Technical notes
Department of Defence
Information on ex-serving ADF members was obtained from the Personnel Management Key Solution (PMKeyS). PMKeyS is a Department of Defence staff and payroll management system that contains information on all people with ADF service on or after 1 January 2001 (when the system was introduced).
Multi-Agency Data Integration Project (MADIP)
MADIP is a partnership among Australian Government agencies to develop a secure and enduring approach for combining information on healthcare, education, government payments, personal income tax, and demographics (including the Census) to create a comprehensive picture of Australia over time (ABS 2022). More information about the MADIP can be found at Multi-Agency Data Integration Project (MADIP) | Australian Bureau of Statistics (abs.gov.au).
The key MADIP datasets used in the analysis for this report (with potential to utilise more in the future) are:
- MADIP Person Linkage Spine (Australian Bureau of Statistics)
- 2011 Census of Population and Housing (Australian Bureau of Statistics)
- Causes of Death / Deaths Registrations (Australian Bureau of Statistics)
National Death Index (NDI)
The NDI is managed by the AIHW and contains person-level records of all deaths in Australia since 1980 obtained from the Registrars of Births, Deaths and Marriage in each state and territory. Its use is confined to data linkage studies approved by the AIHW Ethics Committee for health and medical research. NDI records are supplemented with cause of death information from the NMD (AIHW, 2018b).
In this study, the NDI is linked with Defence payroll data to create the linked PMKeyS–NDI data set used in analysis of suicide in the ADF population.
Defence Suicide Database (DSD)
The DSD is maintained by Defence and contains information on suspected and confirmed deaths due to suicide of personnel serving full time since 1 January 2000. Suspected and confirmed suicides are included in the database only on the advice of the ADF Investigative Service. Cases are confirmed by receipt of a coronial finding of suicide. This database is linked to the PMKeyS and NDI and records with a status of ‘confirmed’ are used to supplement cause of death information from the NDI for numbers of suicides only.
ABS Causes of Death / Deaths Registrations
Causes of death are coded by the ABS to the International Statistical Classification of Diseases and Related Health Problems (ICD). Cause of death for a small number of records may change where a death is being investigated by a Coroner and more up to date information becomes available as a result of the ABS revisions process. This may have a small effect on the number of deaths attributed to suicide in these years. Further information can be found in the Causes of Death, Australia methodology (ABS 2021).
Although this method likely captures the vast majority of suicides, there is potential for some to be missed if coronial findings are finalised or updated more than 4 years after a death.
The ABS Causes of Death data was used to identify ex-serving ADF males and Australian males who died by suicide. This data was then supplemented with the Deaths Registrations data which was used to identify the date of death. This allowed us to identify ex-serving ADF males and Australian males who died by suicide between 9 August 2011 and 31 December 2018. The deaths data in the linked PMKeyS–NDI data set was used to confirm the ex-serving ADF male deaths.
Data linkage, also known as data integration, is a process that brings together information relating to an individual from more than one source. This report utilised probabilistic linkage between the following data sets: linked PMKeyS-NDI, the 2011 Census of Population and Housing, and ABS Causes of Death / Deaths Registrations data.
After undergoing data checking and cleaning, the PMKeyS–NDI data set was linked using a probabilistic data linkage to the AIHW/ABS interoperable spine. This spine allows data held by both organisations to be linked without the need for sharing any identifiable information. The data was linked to the spine by matching by name, sex and date of birth. The linkage procedure involved creating record pairs—one from each data set—by running a series of passes that allow for variation in full name information demographic data. There were over 129,000 links found in the PMKeyS-NDI-interoperable spine linkage. This linkage was carried out by the Data Linkage Unit at the AIHW. This data set was then transferred to the ABS to be linked to the MADIP spine. AIHW staff, using the ABS DataLab environment were subsequently able to link the PMKeyS-NDI data to 2011 Census records and ABS Causes of Death data using the linkages of these data sets to the MADIP spine.
