Technical notes
Scope and features of the COVID-19 register
The AIHW was funded by the Medical Research Future Fund in April 2022 to establish the COVID-19 register (the Register), which is a national linked data asset linking COVID-19 notification data to a range of administrative datasets. This report uses the most recent version of the COVID-19 Register (Version 2.6).
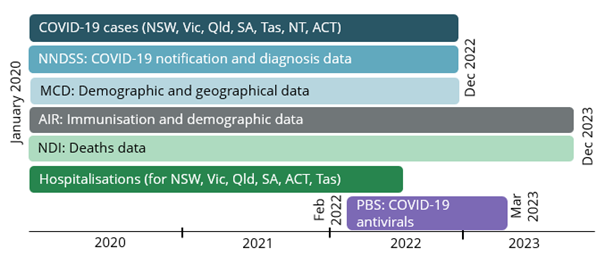
Figure A1 summarises the coverage of each of the data sources used in this report.
COVID-19 case notification data consisted of all notifications from 7 out of 8 states and territories between 25 January 2020 (the date the first case was reported (Hunt 2020)) to 31 December 2022. At the time of setting up the Register, COVID-19 case notifications from all states/territories (except Western Australia (WA)) were available for linkage, owing to WA’s decision to work towards providing these notifications data to the National Health Data Hub (NHDH) instead.
The number of cases of COVID-19 in notifications data will always be an underestimation of the true infection and case rates in the community as some people will not have symptoms, may not seek medical attention or be tested if they are symptomatic. However, underestimation of the rates of COVID-19 probably increased from late 2022 onwards due to a reduction in case detection through changes to testing and reporting requirements, as well as less likelihood of severe disease occurring due to the protective effects of vaccination and prior infection (AIHW 2024).
There are some differences in the geographic and temporal scope of each data source due to the availability of the data in Version 2.6. For example, data from the National Hospital Morbidity Database (NHMD) was only available up to 30 June 2022 and excludes data from Western Australia and the Northern Territory. Time periods for the COVID-19 data also vary slightly by jurisdiction (see Table A1).
Figure A1: Temporal coverage of data sets used (based on the COVID-19 Register Version 2.6)
COVID-19 related hospitalisation definition
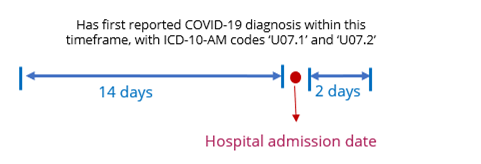
In this report, a standardised definition was used to report COVID-19 related hospitalisations. Hospital admissions that are related in time to a COVID-19 diagnosis will initially be identified and further classified according to ICD-10-AM diagnosis codes recorded in any diagnosis field. Time related hospitalisation is defined as a hospitalisation:
- with a first COVID-19 diagnosis up to 14 days before or 2 days after the hospital admission date, and
- that was not admitted and discharged on the same day to capture admissions related to more severe disease.
A COVID-19 related hospitalisation also had to have COVID-19 recorded in the hospital record (with ICD-10-AM code of U07.1 or U07.2 in any diagnosis field) (Figure A2). A COVID-19 related hospitalisation could be having COVID-19 as a principal diagnosis or an additional diagnosis.
Figure A2: Identification of a COVID-19 related hospitalisation
For the analysis, hospitalisations were created from individual separations. For instance, if a person had multiple separations and the separation and subsequent admission dates were within one day of each another, then they were counted as one hospitalisation. This was to ensure a more accurate alignment of a hospitalisation related in time to a COVID-19 diagnosis. The length of hospital stay was calculated based on the difference between the admission and separation dates.
A first COVID-19 diagnosis had to occur between 15 December 2021 and 1 July 2022 as this end date is the last possible notification date that meets the definition of a COVID-19 related hospitalisation. The small number of hospitalisations related to reinfections were excluded in order to account for the effect of infection-induced immunity on health outcomes. The timeframe used to define a COVID-19 related hospitalisation is based on existing literature and in consultation with National Centre for Immunisation Research and Surveillance (NCIRS) (NSW Government 2023, Stowe et al. 2022).
Using the methodology mentioned above, there were about 30% of COVID-19 related hospitalisations (or close to 35,000) with a COVID-19 code and an acute respiratory code (ICD-10-AM codes J00 to J22) in any diagnosis field (see Table A3).
Diagnosis code for hospitalisation | Number of people with COVID-19 |
|---|---|
Total people with COVID-19 in scope for hospitalisation analysis | 6,200,968 |
No time related hospital admission | 6,075,406 |
Time related hospital admission with a COVID-19 code (COVID-19 related hospitalisation) in any diagnosis field | 114,777 |
Number given an acute respiratory code (J00-J22) in any diagnosis field | 34,940 |
Number without an acute respiratory code (J00-J22) in any diagnosis field | 79,837 |
Time related hospital admission without a COVID-19 code | 10,785 |
Number given an acute respiratory code (J00-J22) in any diagnosis field | 836 |
Number without an acute respiratory code (J00-J22) in any diagnosis field | 9,949 |
Total time related COVID-19 hospitalisations | 125,562 |
Note: This analysis is based on people who had their first reported COVID-19 diagnosis during the Omicron wave. Hospitalisations that occur after subsequent diagnoses for the same person are excluded.
