Did access to antenatal care change during the COVID-19 pandemic?
Given the importance of antenatal care for the health and wellbeing of both the mother and child, and its role in the identification of high risk pregnancies, there is a possibility that changes in use of antenatal care could have adverse effects on outcomes for mothers and babies.
This report seeks to explore the potential impact of the COVID-19 pandemic in Australia on use of antenatal care, using the most recently available MBS data. The report provides preliminary analysis of changing service usage from January 2020 through to December 2020 with comparisons to 2018 and 2019. It focusses specifically on antenatal services claimed on the MBS, defined as:
- Professional antenatal attendance by a medical practitioner;
- Planning and management of a pregnancy, by a medical practitioner, where the pregnancy has progressed beyond 28 weeks' gestation and the service includes a mental health assessment (payable once per pregnancy); or
- Antenatal service provided by a nurse, midwife or an Aboriginal and Torres Strait Islander health practitioner on behalf of, and under the supervision of, a medical practitioner; or
- Professional antenatal attendance performed by a participating midwife.
These services will be referred to collectively as antenatal care throughout the report. This report also looks at diagnostic imaging (ultrasound) services that relate to the management of pregnancy.
The impact of any changes in antenatal care service use on outcomes for mothers and babies is not available from MBS data. This will be explored in the future through analysis of data from the National Perinatal Data Collection in the Australia’s Mothers and Babies publication.
Limitations
This report includes data on antenatal care services eligible for Medicare Benefits rebates only. As such, this report does not include antenatal services provided within public hospitals to public patients or services that qualify for benefits under the Department of Veterans’ Affairs National Treatment account. We acknowledge that antenatal care provided through public hospital services, not covered in this report, contributes significantly to antenatal care provided in Australia. This means data in this report is considered preliminary. However, these limitations also apply to 2018 and 2019 data and therefore these years are provided as baselines to identify changes in use of antenatal care services eligible for Medicare Benefits rebates. Please see Technical notes for a list of MBS items included in this analysis.
This data presents the number of claims for antenatal care processed by Services Australia. Data does not reflect the number of individuals who received the service, nor number of sessions of care an individual received.
Month/quarter relates to the date the claim was processed by Services Australia, not the date care was provided. Further analysis, when other data is available, will be required to ensure that differences are true changes in service usage. More definitions and details on limitations are included in the Technical notes.
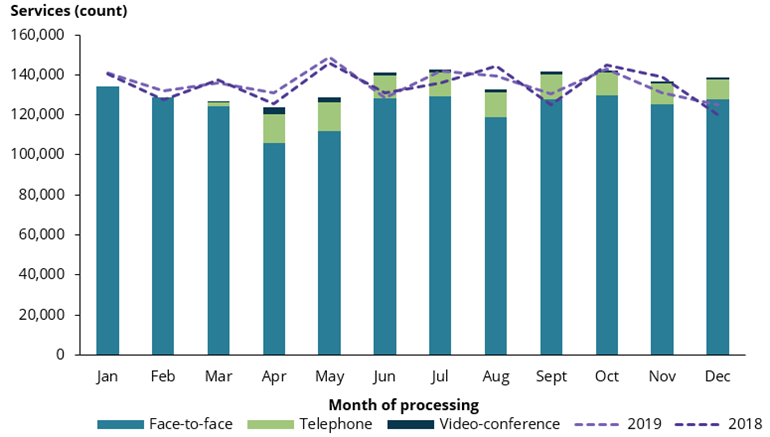
During 2020 over 1.6 million services for antenatal care were processed nationally. Trends in the number of antenatal services processed were similar in 2018 and 2019 (Figure 2). As such, commentary in this report has focussed on comparisons between 2020 and 2019:
- There were around 136,000 fewer face-to-face antenatal services compared with 2019.
- The decrease in face-to-face services was mostly offset by telehealth services (added in March 2020), that contributed 126,000 antenatal services from March to December 2020.
- Overall, there were reductions in services processed during some months in 2020. However this had mostly recovered by December, leaving a decrease of less than 10,000 services (a 0.6% reduction) during 2020 compared with 2019.
In March 2020, the total number of antenatal care services processed dropped by around 9,100 (6.7%) compared to March 2019, in line with the introduction of COVID-19 restrictions around the country. April 2020 displayed a similar trend, where services processed were 5.4% less than the previous year. The largest drop was observed in May. Around 20,000 fewer services were processed in May 2020 compared to May 2019, a decrease of nearly 14% (Figure 2). In June 2020 the number of services processed was higher than in June 2019, and in July number of services processed was very similar for 2020 and 2019.