After removing the records of those ADF members who were out of scope, this resulted in an in-scope population of 45,700 links who were aged between 17 and 80 at Census, older than 16 at hire date, alive, and ex-serving at the time of the 2011 Census, who had served at least one day of service between 1 January 2001 and 30 June 2011. The ABS Cause of Death and Deaths Registrations data was then used in MADIP to identify ex-serving ADF males and Australian males who died by suicide between 9 August 2011 and 31 December 2018. The deaths data in the linked PMKeyS–NDI data set was used to confirm the ex-serving ADF male deaths.
Strict separation of identifiable information and content data is maintained within the Data Linkage Units at both AIHW and the ABS, so that no one person will ever have access to both. Summary results from the linked data set are presented in aggregate format. Personal identifying information is not released, and no individual can be identified in any reporting.
Figure 10 illustrates the linkage process undertaken for this report.
Figure 10: Linkage process
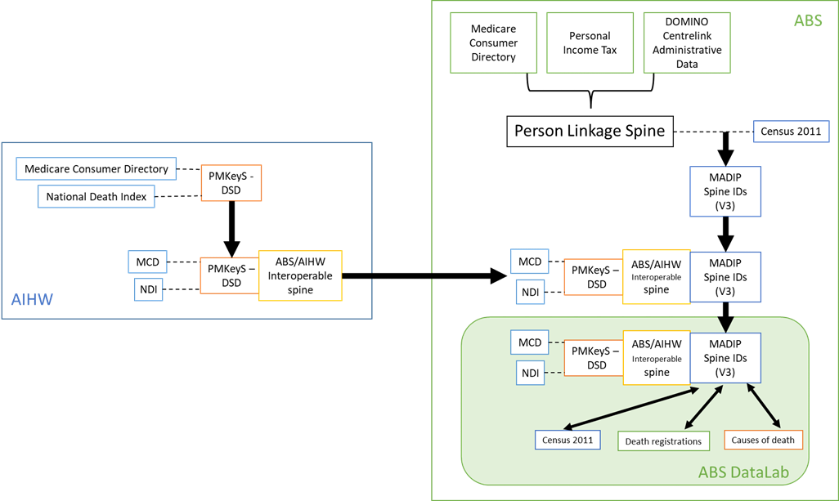
Note: ABS – Australian Bureau of Statistics, AIHW – Australian Institute of Health and Welfare, DOMINO - Data Over Multiple Individual Occurrences, ID – Identification, MCD – Medicare Consumer Directory, NDI – National Death Index, PMKeyS – Personnel Management Key Solution
Age
The age was restricted to 17–80 years for both the ex-serving ADF males and Australian males to match the eligible ADF population. Furthermore, the minimum age at hire for ex-serving ADF males was capped at 16 years and above to remove any linkage errors.
Separation date
The ex-serving ADF population has been restricted to those who separated prior to 30 June 2011 to ensure the study population had separated from the ADF at the time of the 2011 Census. Separation year was used to calculate length of service and time since separation. The reference date for these service-related characteristics is 30 June 2011.
Australian population
Using the 2011 Census persons extract in MADIP, there were 21.7 million people accounted for who were at home on Census night (9 August 2011). In total, the linked 2011 Census population was 16.7 million (75% of the total Australian population at September 2011). Of the total linked 2011 Census population, 6.2 million were males aged between 17 and 80 and used to construct the Australian male comparator cohort for this study, of which around 9,000 died by suicide between 9 August 2011 and 31 December 2018.
The study population is limited to ADF members who were ex-serving and alive at the time of the 2011 Census (9 August 2011), and served at least one day since 1 January 2001 and separated on or prior to 30 June 2011.
The ex-serving ADF male study population does not include members who separated between 1 July 2011 and 9 August 2011, and those who separated before 1 January 2001.
Small numbers
Findings based on small numbers of events can fluctuate from year to year for reasons other than a true change in the underlying risk of the event. As suicide amongst the ex-serving ADF population is a relatively uncommon occurrence (i.e. a statistically rare event), analysis is limited by small numbers.
