–24 (21%)
- 1 in 4 were 25–34 (25%)
- 1 in 5 were 35–44 (21%).
Aboriginal and Torres Strait Islander people were over-represented among those who had a FDV stay; 28% (or 8,232) of those with at least one FDV stay were Indigenous compared with around 3.3% of the Australian population (estimate as at 2016)(ABS 2018).
Around 1 in 8 (3,590 or 12%) people with a FDV hospital stay, had more than one stay, but this varied by population group
People with repeat FDV hospital stays made up a small proportion of those with FDV stays; most people (88%) who had a FDV stay, had only one. However, this varied by sex and Indigenous status:
- Indigenous people were more likely than non-Indigenous people to have more than one FDV hospital stay (20% and 9%, respectively).
- Females were more likely than males to have more than one FDV hospital stay (14% and 9%, respectively).
Other assault hospital stays were higher among the FDV group than among the comparison group
The FDV group experienced 5,500 other assault hospital stays (that is, in addition to their FDV assault hospital stays) in the 8 years to 2018–19. Around 1 in 5 (21%) had multiple assault hospital stays (including both FDV and other assault).
Most (73%) other assault hospital stays for the FDV group had an ‘unspecified’ perpetrator. It is possible that some of these assaults could be due to unidentified FDV.
Head injuries were the most common type of injury leading to a FDV hospital stay
Over half (51%) of FDV hospital stays had a head injury recorded as the first injury within the hospital record (some records have several injuries). This might in part reflect the inherently serious nature of head injuries compared with other types of injuries. The next most common first injury recorded within a hospital stay were injuries to the abdomen (7.5%) thorax (7.5%) and wrist and hand (6.6%). These 4 categories account for 73% of all first injuries of FDV hospital stays. These data refer to the first recorded injury within a hospital stay. However, over half (53%) of FDV hospital stays had multiple injuries recorded.
Repeat FDV hospital stays most commonly occurred within 1 year, but some people experienced several years between stays
Overall, among those who experienced multiple FDV stays, most experienced an additional stay that occurred within 1 year (62%). However, there was also a clear relationship between length of time available in the measurement period, and length of time between additional stays. That is, some people with longer follow-up periods demonstrated several years could occur between identified FDV hospital stays.
Partners were responsible for most FDV hospital stays and most repeat hospital stays
Partners were recorded as the perpetrator for 62% of FDV hospital stays, other family members for 29% and parents for 10% (note these do not add to 100% as a single hospital stay can have multiple perpetrators recorded). Females were more likely to have a hospital stay due to a partner (76% of stays) than males (30% of stays), while males were more likely to have a hospital stay due to ‘other family member’ (55%) than females (18%).
Partners were most likely to be responsible for repeat FDV hospital stays; among the total 3,590 people who had a repeat FDV stay, 2,800 had at least one FDV stay due to a partner. Of these 2,800, 87% had at least one additional stay due to a partner (the remainder had a repeat due to either a parent or other family member).
People who had a FDV hospital stay had a greater number of (acute care) hospital stays, and their principal diagnoses were more varied, than the comparison group
People who had a FDV stay, had 8 hospital stays, on average, compared with 5 hospital stays among the comparison group. The most common principal diagnosis among the FDV group was Injury and poisoning (51% of which were FDV associated). Among the comparison group, the most common principal diagnosis was Persons encountering health services for specific procedures and health care. This includes treatments such as dialysis.
About 1 in 10 hospital stays among the FDV group were for Pregnancy, childbirth and pureperium, highlighting the risks to mothers of this type of violence. Hospitalisation for Mental and behavioural conditions was relatively more common among the FDV group (11% of all hospital stays) than the comparison group (4%), also highlighting the important connections between FDV and poor mental health.
People who had a FDV hospital stay had more ED presentations on average than the comparison group
Almost 9 in 10 (87%) of the FDV group had at least one emergency department (ED) presentation (which did not lead to a hospital admission), compared with 7 in 10 (72%) of the comparison group. The FDV group were also more likely to have multiple ED presentations (87% compared with 73%). People with 3 or more FDV stays were the most likely to have had 10 or more ED presentations (53%). From the national data, it cannot be determined whether any of these presentations were FDV-related.
People who had a FDV hospital stay had a higher rate of death, and different causes of death, when compared with the comparison group
Of the FDV group, 5.7% had a death recorded from 2010 to 2019, compared with 4.4% of the comparison group. The cause of death for these groups also varied. The leading causes of death among the FDV group (where a cause of death was listed) were coronary heart disease, accidental poisoning, suicide and liver disease. The leading causes of death for the comparison group were coronary heart disease, lung cancer and cerebrovascular disease.
When examining the rate ratios, the FDV group were 10 times as likely to die due to assault, 3 times as likely to die due to accidental poisoning or liver disease, and 2 times as likely to die due to suicide, as the comparison group.
This report uses the term ‘hospital stay’ which refers to a continuous period of acute care hospitalisation and may be made up of one or more acute care ‘hospital separations’ (see Figure 2.1 for more information).
Figure S1: Number and demographics of people with at least one FDV hospital stay, 2010–11 to 2018–19
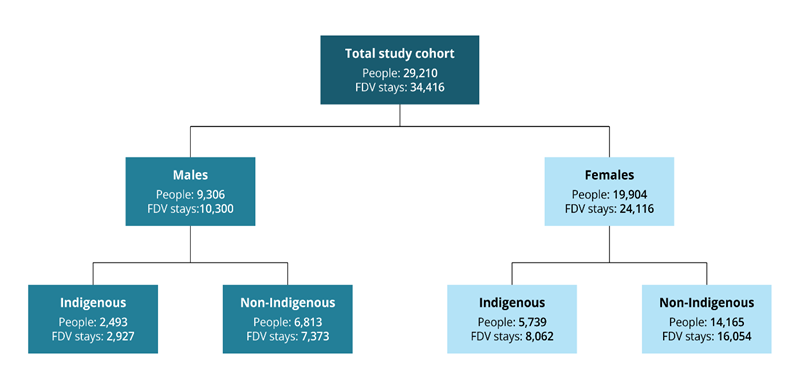
Note: The FDV cohort includes people who had a FDV stay from 2010–11 to 2017–18. Analyses include FDV stays that occurred from 2010–11 to 2018–19. Data for Western Australia and the Northern Territory were not available for analysis.