Acute rheumatic fever and rheumatic heart disease are preventable
Acute rheumatic fever (ARF) and rheumatic heart disease (RHD) are both preventable diseases. They are common in low- and middle-income countries, and among population groups living in poor socioeconomic conditions in high-income countries (Naughton et al. 2024; Wyber & Carapetis 2015; Webb et al. 2015). ARF and RHD are caused by aspects of socioeconomic disadvantage, such as houses that are inadequate for the number of residents, socioeconomic deprivation, low levels of functioning ‘health hardware’ (for example, toilets, showers, taps) and lack of access to health care services (Webb et al. 2015; Sims et al. 2016). Improved living conditions and access to functional health hardware can reduce high rates of Strep A infections (Katzenellenbogen et al. 2017).
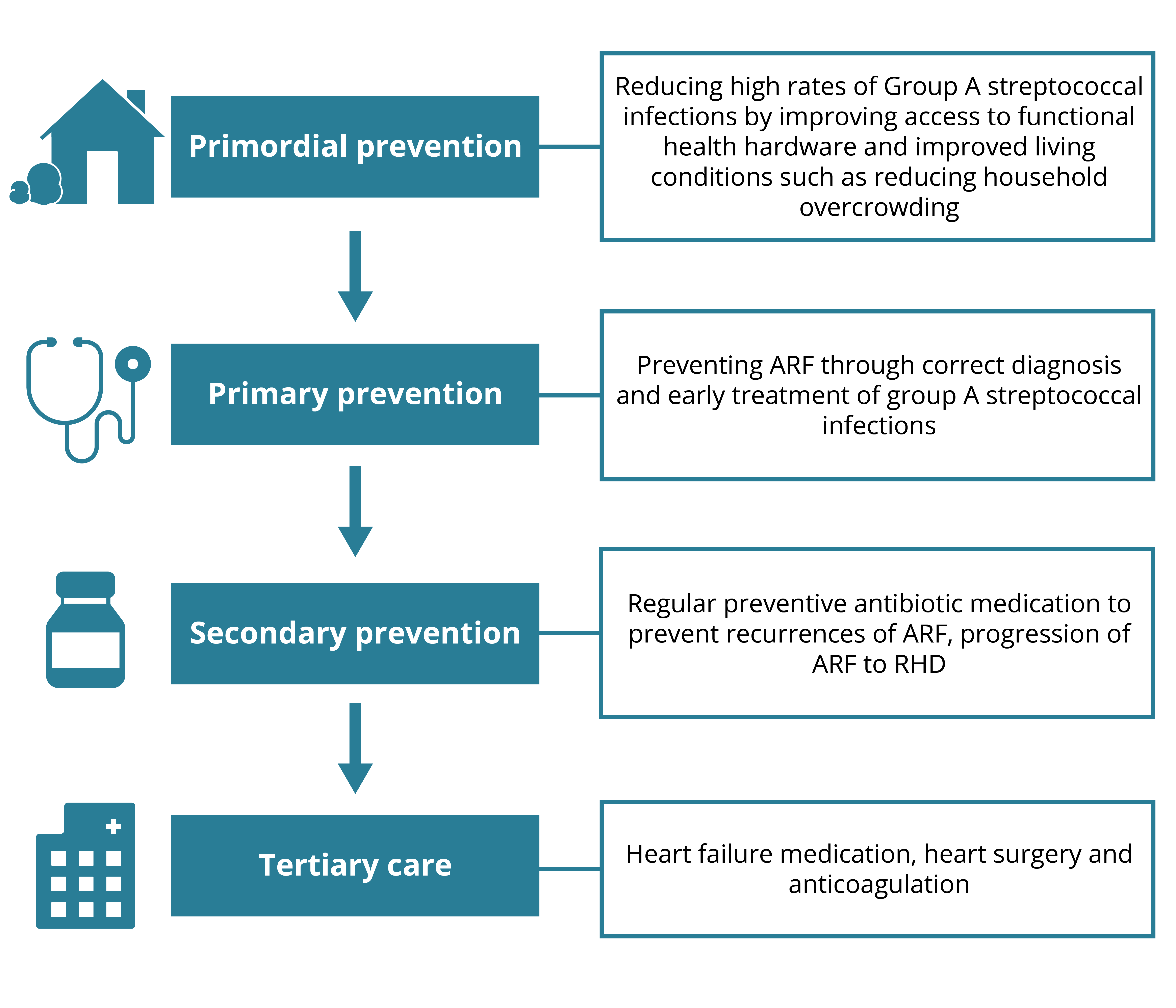
Several opportunities exist to interrupt the disease pathway from Strep A infection to ARF and then RHD (Figure 1.2). The National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people makes recommendations for preventive health assessments that aim to support primary health care providers to prevent, detect and treat ARF and RHD in their communities (NACCHO and RACGP 2024). Prevention measures that improve living conditions and environmental health and address reduction of group A streptococcal infections are called primordial prevention measures.
ARF can also be prevented through the early treatment of Strep A infections with penicillin, as this can interrupt the link between Strep A infection and the abnormal immune response that causes ARF. Given the high prevalence of Strep A skin and throat infections among First Nations people, accurate identification and active treatment of these infections with antibiotics will help reduce the burden of ARF (Menzies School of Health Research 2025).
Secondary prevention of progression from ARF to RHD relies on accurate diagnosis of ARF, to enable commencement of regular antibiotic preventive medication. Correct diagnosis is challenging as there is no specific single laboratory test for ARF, and it can be misdiagnosed. Diagnosis is based on clinical criteria outlined in the Australian modification of the Jones criteria (Technical notes – Table T1), which take into account Australia's high-risk groups.
For people with suspected or clinically confirmed ARF episodes, intramuscular injection of benzathine benzylpenicillin G (BPG) is recommended every 21 to 28 days to prevent further Strep A infections and reduce the risk of developing recurrent ARF. Although the injection causes significant patient discomfort and inconvenience, BPG prophylaxis is the most clinically effective and cost-effective treatment for RHD control at both individual and community levels (Webb et al. 2015; Wyber & Carapetis 2015; Menzies School of Health Research 2025).
Tertiary prevention aims to slow disease progression and prevent complications associated with RHD and can include surgery to repair or replace damaged heart valves once RHD is established (Noonan 2020).
The RHD Endgame Strategy: the blueprint to eliminate rheumatic heart disease in Australia by 2031 (Wyber et al. 2020) estimated that implementing a range of strategies aimed at reducing household crowding, improving hygiene infrastructure, strengthening primary health care, and enhancing the delivery of secondary prophylaxis, would reduce ARF and RHD cases by 69% and 71%, respectively.
Australia’s Long Term National Health Plan to build the world’s best health system, published in August 2019, included 4 key pillars:
- Guaranteeing Medicare and improving access to medicines through the Pharmaceutical Benefits Scheme
- Supporting our public and private hospitals, including improvements to private health insurance
- Mental health and preventive health
- Medical research to save lives and boost our economy.
The Plan presented nine priorities for Pillar One, one of which is to “Eradicate rheumatic heart disease by 2030” (Department of Health 2019). Action at all levels from primordial prevention through to tertiary is critical to achieving this through eliminating new cases of RHD and enabling people already living with ARF and RHD to live long and healthy lives.
Figure 1.2: ARF and RHD prevention measures
Source: AIHW