For example, analysis of ex-serving ADF females was not possible. For ex-serving ADF males, after disaggregating by selected demographic and socioeconomic characteristics reported in the 2011 Census, small number of observed suicides in the study population have also been encountered. This has meant limiting the analysis further, for example, disaggregating by age or service-related characteristics or confidentialising small cell counts. This has also limited the utility of proportion ratios and risk ratios in some areas. Such treatments have been footnoted in the data tables accordingly.
Linkage
The linkage processes only provide data for those ex-serving ADF members who had a 2011 Census record. An individual not having a 2011 Census record could be a result of:
- them being overseas at the time of the 2011 Census.
- them not having completed a Census record.
- linkage error due to coercion to a later spine, insufficient information for linkage, or the record not being available.
Furthermore, a commitment by ABS to not use names from the 2011 Census for data linkage purposes resulted in lower linkage rates due to less identifying information available for use (Biddle and Marasinghe 2021).
The 2011 Census data were analysed because whilst it results in fewer ex-serving ADF members (compared to 2016 Census); it provides a greater number of suicides to analyse. Notably a limitation of using the 2011 Census (compared to 2016 Census) is the information is less current.
Uncertainty in the estimates
All data are subject to some level of uncertainty. For the data presented in this analysis the sources of uncertainty include:
- Linkage error: Uncertainty is introduced when there is error in linking data sets. The data used in this report carries some risk of linkage error.
- Timeliness of data: Some of the data used in this analysis was collected on 2011 Census Night (9 August 2011) and are a snapshot in time. For the purposes of the analysis, the reported characteristics are assumed static for the duration of the scope period. However, these characteristics (e.g. education and employment status) can change over time, particularly for certain population groups. The use of out-of-date information introduces a source of error to the analysis.
- Small numbers of observed suicides: Suicides among ex-serving ADF males account for a small proportion of the data, and therefore have high margins of variability.
- Randomness in the timing of suicides: The number of deaths by suicide that occur in different time intervals of the same length are expected to fluctuate, even if the underlying population risk remains the same. The exact distribution of the counts is unknown. With deaths by suicide being a rare event, it is assumed in this report that the counts follow a Poisson distribution. If this is the case, then the level of uncertainty due to randomness decreases as the number of deaths by suicide in the study period increase.
Proportion ratios
Proportion ratios measure the degree of inequality between populations, i.e. comparing the proportion in one population to the same proportion in another population. Proportion ratios are sensitive to size of the populations, and are subject to volatility when used with small numbers, and so should be used with caution when comparing ex-serving ADF males who died by suicide to the Australian male population who died by suicide.
The proportion ratio is calculated by dividing the proportion in a study group by the proportion in a control group.
Figure 11: Formula for calculating proportion ratios
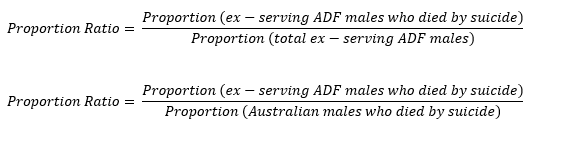
When the proportion ratio is greater than 1, it suggests an increased risk of the outcome in the study group. When a proportion ratio is less than 1, it suggests a reduced risk of the outcome in the study group. If the proportion ratio is 1 or close to one, it suggests no difference or little difference in risk.
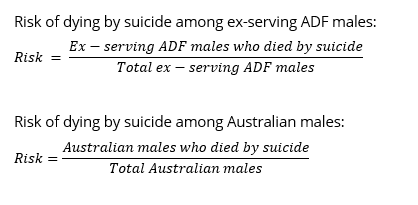
Risk (Incidence proportion/Cumulative incidence)
Risk, otherwise known as incidence proportion or cumulative incidence, is the proportion of a population at risk that develops the outcome of interest (in this case, death by suicide) over a specified time period (in this case, during the study period between 9 August 2011 and 31 December 2018 inclusive). Utilising this statistical measure required the 2011 Census data to run under the assumption that any socioeconomic characteristics reported at the time of the 2011 Census persisted until the end of the study period without migration into or out of the population, as it represented a static snapshot in time without a temporal component. Risk per 100,000 for the study period can be found in the accompanying supplementary data tables (Table S3).
