Health and wellbeing of First Nations people
Web article
Release Date:
Section: First Nations people
Citation
AIHW (Australian Institute of Health and Welfare) (2026) Health and wellbeing of First Nations people, AIHW, Australian Government, accessed 9 July 2026.

Figure 1: Disease group contribution to total, fatal and non-fatal burden among First Nations people, 2022
Mental & substance use disorders was the greatest contributor to total burden (responsible for 20%) and non-fatal burden (40%). Injuries (including suicide) was the greatest contributor to fatal burden at 22%. Musculoskeletal conditions was the second largest contributor to non-fatal burden, and cancer to fatal burden.

Eye health, hearing health, and oral health
In 2023–24, the prevalence of eye/sight problems among First Nations people was 41% based on self-reported data from the ABS NATSIHS (note that this includes corrected refractive error) (ABS 2024).
Vision loss has a profound impact on a person’s quality of life and ability to perform everyday activities, for example, by limiting opportunities for physical mobility, work, education, and social engagement (Razavi et al. 2018). In the 2022-25 Australian Eye and Ear Health Survey, 11.2% of First Nations participants experienced vision impairment (11%) or blindness (0.2%) (AIHW 2026a).
Preventable vision problems, such as trachoma, diabetic retinopathy and cataracts, affect First Nations people aged 40 and over at much higher rates than non-Indigenous Australians of the same age. The Eye health measures for Aboriginal and Torres Strait Islander people annual report provides an evidence base for monitoring changes in eye health among First Nations people, identifying inequalities and highlighting potential gaps in service provision.
Hearing health and oral health problems are 2 issues that also particularly affect First Nations children, especially those living in remote areas.
Among First Nations children aged 0–14, the estimated proportion reporting an ear or hearing problem decreased from 11.2% in 2001 to 4.9% in 2022–23 (AIHW 2025). Middle ear infection was reported as a long-term ear or hearing problem affecting 2.7% of First Nations children aged 0–14 (8,800 children) in 2022–23.
First Nations children are more likely than non-Indigenous children to experience tooth decay and to be hospitalised for dental problems (AIHW 2023a). Several factors contribute to the poorer oral health of First Nations children, including social disadvantage and lack of access to appropriate diet and dental services.
Specific programs such as the Northern Territory Remote Aboriginal Investment Oral Health Program, the Northern Territory hearing health outreach program, and the Queensland Deadly Ears program aim to diagnose and treat these problems and reduce their impact on the First Nations community.
Social and emotional wellbeing
Social and emotional wellbeing is the foundation of physical and mental health for First Nations people. It is a holistic concept that encompasses the importance of connection to land, culture, spirituality and ancestry, and how these affect the wellbeing of the individual and the community (Gee et al. 2014).
Figure 3: Model of social and emotional wellbeing
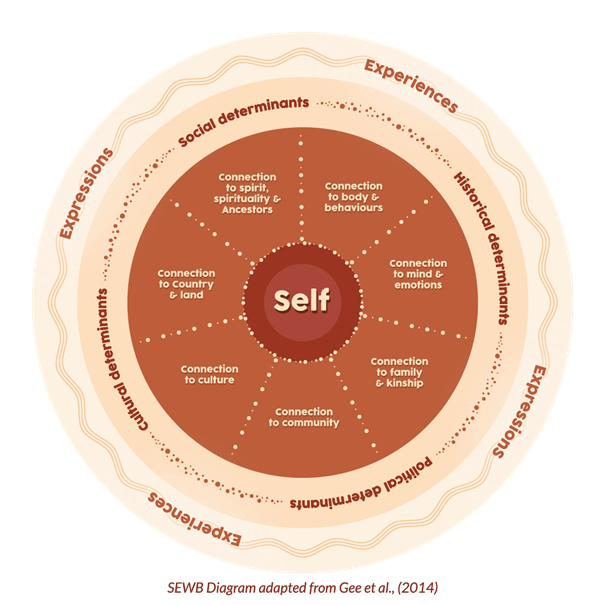
Source: Kimberley Aboriginal Medical Services (2022).