While the number of services processed recovered in June and July, they dropped again in August, likely reflecting another spike in cases in Australia at that time (DoH 2020). However, from September onwards the number of antenatal services processed mostly continued to improve; with September, November and December all showing an increase in services processed compared to the same months in 2019.
Figure 2: Antenatal care services, by method of delivery and month of processing, Australia, 2020
Notes:
- Month is determined by the date the service was processed by Services Australia, not the date the service was rendered. Monthly figures may vary due to the varying number of processing days in a month, which depends on the number of days in the month, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
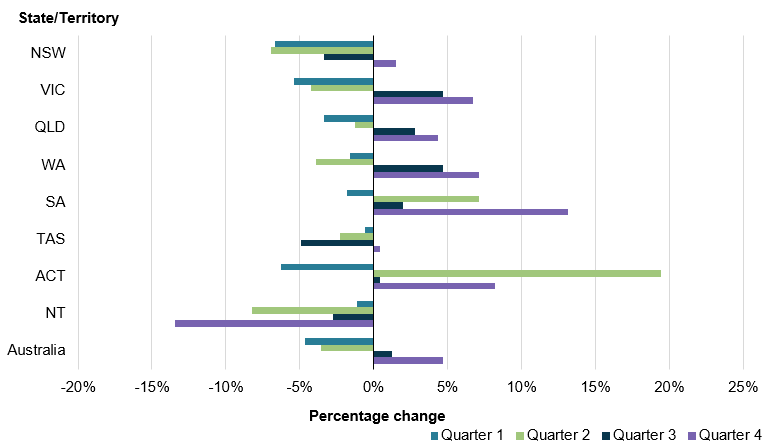
Over 2020, New South Wales (NSW) experienced the largest reduction in antenatal care services processed, a drop of more than 21,000 services. This is a 3.9% decrease compared with the same period in 2019. Figure 3 shows that during the second quarter of 2020, the Northern Territory (NT), NSW and Victoria had the largest proportional drop in antenatal services processed compared with second quarter of 2019 (8.2%, 6.9% and 4.3% respectively). Conversely, for the Australian Capital Territory (ACT) there was a large increase (19.5%) in antenatal services processed during quarter 2 compared to 2019. South Australia also experienced an increase in quarter 2 compared to 2019.
Figure 3: Quarterly percentage change in antenatal services processed during 2020 from 2019, by state/territory
Notes
- Quarter is determined by the date the service was processed by Services Australia, not the date the service was rendered. Quarterly figures may vary due to the varying number of processing days in a month/quarter, which depends on the number of days in the month/quarter, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
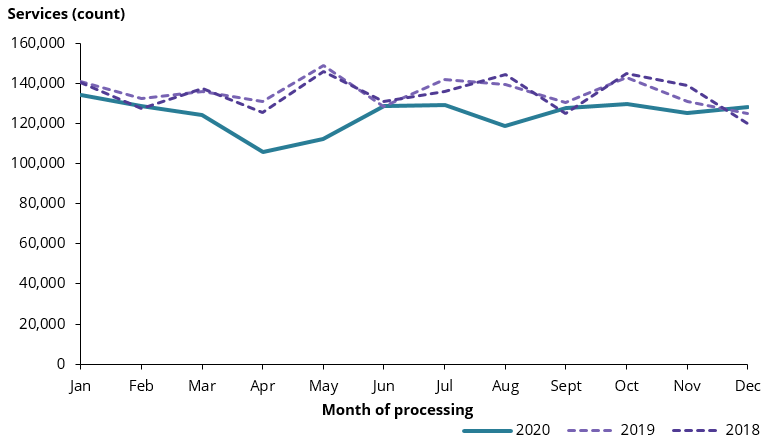
Nationally, there were around 136,000 fewer face-to-face antenatal care service claims processed during 2020, compared 2019. This is an 8.3% decrease for 2020 compared to the previous year.
Generally, the national trend for face-to-face services was similar to the trends described for total antenatal services, as face-to-face services made up the majority (around 92%) of antenatal services processed during 2020. The number of face-to-face antenatal care services processed decreased most noticeably from March to April (Figure 4). In April 2020 nearly 106,000 services for face-to-face antenatal care were processed, 19.2% fewer than April 2019. In May 2020, 112,000 antenatal care services were processed, 24.7% fewer than May 2019.
Figure 4: Face-to-face antenatal services, by month of processing, Australia 2018–2020
Notes
- Month is determined by the date the service was processed by Services Australia, not the date the service was rendered. Monthly figures may vary due to the varying number of processing days in a month, which depends on the number of days in the month, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
What happened in the states and territories?
