Bowel cancer facts
Defining bowel cancer
Bowel cancer (or colorectal cancer) generally develops through a multistage process in which a series of cellular mutations occurs over time. Most bowel cancers start in the epithelial cells, which form part of the inner lining of the large bowel (intestinal mucosa layer). Early stages of these mutations result in benign polyps. However, a polyp may mutate further and become a benign adenoma and, ultimately, a malignant bowel cancer (Figure 1.1). Later stages of bowel cancer can spread to other sites in the body through the lymphatic or vascular system.
Figure 1.1: Beginnings of bowel cancer
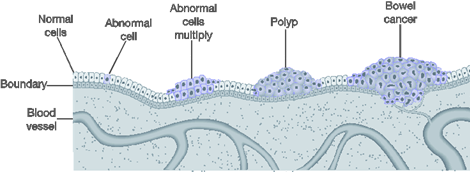
© Commonwealth of Australia 2024.
Cancer stage
Bowel cancer stage describes the extent or spread of cancer in the body at diagnosis. Staging is usually based on the size of the tumour, whether lymph nodes contain cancer, and whether the cancer has spread from the original site to other parts of the body (Brierley et al. 2016). Cancer Australia, in consultation with state and territory cancer registries and the Australian Institute of Health and Welfare (AIHW), developed cancer staging rules for high‑incidence cancers (including bowel cancer). These registry-defined cancer stages are closely related to the Tumour, Nodes and Metastasis (TNM) Classification of Malignant Tumours. Prognosis is often related to what stage of development the cancer has reached when first diagnosed, with smaller, less developed cancers having better prognoses than advanced cancers (Table 1.1).
| Registry-derived Australia stage | Description | 5-year relative survival estimates |
|---|---|---|
I | Stage I – equivalent to TNM stage I: early stage Cancer has invaded several layers of the bowel, but has not spread outside the bowel wall | 99% |
II | Stage II – equivalent to TNM stage II: early stage Cancer has grown through the muscle layer of the bowel or rectum and invaded nearby tissues, but has not spread to the lymph nodes | 89% |
III | Stage III – equivalent to TNM stage III: locally advanced Cancer has spread to nearby lymph nodes, but not to other parts of the body | 71% |
IV | Stage IV – equivalent to TNM stage IV: metastatic The cancer has spread from where it started in the colon or rectum to other organs, often the liver and lungs, and/or non-regional lymph nodes | 13% |
Note:
Descriptions and 5-year relative survival estimates were sourced from 2011 Australian stage data (AIHW 2019).
Risk factors for bowel cancer
A risk factor is any factor associated with an increased likelihood of a person developing a health disorder or health condition. It is not known what causes bowel cancer; however, several risk factors have been identified that may increase the chance of developing it – see Box 1.1 (AIHW 2021; Bouvard et al. 2015; Dekker et al. 2019; IARC 2014; Song et al. 2015; WCRF and AICR 2007).
Box 1.1: Risk factors for bowel cancer
Behavioural and biomedical factors
Personal and lifestyle factors associated with an increased risk of bowel cancer include:
- dietary risks (diet high in red meat, processed meat, and diet low in whole grains, high-fibre cereals and milk)
- overweight and obesity
- physical inactivity
- alcohol use
- tobacco use
- high blood plasma glucose
- occupational hazards and exposures.
Family history and genetic susceptibility
Some genetic mutations increase the risk of bowel cancers, and these can also be passed from parent to child. Between 12% and 35% of bowel cancers can be attributed to a hereditary component (Dekker et al. 2019).
Ionising radiation
Ionising radiation from radiology (diagnostic X-rays), working in the nuclear industry, and natural sources can be a risk factor for bowel cancer.
Bowel cancer treatment
The aim of bowel cancer treatment is generally to remove the cancer and any cancer cells that may be left in the bowel or other parts of the body. However, treatment can vary based on individual factors, such as the type of cells involved, the size of the tumour, and the bowel cancer stage – some patients may receive palliative care. Treatment of bowel cancer commonly involves surgery to remove the cancer, with or without chemotherapy or radiation therapy.
Early diagnosis of bowel cancer can improve treatment outcomes and survival. Further, removal of polyps and adenomas (polypectomy) during a colonoscopy reduces the risk of their developing into bowel cancer. The excision of adenomatous polyps, together with regular surveillance, has been found to reduce bowel cancer incidence and mortality (Dekker et al. 2019).