First Nations people’s experience of social and emotional wellbeing varies across different cultural groups as well as across individuals. The concept of social and emotional wellbeing also recognises that a person’s wellbeing is influenced by the social determinants of health, engendered through the inequity of government policies, institutional racism, the effects of colonisation and other past events. For more information, see Determinants of health for First Nations people.
Social and emotional wellbeing is not the same as mental health and mental illness, but they can interact and influence each other (PM&C 2017). The National strategic framework for Aboriginal and Torres Strait Islander peoples’ mental health and social and emotional wellbeing 2017–2023 (the Framework) recognises this distinction and proposes a model of social and emotional wellbeing with 7 overlapping domains (Gee et al. 2014; PM&C 2017).
For many First Nations people, good mental health is indicated by feeling a sense of belonging, having strong cultural identity, maintaining positive interpersonal relationships, and feeling that life has purpose and value (Dudgeon et al. 2014; Dudgeon and Walker 2015). Conversely, poor mental health can be affected by major stressors such as removal from family, incarceration, death of a close friend or family member, discrimination, and unemployment, as well as stressors from everyday life (Gee et al. 2014; PM&C 2017).
In 2022–23, based on self-reported survey responses, an estimated 29% of First Nations people aged 2 and over had a diagnosed mental health or behavioural condition, and 3 in 10 (30%) First Nations adults experienced ‘high or very high’ levels of psychological distress (ABS 2024).
Furthermore, disruptions to family and kinship connections, removal of children from their families (Stolen Generations) and other removals resulting in inter-generational trauma, have been linked to increased suicide and suicidal behaviour in First Nations communities (Dudgeon et al. 2021).
The Stolen Generations
The Stolen Generations survivors and their families are a particular group of Aboriginal and Torres Strait Islander people who experience greater disadvantage than other First Nations people. Analysis of data from the 2014–15 National Aboriginal and Torres Strait Islander Social Survey showed that people who reported being removed from family were more likely than those who did not to have been imprisoned or arrested in the previous 5 years, to have low income, to have poor self-assessed health, to have poor mental health, and to have experienced homelessness in the previous 10 years. This disadvantage persisted through the generations, with adult descendants and co-resident children also experiencing poorer health and wellbeing outcomes compared with other First Nations people (AIHW 2019a, 2019b).
Who are the Stolen Generations?
Between approximately 1910 and 1972, thousands of Aboriginal and Torres Strait Islander children were forcibly removed from their families and communities as a part of government policies across Australian jurisdictions. The Bringing them Home report (HREOC 1997) estimated that this practice affected between 1 in 10 and 1 in 3 First Nations children during that period.
In 2018 –19, there were an estimated 33,600 Stolen Generations survivors across Australia. Around 1 in 3 First Nations adults were estimated to be descendants of the Stolen Generations (AIHW 2021). Updates to these estimates are currently being produced, with an expected release date in late 2026.
Suicide deaths
Reducing deaths by suicide and suicidal behaviour among First Nations people is an issue of major concern for many First Nations communities and a public health priority for all Australian governments. Suicide was the fifth leading cause of death among First Nations people in 2024 (298 deaths), accounting for 5.5% of all deaths (data for New South Wales, Victoria, Queensland, Western Australia, South Australia and the Northern Territory only), and the 17th leading cause of death for non-Indigenous Australians in these 6 jurisdictions (2,882 deaths, of 1.7% of all deaths) (ABS 2025a). Among First Nations children aged 5–17 during the 5-year period 2020–2024, suicide was the leading cause of death for females, and second leading cause for males (ABS 2025d).
Target 14 in the National Agreement on Closing the Gap is a significant and sustained reduction in suicide of Aboriginal and Torres Strait Islander people towards zero.