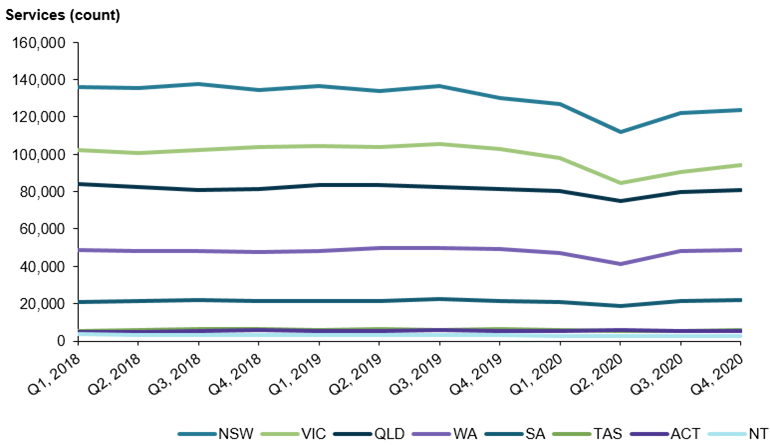
Most states and territories experienced a decrease in face-to-face services in quarter 2 of 2020 (Figure 5). Victoria and NSW had the highest incidence of COVID-19 in Australia during 2020 (DoH 2020) and correspondingly recorded the largest reductions in services for face-to-face antenatal care (Figure 5). Victoria had the largest decrease (11.8%) in face-to-face antenatal care services processed during 2020 when compared with 2019. NSW also had a 9.8% drop in face-to-face services in 2020 compared to the previous year. For the ACT antenatal care services processed remained similar to previous years, with a 0.3% difference when compared with the same period in 2019.
Figure 5: Face-to-face antenatal services, by state/territory and quarter of processing, 2018–2020
Notes
- Quarterly figures may vary due to the varying number of processing days in a quarter, which depends on the number of days in the month/quarter, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
In response to the COVID-19 pandemic, the Australian Government added temporary telehealth items to the MBS in March 2020 (DoH 2020b). These items cover antenatal attendances and services provided by video-conference or telephone. Telehealth services can improve accessibility in certain situations. There are some limitations to telehealth. Health providers need to ensure that the provision of services occurs safely, in accordance with relevant professional standards, and are satisfied that it is clinically appropriate to provide the telehealth service to the patient (DoH 2020b; RANZCOG 2020; RANZCOG 2020b). In the United Kingdom, virtual appointments are suggested only when no antenatal physical examination is required, or there are no additional risk factors (RCOG 2020).
From March until December 2020, almost 1 in 10 (9.3%) antenatal care services processed were delivered via telehealth (either by telephone or video-conference).
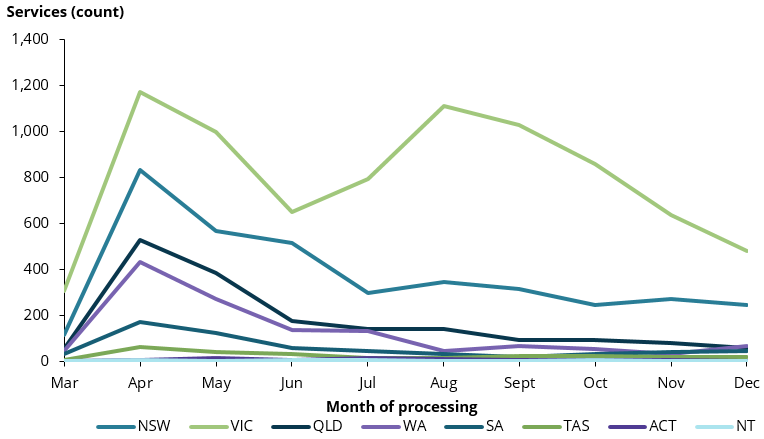
The peak uptake for telehealth antenatal care services was in April and May 2020 (17,987 and 16,525 respectively). During these months, telehealth services made up 14.5% and 12.9% respectively of total antenatal care services processed. For most states and territories, these numbers declined after May (Figures 6 and 7).
However, in Victoria the use of telehealth services rose again after June, reaching the highest peak in August. This coincides with a second wave of COVID-19 and increased restrictions in Victoria during this time. For the month of August, 1 in 5 antenatal care services processed for Victoria were telehealth services (7,173 services).
Figure 6: Video-conference antenatal services by state/territory and month of processing, 2020
Notes
- Month is determined by the date the service was processed by Services Australia, not the date the service was rendered. Monthly figures may vary due to the varying number of processing days in a month, which depends on the number of days in the month, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
- Temporary telehealth items were added to the MBS on 13 March 2020, therefore no data is available prior to March.
