Methods
Data are presented on the number of babies with in scope congenital anomalies in the 2017 birth cohort, that were diagnosed up to 12-months of age and the women who gave birth to these babies. The number of babies is higher than the number of women who gave birth due to the occurrence of multiple births.
In scope congenital anomalies are those that have significant medical, social or cosmetic outcomes for an individual. Over 400 congenital anomaly condition codes at the 4-character level of the ICD-10-AM are in scope for this report. These were agreed to by NCAAG, as were out-of-scope anomalies (see ![]() Reporting inclusions and
Reporting inclusions and ![]() Reporting exclusions).
Reporting exclusions).
Out of scope anomalies include:
- terminations of pregnancy before 20 weeks’ gestation
- anomalies diagnosed after 12 months of age
- anomalies that do not have significant medical, social or cosmetic outcomes – these are sometimes referred to in other literature as minor congenital anomalies (CDC 2020)
- anomalies where data were not available across all reporting jurisdictions.
Some in scope congenital anomalies, 1,226 (4%) were excluded from reporting for data quality reasons. This included where the state of birth was unknown, to ensure duplicate records were not included across jurisdictions, or where records could not be linked to the NPDC.
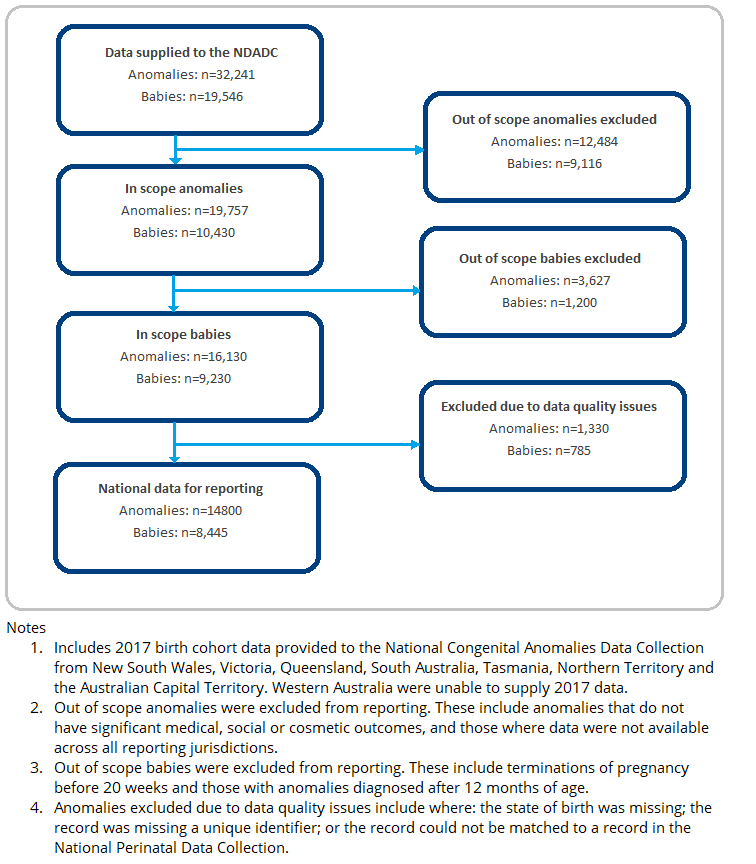
Figure 6 describes the process for deriving the numbers presented in this report, the cases excluded from national reporting and why these were excluded.
Figure 6. Processing flowchart for 2017 NCADC data
Numbers and rates
The NCADC reports estimates per 1,000 total births (live births and stillbirths). This provides information about the rate of the anomaly among all births. Estimates are based on the number of cases (live births and stillbirths) from the NCADC, divided by the total number of births (live births and stillbirths) from the respective NPDC birth cohort. The NPDC includes live births and stillbirths of at least 20 weeks of gestation or at least 400 grams birthweight. Terminations of pregnancy of at least 20 weeks of gestation or at least 400 grams birthweight are included as births. No congenital anomalies data were available for Western Australia in 2017, so this jurisdiction was not included in the numerator or denominator for rate calculations.
It is not possible to identify all cases with a particular anomaly, as a proportion of pregnancies affected with an anomaly will spontaneously miscarry before being diagnosed. This report also excludes terminations of pregnancy before 20 weeks’ gestation and cases diagnosed after 12 months of age, so the numbers and rates presented will underestimate the overall prevalence of congenital anomalies in Australia. Moreover, there are differences in the methods used to collect congenital anomalies data between jurisdictions, so the numbers and rates presented should be interpreted with caution. More information about the impacts of these differences can be found in Data quality, availability and interpretation.
Small numbers
Data on specific anomalies are presented at the national level, and any disaggregation by baby and maternal characteristics at the broad body system level, to protect the privacy of individuals. In the baby characteristics and maternal characteristics sections, ‘not stated’ values were excluded from calculations due to small numbers. These represented a small number (less than 1%) of cases.
Calculation of perinatal mortality rate
The perinatal mortality rate is calculated as the proportion of births in a specified population which are stillbirths or neonatal deaths (perinatal deaths). This proportion is expressed in relation to all births.
The perinatal mortality rate for babies diagnosed with one or more congenital anomalies is calculated as the proportion of births in this population which are stillbirths or neonatal deaths (perinatal deaths). This proportion is expressed in relation to all births in babies with one or more congenital anomalies.
To calculate the perinatal mortality rate:
Perinatal mortality rate = Number of perinatal deaths x 1,000 / Total number of births
Classification system
Anomalies in this report were coded according to the tenth edition of the ICD-10-AM. The classification system used to code congenital anomalies can vary by jurisdiction. In New South Wales, the ICD-9-BPA is used to code anomalies recorded in the New South Wales Register of Congenital Conditions. In Victoria, Queensland, South Australia, Tasmania, the Northern Territory, the Australian Capital Territory, and for the New South Wales admitted patient data collection, anomalies are coded using the ICD-10-AM.