Source: AIHW COVID-19 Register (version 2.6)
Severe and/or fatal hospital outcomes
Severe and/or fatal hospital outcomes were defined as any of the following during the hospital admission:
- having an intensive care unit (ICU) stay
- involving continuous ventilatory support (CVS)
- died in hospital (as recorded by a separation mode of 8 or 80 in the NHMD).
These categories are not mutually exclusive. For example, a person who had an ICU stay and then died in hospital would appear in both categories.
Deaths
The COVID-19 Register contains deaths data from the National Death Index (NDI). Version 2.6 of the COVID-19 Register includes NDI data from 25 January 2020 to 31 December 2022.
It is important to note that the number of COVID-19 deaths reported in the COVID-19 Register may differ from those reported by the Australian Bureau of Statistics and state and territory health departments due to the nature of probabilistic linkage and differing definitions used.
Classifying causes of death
Causes of death are documented on death certificates by medical practitioners or coroners and coded by the Australian Bureau of Statistics (ABS) using the World Health Organization (WHO) International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10).
Underlying cause of death is the disease or injury that initiated the train of events leading directly to death, or the circumstances of the accident or violence that produced the fatal injury. Dying ‘from’ a cause refers to having the condition as the underlying cause.
Most deaths, however, result from more than one contributing disease or condition.
Associated causes of death are all causes involved in the death, other than the underlying cause of death. They include the immediate (or terminal) cause (the condition that occurred immediately before death or closest to the time of death), any intervening causes, and conditions which contributed to the death but were not related to the disease or condition causing the death. Analyses using associated causes of death offer insight into the disease processes occurring at the end of life or, for injury causes of death, the nature of the injury. Dying ‘with’ a cause refers to having the condition as an associated cause of death.
See also Life expectancy & deaths - Glossary and Australia’s health - Glossary.
Deaths due to or with COVID-19
This report aligns ICD-10 code inclusion for dying with, or due to, COVID-19 with other mortality analyses, including the ABS COVID-19 Mortality in Australia: Deaths registered until 31 January 2024.
Deaths due to COVID-19 refers to deaths with COVID-19 as an underlying cause of death, meaning COVID-19 initiated the sequence of events resulting in death. These deaths have an underlying cause of death recorded in the NDI as U07.1 COVID-19 virus identified; U07.2 COVID-19, virus not identified; or U10.9 Multisystem inflammatory syndrome associated with COVID-19.
Deaths with COVID-19 refers to deaths with COVID-19 as an associated cause of death, meaning COVID-19 contributed to the death but was not the underlying cause. These deaths have an associated cause of death recorded in the NDI as U07.1 COVID-19 virus identified; U07.2 COVID-19, virus not identified; or U09.9 Post COVID-19 condition, unspecified.
Deaths due to or with COVID-19 include those that occurred after a reported COVID-19 diagnosis, regardless of time period, or up to 21 days prior to diagnosis.
Case Fatality Rate
The case fatality rate refers to the number of deaths due to COVID-19 divided by the number of people diagnosed with COVID-19 expressed as a percentage.
Timeliness and completeness of deaths data
Cause of death information in the NDI is subject to a revisions process. Cause of death data in this report is final for 2020, revised for 2021, and preliminary revised for 2022. Cause of death information for people who died in 2023 was not available at the time of analysis. These deaths are excluded in the analysis of people who died with or due to COVID-19. For more information on the revisions process, coverage and how deaths data are processed, see ABS Causes of death, Australia, Methodology: Data quality - Revisions process and ABS Causes of Death, Australia methodology.
COVID-19 antiviral prescriptions
Eligibility and access
COVID-19 oral antiviral treatments, Lagevrio® (molnupiravir) and Paxlovid® (nirmatrelvir and ritonavir), were approved by the Australian government for use from January 2022 and made available for selected populations through the Pharmaceutical Benefits Scheme (PBS) from March 2022 (Pharmaceutical Benefits Scheme 2024a, 2024b). COVID-19 antivirals are generally recommended to be taken within 5 days of symptoms starting or testing positive for COVID-19 (Department of Health and Aged Care 2024a).
It should be noted that the eligibility criteria for COVID-19 antivirals have been set up to provide access for people who are vulnerable to severe disease and have broadened over time. Eligible individuals include older Australians and people with specified risk factors, people who are moderately to severely immunocompromised, or people with history of previously being hospitalised for COVID-19 (Pharmaceutical Benefits Scheme 2024c and 2024d).
Table A4 shows the eligibility criteria for COVID-19 antivirals and how they have broadened over time.