- The scale is different for Figures 6 and 7, therefore they are not directly comparable to each other.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
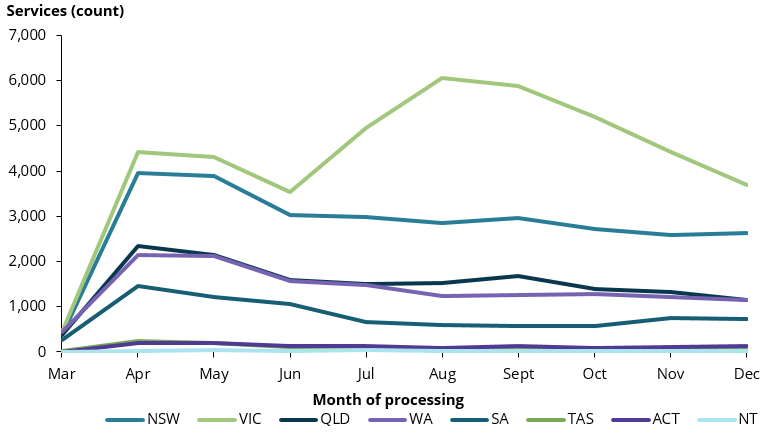
Figure 7: Telephone antenatal services by state/territory and month of processing, 2020
Notes
- Month is determined by the date the service was processed by Services Australia, not the date the service was rendered. Monthly figures may vary due to the varying number of processing days in a month, which depends on the number of days in the month, public holidays, overtime worked, and events such as school holidays that may impact staffing. Additionally, processing may have been impacted by COVID-19.
- Refer to Technical Notes for list of MBS items included in this analysis.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
- Temporary telehealth items were added to the MBS on 13 March 2020, therefore no data is available prior to March.
- The scale is different for Figures 6 and 7, therefore they are not directly comparable to each other.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
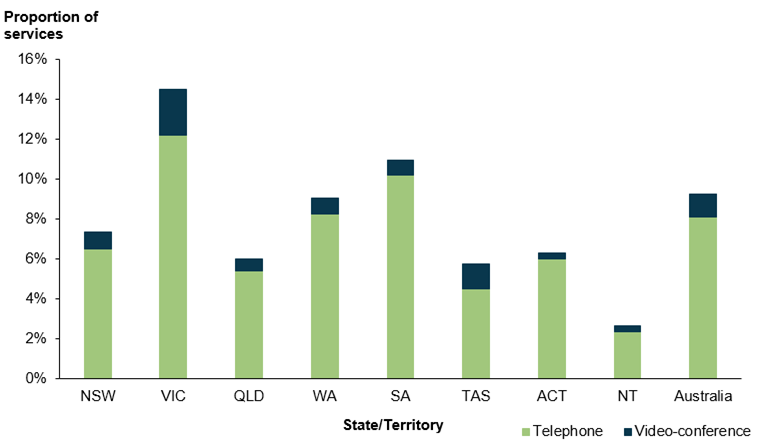
During the period March to December 2020, telehealth services were most common in Victoria, comprising nearly 15% of antenatal care services processed during this period. South Australia had the second highest proportion, with 11.0% of antenatal services claimed as telehealth (Figure 8).
Use of antenatal telehealth services was least common in the Northern Territory, where less than 3% of antenatal services processed for March to December were telehealth services.
Across the country, telephone consults were more common than video-conference, comprising 87.5% of antenatal telehealth services.
Figure 8: Proportion of antenatal services processed as telehealth, by state/territory, March to December 2020
Notes
- Refer to Technical Notes for list of MBS items included in this analysis.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
- Temporary telehealth items were added to the MBS on 13 March 2020, therefore no data is available prior to March.
Chart: Australian Institute of Health and Welfare
Source: AIHW analysis of Medicare Benefits Schedule item reports. Sourced on 15 April 2021.
DoH (Australian Government Department of Health). 2020. Coronavirus (COVID-19) current situation and case numbers. Canberra: DoH. Viewed 22 December 2020.
DoH (Australian Government Department of Health). 2020b. COVID-19 Temporary MBS Telehealth Services. Canberra: DoH. Viewed 23 November 2020.
RANZCOG (The Royal Australian and New Zealand College of Obstetricians and Gynaecologists). 2020. Advice to obstetricians and gynaecologists, GP obstetricians. 14 March 2020. Melbourne: RANZCOG. Viewed 15 January 2021.
RANZCOG (The Royal Australian and New Zealand College of Obstetricians and Gynaecologists). 2020b. Updated advice for the care of pregnant women. 5 June 2020. Melbourne: RANZCOG. Viewed 15 January 2021.
RCOG (Royal College of Obstetricians and Gynaecologists). 2020. Coronavirus (COVID-19) infection in pregnancy. Information for healthcare professionals. United Kingdom. Version 12: Published 14 October 2020.