Figure 12: Formula for calculating risk
Risk ratios
Risk ratios (RR), also referred to as relative risk, is a measure that gives an indication of the strength of an association. The RR is calculated by dividing the risk in an exposed group by the risk in an unexposed group. For example, the Australian males is the unexposed population, while the ex-serving ADF males is the exposed population. In this report, risk ratios were estimated without controlling for other socioeconomic characteristics. RRs are subject to volatility when used with small numbers, and so should be interpreted with caution when comparing risks among ex-serving ADF male subgroups or between ex-serving ADF males and Australian males.
Figure 13: Formula for calculating risk ratios
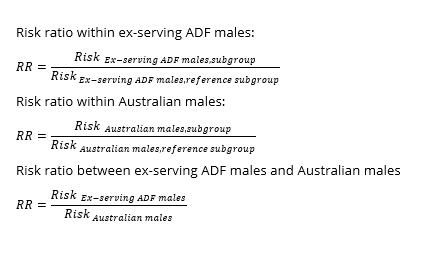
When a RR is greater than 1, it suggests an increased risk of the outcome in the exposed group. When a RR is less than 1, it suggests a reduced risk of the outcome in the exposed group. If a RR is 1 or close to one, it suggests no difference or little difference in risk.
Using confidence intervals to test for statistical significance
This report uses confidence intervals of 95% in the calculation of proportion ratios and risk ratios. Broadly speaking, wider confidence intervals (CIs) imply less certainty around a calculated value, and narrower CIs imply more certainty. Specifically, a CI at 95% suggests that repeated samples calculating the CI in the same manner would contain the true value 95% of the time.
Statistical significance is a measure that indicates how likely it is that an observed difference, or a larger one, would occur under the conditions of the null hypothesis.
In this study, 95% CIs are provided for the proportion ratios and risk ratios to indicate the level of uncertainty around these estimates due to random fluctuations in the number of suicides. It has been assumed that the number of suicides observed in the ex-serving ADF male population within the study period is random and follows a Poisson distribution. Estimates produced using low numbers can be sensitive to small changes in numbers of deaths over time and will therefore have wide CIs. 95% CIs are provided within this report as they may account for the variation in absolute numbers of deaths by suicide. It is important to note that there are other sources of uncertainty, such as data collection error and linkage error, that are not captured by the provided CIs.
Use of CIs is the simplest way to test for significant differences between ex-serving groups and Australian comparison groups. For the purpose of this report, differences are deemed to be statistically significant if CIs do not overlap with 1.0 for proportion ratios or risk ratios.
The AIHW thanks and acknowledges the large contribution by staff from a range of organisations in providing datasets and advice. These organisations are:
- Department of Defence
- Department of Veteran’s Affairs
- Australian Bureau of Statistics
- Royal Commission into Defence and Veterans Suicides
The AIHW also thanks and acknowledges contributions of internal staff from the AIHW; Data Integration Service Centre who conducted the data-linkage, Ethics Privacy and Legal Unit who facilitated the ethics approval process, Specialist Capability Unit who provided statistical guidance in the methods used for analysis and the Suicide and Self-Harm Monitoring Unit for advice on reporting on MADIP data for suicide analysis.
| ABS | Australian Bureau of Statistics |
|---|---|
| ADF | Australian Defence Force |
| AIHW | Australian Institute of Health and Welfare |
| Air Force | Royal Australian Air Force |
| Army | Australian Army |
| DVA | Department of Veterans’ Affairs |
| PMKeyS | Personnel Management Key Solution |
| Navy | Royal Australian Navy |
| NMD | National Mortality Database |
| NDI | National Death Index |
ABS (Australian Bureau of Statistics) 2011, Census of Population and Housing: Census Dictionary, 2011, May 2011. Cat. no: 2901.0. Canberra: ABS.