Between 2018 and 2024, the rate of suicide among First Nations people increased, however this trend should be interpreted with caution as the increases may be due to improvements in Indigenous identification in deaths data over time rather than underlying changes in the suicide rate (Productivity Commission 2026).
When adjusted for population size and age-structure, the suicide rate among First Nations people is more than double that of non-Indigenous Australians (ABS 2025b).
Suicide and self-harm behaviours arise from a complex set of interrelated personal, social, and historical factors (Dudgeon et al. 2017), but they can be prevented. For more information on suicide prevention among First Nations people, see the Indigenous Mental Health and Suicide Prevention Clearinghouse.
Life expectancy and deaths
Life expectancy is widely used as an indicator of population health. In general, life expectancy is higher in females than males, and lower in remote than in non-remote areas. Given current mortality patterns:
- First Nations males born in 2020–2022 could expect to live 71.9 years, and First Nations females 75.6 years
- First Nations males and females living in Major cities expected to live around 5 years longer than those living in Remote and very remote areas (ABS 2023).
Due to significant changes in Indigenous identification over time in both the Census and in death records and the mismatch between how the Indigenous status information is collected in each, it is not possible to compare life expectancy estimates for 2020–2022 with those from earlier time periods (ABS 2023).
The median age at death for First Nations people in New South Wales, Queensland, Western Australia, South Australia and the Northern Territory combined has increased from 57.8 years in 2014 to 63.2 in 2024 (ABS 2025c). In 2024, the leading specific causes of death among First Nations people in these 5 jurisdictions were coronary heart disease, chronic lower respiratory diseases, diabetes, cancers of the lung, bronchus and trachea, and intentional self-harm (ABS 2025a).
Deaths data can also be analysed by broad causes of death. The leading 5 broad causes of death for First Nations people in the 5-year period 2019–2023 were cancer and other neoplasms (24% of deaths), cardiovascular disease (21%), injury and poisoning (14%), respiratory disease (9.4%) and endocrine, nutritional and metabolic diseases (8.8%) (AIHW 2026c).
There have been recent improvements in how Indigenous status is derived in deaths data. While improving the quality of the data overall, these changes have introduced a break in time series in First Nations death statistics in 2022 in NSW, and 2023 in Victoria, with corresponding impacts at the national level (ABS 2025b).
Between 2016 and 2021 (the last year before the break in series), the age-standardised death rate for cancer and other neoplasms increased by 15% for First Nations people in New South Wales, Queensland, Western Australia, South Australia and the Northern Territory combined (AIHW 2026c). There was no significant change in the age-standardised rates for deaths due to cardiovascular disease between 2016 and 2021 for First Nations people.
The Aboriginal and Torres Strait Islander Health Performance Framework provides detailed information on life expectancy and deaths among First Nations people, including infant and child mortality, leading causes of death, avoidable and preventable deaths, and changes over time.
It’s not the same everywhere
On average, First Nations people living in remote areas have higher rates of disease burden and lower life expectancy compared with those in non-remote areas. Key contributors to this include differences in educational and employment opportunities, in access to health services, in housing circumstances, and in other factors that support healthy behaviours (such as the availability and cost of fresh fruit and vegetables). But areas of relative advantage and disadvantage also exist within these regions. Local areas and communities may experience different issues and outcomes to others and have different needs and priorities. Looking at variations across smaller geographic areas can help to highlight specific areas of need, so that programs and services can be directed where they will be of most benefit.
Regional insights for local needs
The Regional Insights for Indigenous Communities (RIFIC) website brings together a range of regional statistics about the health and wellbeing of First Nations people and communities. It aims to help communities set priorities and participate in joint planning with governments and service providers.
Where do I go for more information?
For more information on the health and wellbeing of First Nations people, see:
- Aboriginal and Torres Strait Islander Health Performance Framework
- Australian Burden of Disease Study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018
- Indigenous Mental Health & Suicide Prevention Clearinghouse
- Department of Health, Disability and Ageing Aboriginal and Torres Strait Islander health
For more on this topic, see First Nations people.