Chronic musculoskeletal conditions:
All arthritis
Web article
Last updated:
Topic: Musculoskeletal conditions
Citation
AIHW (Australian Institute of Health and Welfare) (2024) All arthritis, AIHW, Australian Government, accessed 19 July 2026.
This article is part of Chronic musculoskeletal conditions
Figure 1: Prevalence of arthritis, by age and sex, over time (2001 to 2022) by population group, 2022
This figure shows that the prevalence of people living with other type of arthritis increased with increasing age.

Prevalence in Aboriginal and Torres Strait Islander (First Nations) people
The Australian Institute of Health and Welfare (AIHW) uses ‘First Nations people’ to refer to Aboriginal and/or Torres Strait Islander people in this report.
In 2018–19, around 85,600 (11%) First Nations people were estimated to have arthritis, based on the National Aboriginal and Torres Strait Islander Health survey (NATSIHS), similar to that reported in 2012–13 (10%) (ABS 2019).
Impact of arthritis
Arthritis can have a profound impact on a person’s quality of life and wellbeing due to acute and chronic pain, physical limitations, management of the condition and mental health impacts (Briggs et al. 2016; Sharma et al. 2016).
Although arthritis affects people of all ages, its prevalence increases sharply from the age of 45 years.
Measures of impact presented in this section include burden of disease, health expenditure and mortality data.
Burden of disease
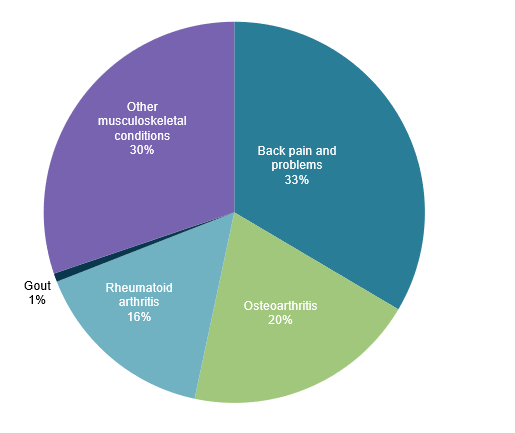
Common forms of arthritis (osteoarthritis, rheumatoid arthritis and gout) are large contributors to illness, pain and disability in Australia. Based on data from the Australian Burden of Disease Study 2023, musculoskeletal conditions were responsible for 13% of the total burden of disease (approximately 723,000 disability-adjusted life years or DALY). Of this proportion:
- osteoarthritis contributed 20% of disease burden
- rheumatoid arthritis contributed 16%
- gout contributed 0.7%.
The remaining burden was attributed to ‘other musculoskeletal conditions’ (30%) and ‘back pain and problems’ (34%) (Figure 2) (AIHW 2023a).
For more information, see Osteoarthritis, Rheumatoid arthritis and Gout.
Figure 2: Musculoskeletal conditions burden (Disability-adjusted life years), by disease, 2023
Source: AIHW 2023a.
Health system expenditure
Arthritis significantly impacts the Australian economy. Increased health care costs and higher use of health care services (for example, general practitioners, specialists, allied health and pharmaceuticals) required to treat and manage arthritis represent direct financial costs to the health care system.
There are also indirect costs associated with arthritis and/or musculoskeletal conditions and comorbidities, such as productivity losses, disability support pensions and other welfare payments, early retirement and carer costs (Schofield et al. 2018; Arthritis Australia 2014).
In 2020–21, health expenditure for arthritis was estimated to be:
- $4.3 billion for osteoarthritis, representing 2.9% of total disease expenditure
- $966.1 million for rheumatoid arthritis, representing 0.6% of total disease expenditure (AIHW 2023b).
For more information, see Health system spending on disease and injury in Australia, 2020–21.
Treatment and management of arthritis
At present, there is no cure for arthritis, with treatment aiming to manage symptoms and maximise quality of life. Arthritis-related conditions are predominantly managed in primary health care settings by a range of health professionals.
What role do GPs play in managing arthritis?
Treatment of arthritis generally involves a combination of self-management (such as diet and exercise), education on living with the condition, physiotherapy, medication (for pain and inflammation), and referral to specialist care where necessary (WHO 2019).
It is worth noting that there is currently no nationally consistent primary health care data collection to monitor provision of care by GPs. See General practice, allied health and other primary care services.
What medicines are used to treat arthritis?
Medication is primarily used to manage symptoms of pain, inflammation and improve functioning and quality of life among people with arthritis. Medications can range from general over-the-counter analgesics (painkillers) to highly specialised medications and vary depending on the type and severity of the condition.
What role do hospitals play in treating arthritis?
Osteoarthritis was the most common type of arthritis hospitalisation in 2021–22, and as a principal diagnosis accounted for 2.1% of all hospitalisations. Rheumatoid arthritis and gout accounted for 0.1% each.
Joint replacement surgery may be required for those with severe arthritic conditions who are unresponsive to medication and exercise (RACGP 2018). These procedures restore joint function, help relieve pain and improve quality of life of the affected person. Osteoarthritis is the most common condition leading to hip and knee replacement surgery in Australia (AOANJRR 2019).
For more information on these conditions, see Osteoarthritis, Rheumatoid arthritis, Juvenile arthritis and Gout.
Comorbidities of arthritis
People with arthritis often have other long-term conditions known as ‘comorbidity'.
According to the NHS, in 2022, an estimated 2.7 million (74%) people who were living with arthritis also had one or more other chronic conditions (Figure 3) (ABS 2023).
Among people living with arthritis, mental and behavioural conditions were the most common comorbidity (38%), followed by back problems (36%) and asthma and heart, stroke and vascular disease (17% each) (Figure 3) (ABS 2023).
Figure 3: Number of selected chronic conditions and types of comorbidity in people with arthritis, 2022
This figure shows that 26% of people estimated to be living with arthritis reported not having any other selected chronic conditions.