Changes to eligibility criteria | Age (years) and/or risk | Moderately to severely immuno-compromised patients | Aboriginal or Torres Strait Islander (First Nations) people |
|---|---|---|---|
65 to 74 with 2 risk factors; or >=75 with one risk factor | No age criteria | >= 50 years with 2 risk factors | |
50 to 69 with 2 risk factors; or >=70 | >=18 | >=30 with 2 risk factors | |
50 to 69 with 2 risk factors; or >=70 | >=18 | >=30 with one risk factor | |
50 to 69 with 2 risk factors (or previously hospitalised for COVID-19); or >=70 | >=18 | >=30 with one risk factor (or previously hospitalised for COVID-19) | |
18 to 49 and previously hospitalised for COVID-19; or 50 to 59 with 2 risk factors (or previously hospitalised for COVID-19); or 60 to 69 with one risk factor (or previously hospitalised for COVID-19); or >=70 | >=18 | >=30 with one risk factor (or previously hospitalised for COVID-19) | |
18 to 49 and previously hospitalised for COVID-19; or 50 to 69 years with one risk factor (or previously hospitalised for COVID-19); or >=70 | >=18 | >=30 with one risk factor (or previously hospitalised for COVID-19) | |
| Criteria from 1 March 2024 | 18 to 49 and previously hospitalised for COVID-19; or 50 to 69 with 2 risk factors (or previously hospitalised for COVID-19); or >=70 | >=18 | >=30 with one risk factor (or previously hospitalised for COVID-19) |
Source: Schedule of Pharmaceutical Benefits
COVID-19 antivirals are generally not recommended for those aged under 18 (Pharmaceutical Benefits Scheme 2024c). However it should be noted that individuals aged under 18 may be prescribed antivirals under exceptional circumstances according to guidelines from some jurisdictions (Children’s Health Queensland 2023, Perth’s Children Hospital 2023, SA Health 2024, The Royal Children’s Hospital Melbourne 2022).
Antiviral data source and coverage
COVID-19 antiviral data in this report were drawn from records of prescriptions dispensed under the PBS in the COVID-19 Register, where either the:
- Australian Government paid a subsidy
- prescription was dispensed at a price less than the relevant patient co-payment (under co-payment prescriptions) and did not attract a subsidy.
PBS data covers all COVID-19 antiviral prescriptions dispensed by approved suppliers, including community pharmacies, public and private hospital pharmacies and dispensing doctors, but does not cover:
- private prescriptions
- medicines supplied to admitted patients in public hospitals (prescriptions to patients on discharge and non-admitted patients in all states and territories are in scope, except for New South Wales and the Australian Capital Territory)
- medicines dispensed through alternative arrangements where the patient cannot be identified, such as direct supply to Aboriginal health services, are excluded.
Provision of some medicines may be under-represented in remote areas, particularly in the Northern Territory, where there are a high proportion of First Nations people who access medicines through Aboriginal health services.
Identifying people who were prescribed COVID-19 antivirals
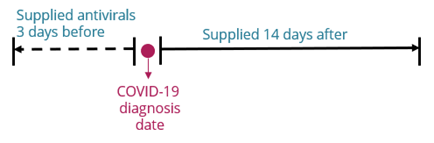
In this report, a person with COVID-19 was considered to have been prescribed COVID-19 antivirals if they were supplied within 3 days before diagnosis of COVID-19 and up to 14 days after diagnosis (Figure A3).
If a person had repeated COVID-19 infections (more than 90 days between two positive tests), prescriptions of antivirals were examined for each infection.
Figure A3: Timeframes for prescribing of COVID-19 antivirals
The following considerations were used for the above definition:
- antivirals supplied a few days before the diagnosis date accounted for any possible delay in COVID-19 notifications or delay in supply of antivirals (as compared to the actual prescribed date)
- antivirals are generally commenced within 5 days of symptoms starting or testing positive for COVID-19 and taken for a course of 5 days (Pharmaceutical Benefits Scheme 2024c and 2024d)
- the median incubation period for SARS-CoV-2 circulating in the time period covered in this report is 5 to 7 days, with a range of 1 to 14 days (Department of Health and Aged Care 2024b)
The analysis on COVID-19 antivirals considers individuals with COVID-19 notification dates from 16 February 2022 to 31 December 2022. This is due to COVID-19 antivirals only being made available through PBS from 2 March 2022 onwards, and because it was possible for an individual to be diagnosed with COVID-19 in mid-late February 2022 to be prescribed antivirals in March 2022 based on the above definition.
COVID-19 vaccination
COVID-19 vaccine recommendations
The COVID-19 vaccination program began as a staged rollout in February 2021 and are free to all people in Australia, including those without a Medicare card. By February 2023, over 95% of Australians aged 16 and over had received at least 2 doses and more than 70% had received 3 doses. About 45% of the eligible population (aged 30 over) had received a fourth dose (Department of Health and Aged Care 2023a).
The rollout was carried out in phases and might have differed across states and territories, as vaccines were allocated based on the proportion of the eligible population in the state or territory and vaccine supply (Australia National Audit Office (ANAO) 2022). Figure A4 below shows key phases of the COVID-19 vaccination rollout which started from February 2021.
Figure A4: Key phases of the COVID-19 vaccination rollout between 2020 and 2022

Note: This figure is a schematic representation of key phases of the COVID-19 vaccination rollout. It does not include all Australian Government advice and recommendations at each key phase.
Source: ANAO 2022, National Centre for Immunisation Research and Surveillance (NCIRS) 2024, Department of Health and Aged Care 2022.