All national congenital anomalies data were standardised to ICD-10-AM. The ICD is hierarchical, with various disease chapters, including one on congenital anomalies that are divided into more specific disease groupings (represented by 3-character codes). These groupings can mostly be divided into more specific disease categories, represented by 4- and 5-character codes. Most NCADC data (98.3%) were supplied and analysed at the 4- and 5-character code level of detail.
Anomaly descriptions
There are no nationally agreed clinical definitions for the anomalies included in this report, so the AIHW worked with the NCAAG to develop simple descriptions for this report. Brief descriptions for a data visualisation and for the glossary were developed. These are based on a range of sources, including for example, the Centers for Disease Control and the WHO birth defect surveillance atlas.
Data elements
Various characteristics of the babies diagnosed with an anomaly and the women giving birth to these babies are presented. Baby characteristics include sex, birthweight, birthweight adjusted for gestational age, gestational age and jurisdiction of birth. Information is also presented on outcomes and whether the baby was liveborn and survived the neonatal and post-neonatal period.
For women giving birth to a baby with an anomaly, information is presented on their First Nations status, age at the birth of their baby, parity, plurality and remoteness area of usual residence. The data elements included in this report are described below.
Baby characteristics
Sex
Data on the sex of each baby were collected as ‘male’, ‘female’, ‘indeterminate’ or ‘not stated’. Data for indeterminate or not stated sex were excluded from reporting in the Baby characteristics section due to small numbers.
Birthweight
Birthweight is the first weight of the liveborn, or stillborn baby obtained after birth. In this report babies are defined as being of ‘low’ birthweight if their weight at birth is less than 2,500 grams. Babies are defined as being a ‘normal’ birthweight if their weight at birth is 2,500g or more and this includes a small number of babies (around 1%) with a high birthweight (4,500g or more). A small number of records with 'not stated' birthweight were excluded from reporting in the Baby characteristics section due to small numbers.
Gestational age
Gestational age is the duration of pregnancy in completed weeks, calculated from the date of the first day of a woman’s last menstrual period and her baby’s date of birth; or via ultrasound; or derived from clinical assessment during pregnancy or from examination of the baby after birth. The WHO defines ‘pre-term’ as less than 37 completed weeks of gestation, ‘term’ as 37 completed weeks to less than 42 completed weeks of gestation, and ‘post-term’ as 42 or more completed weeks of gestation. Pre-term birth is associated with morbidity and mortality in newborn babies. In this report babies are defined as being at ‘term’ if they have 37 completed weeks of gestation. This includes a small number of babies (less than 1%) that were born ‘post-term’ (at 42 or more completed weeks of gestation). A small number of records with 'not stated' gestational age were excluded from reporting in the Baby characteristics section due to small numbers.
Birthweight adjusted for gestational age
A baby may be small due to being pre-term (born early) or being small for gestational age (either due to genetic factors, or because it is the subject of a growth restriction within the uterus). Adjusting birthweight for gestational age allows for differences in a baby’s growth status and maturity to be taken into account when examining their health outcomes at birth. Data on birthweight adjusted for gestational age are limited to liveborn singleton babies. Babies are defined as being ‘small for gestational age’ if their birthweight is below the 10th percentile for their gestational age and sex, as determined by national percentiles. Babies are defined as being ‘large for gestational age’ if their birthweight is above the 90th percentile for their gestational age and sex.
Jurisdiction
This is the state or territory where a baby is born. It is not necessarily the state or territory where the woman giving birth usually lives.
Maternal characteristics
Age
The age of a woman at the birth of their baby. A small number of records with 'not stated' age were excluded from reporting in the Maternal characteristics section due to small numbers.
First Nations status
First Nations status refers to whether a woman giving birth has identified as being of Aboriginal, Torres Strait Islander, or both Aboriginal and Torres Strait Islander origin. Non-Indigenous women refers to women giving birth who have not identified as Aboriginal or Torres Strait Islander. A small number of records with 'not stated' First Nations status were excluded from reporting in the Maternal characteristics section due to small numbers.
Parity
Parity refers to the number of previous pregnancies that resulted in live births or fetal deaths. In this report, categories include ‘primiparous’ for the first pregnancy, or ‘multiparous’, for one or more previous pregnancies. A small number of records with 'not stated' parity were excluded from reporting in the Maternal characteristics section due to small numbers.
Plurality
Plurality refers to the number of babies resulting from a single pregnancy. In this report, categories include ‘singleton’ for a single birth, and ‘multiple’ for the births of twins, triplets, quadruplets, quintuplets, sextuplets and other. A small number of records with 'not stated' plurality were excluded from reporting in the Maternal characteristics section due to small numbers.
Remoteness area
This is the remoteness area of usual residence. This report uses the Australian Statistical Geography Standard (ASGS) that groups geographic areas into 6 classes of Remoteness Area based on their relative access to services using the Accessibility/Remoteness Index of Australia. The 6 classes are: Major cities, Inner regional, Outer regional, Remote, Very remote and Migratory (ABS 2018). Remoteness area is derived by applying the ABS 2011 Australian Statistical Geography Standard to the area of mother’s usual residence. It only calculated where geographic area of usual residence was provided. Due to small numbers, remoteness area is presented under 4 categories: Major cities, Inner regional areas, Outer regional areas and Remote and very remote areas.
References
ABS (Australian Bureau of Statistics) (2018) Australian Statistical Geography Standard (ASGS): Volume 5 – Remoteness Structure, July 2016 , ABS website, accessed 5 July 2023.