ABS (2016), Housing Circumstances of People Using Mental Health Services and Prescription Medications.
ABS (2021), Causes of Death, Australia Methodology.
ABS (2022) Multi-Agency Data Integration Project (MADIP) | Australian Bureau of Statistics (abs.gov.au), ABS.
AIHW (Australian Institute of Health and Welfare) (2018a), A profile of Australia’s veterans 2018. Cat. no. PHE 235. Canberra: AIHW.
AIHW 2018b. Canberra: AIHW. 18 June 2019. About National Death Index.
AIHW (2020), Australia’s health 2020.
AIHW (2021a), Serving and ex-serving Australian Defence Force members who have served since 1985: suicide monitoring 2001 to 2019. Cat. no. PHE 290. Canberra: AIHW.
AIHW (2021b), Final report to the Independent Review of Past Defence and Veteran Suicides. Cat. no. PHE 295. Canberra: AIHW.
AIHW (2021c), Australia’s welfare 2021: in brief. Cat. no. PHE 237.
AIHW (2021d) Housing affordability. Cat. no. PHE 237.
AIHW (2022), Understanding the wellbeing characteristics of ex-serving ADF members. Cat no. PHE 303. Canberra: AIHW.
Baker, D, Rice, S, Sadler, N, Cooper, J and Wade, D 2017, The Next Post: Young people transitioning from military service and their mental health. Melbourne: Orygen, The National Centre of Excellence in Youth Mental Health, 2017.
Biddle, N and Marasinghe, D. (2021) Using census, social security and tax data from the Multi-Agency Data Integration Project (MADIP) to impute the complete Australian income distribution
DSS (Department of Social Services) (2015) A new system for better employment and social outcomes. Canberra: DSS.
DVA (Department of Veterans’ Affairs) (2011). Mental Health and Wellbeing after Military Service.
Defence (Department of Defence) (2017). ADF member and family transition guide: a practical manual to transitioning.
Harrod M, Miller E, Henry J & Zivin K 2017, ‘I’ve never been able to stay in a job’: a qualitative study of veterans’ experiences of maintaining employment. Work 57: 259 – 268
Hawthorne G, Korn S & Creamer M 2014, Australian peacekeepers: long-term mental health status, health service use, & quality of life – summary report. Melbourne: University of Melbourne.
Jones, K, Varker, T, Stone, C, Agathos, J, O’Donnell, M, Forbes, D, Lawrence-Wood, E & Sadler, N 2020, Defence Force and Veteran suicides: Literature review. Report prepared for the Australian Commission on Safety and Quality in Health Care. Phoenix Australia – Centre for Posttraumatic Mental Health: Melbourne.
Lin N, Simeone R, Ensel W & Kuo W 1979, Social support, stress life events, and illness: a model and an empirical test. Journal of Health and Social Behaviour 20:108 – 119
National Mental Health Commission (NMHC) 2017, Review into the Suicide and Self-Harm Prevention Services Available to current and former serving ADF members and their families, Final Report, 28 March 2017.
Open Arms, 2019 Protective factors
Ozbay F, Johnson DC, Dimoulas E, Morgan CA, Charney D, Southwick S 2007, Social support and resilience to stress: from neurobiology to clinical practice. Psychiatry (Edgmont) 2007; 4:35 – 40
Parliament of Australia 2022, Royal Commission into Defence and Veteran Suicide Interim Report.
PMC (Department of the Prime Minister and Cabinet) (2022). Data Integration.
Productivity Commission 2019, A Better Way to Support Veterans, Report no. 93, Canberra.
The Senate Foreign Affairs, Defence and Trade References Committee (SFADTRC) inquiry into Suicide by Veterans and Ex-Service Personnel, The Constant Battle: Suicide by Veterans (The Senate Foreign Affairs Defence and Trade References Committee, 2017)
von Sanden N (2020). ‘Improving Inter-Agency Data Sharing Through Linkage Spine Interoperability’, International Journal of Population Data Science, 5(5). DOI: 10.23889/ijpds.v5i5.1577.