Allergic rhinitis
In 2017–18, an estimated 19% of Australians had allergic rhinitis. Children were less likely to have allergic rhinitis (10%) compared with all other age groups (Figure 1).
Figure 1: Prevalence of allergic rhinitis, by sex and age group, 2017–18
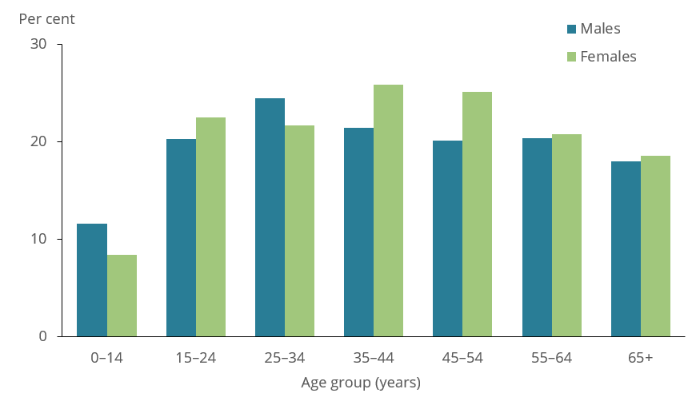
Note: Allergic rhinitis refers to self-reported current and long-term allergic rhinitis.
Source: ABS 2018 (Data tables).
The ACT had the highest rate of allergic rhinitis in Australia (29%) in 2017–18 compared with all other states and territories (Figure 2).
Figure 2: Prevalence of allergic rhinitis, by state and territory, Australia, 2017–18

Note: Rates have been age-standardised to the 2001 Australian Standard Population as at 30 June 2001. Age groups: 0–14, 15–24, 25–34, 35–44, 45–54, 55–64, 65+.
Source: ABS 2018 (Data tables).
Treatment of allergic rhinitis
There are a range of treatments available for allergic rhinitis, many of which do not require a prescription from a doctor. The main medicines used are intranasal corticosteroids (nasal sprays) and oral antihistamines. For persistent allergic rhinitis and for moderate/severe intermittent allergic rhinitis, guidelines recommend the use of nasal sprays as the first-line therapy (AIHW 2019). For mild intermittent allergic rhinitis, the use of antihistamines is recommended (AIHW 2019).
Comprehensive data are not available on the use of allergic rhinitis medicines. Data from pharmacy suppliers, however, suggest that spending by pharmacies on these medicines doubled between 2001 and 2010, going from $107.8 million to $226.8 million per year (AIHW 2011). While not all of these medicines would have been used for allergic rhinitis, treatment of this condition is likely to have accounted for a large proportion of the increase.
Seasonality of pharmacy supply pattern
Each year between 2006 and 2010, the wholesale supplies of oral antihistamines increased around July and peaked around October–November (AIHW 2011).