Chronic musculoskeletal conditions:
Rheumatoid arthritis
Web article
Last updated:
Topic: Musculoskeletal conditions
Citation
AIHW (Australian Institute of Health and Welfare) (2024) Rheumatoid arthritis, AIHW, Australian Government, accessed 27 July 2026.
This article is part of Chronic musculoskeletal conditions
Page highlights
Rheumatoid arthritis is a chronic autoimmune condition that causes inflammation, pain, swelling, stiffness and loss of function in joints, commonly in the hands.
How common is rheumatoid arthritis?
Around 514,000 (2.0%) people in Australia were estimated to be living with rheumatoid arthritis in 2022.
Impact of rheumatoid arthritis
- Rheumatoid arthritis accounted for 2.0% of total disease burden and 16% of the total burden of disease for all musculoskeletal conditions in 2023.
- In 2020–21, an estimated $966.1 million was spent on the treatment and management of rheumatoid arthritis, representing 0.6% of total health system expenditure and 6.6% of expenditure for all musculoskeletal conditions.
- Rheumatoid arthritis contributed to 1,322 deaths or 5.1 deaths per 100,000 population in 2022, representing 0.7% of all deaths.
Treatment and management of rheumatoid arthritis
In 2021–22, there were 10,000 hospitalisations with a principal diagnosis of rheumatoid arthritis (39 hospitalisations per 100,000 population).
What is rheumatoid arthritis?
Rheumatoid arthritis is a chronic autoimmune condition characterised by inflammation of the joints, pain, swelling, stiffness and loss of function in the joints. It commonly affects the hand joints and both sides of the body at the same time (CDC 2019).
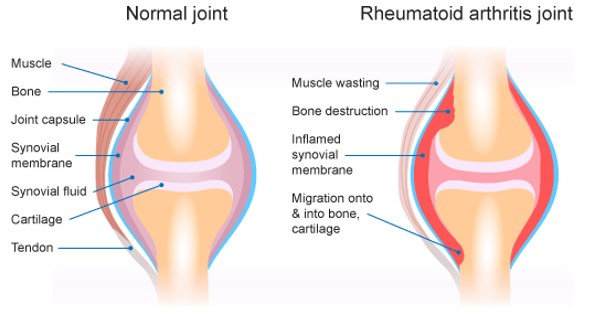
In a healthy joint, the tissue lining the joint (called the synovial membrane or joint synovium) is very thin and produces fluid that lubricates and nourishes joint tissues (RACGP 2009). In people with rheumatoid arthritis, the immune system attacks the synovial membrane which becomes thick and inflamed, resulting in unwanted tissue growth (Figure 1). As a result, bone erosion and irreversible joint damage can occur, leading to permanent disability (RACGP 2009).
Figure 1: Comparison of healthy joint and joint with rheumatoid arthritis
How common is rheumatoid arthritis?
Around 514,000 (2.0%) people in Australia were estimated to be living with rheumatoid arthritis, according to self-reported data in the 2022 Australian Bureau of Statistics (ABS) National Health Survey (NHS) (ABS 2023). This represented 14% of people living with any form of arthritis (excluding gout).
For more information about other forms of arthritis, see All arthritis, Osteoarthritis, Gout, and Juvenile arthritis.
Note: Unless otherwise stated, crude rates are presented for prevalence in this report and as such, these rates have not been adjusted to account for differences in the age structures of different populations. Care should therefore be taken before making comparisons between populations using these data.
According to the NHS, in 2022, rheumatoid arthritis was:
- most common in people aged 75 years and over (8.9%) (ABS 2023), although the onset of rheumatoid arthritis most frequently occurred in those aged 35–64 (AIHW 2023; Duarte-Garcia 2019)
- slightly more common in females compared with males (2.5% and 1.6%, respectively) (Figure 2) (ABS 2023).
Figure 2: Prevalence of rheumatoid arthritis, by age and sex, 2022
This figure shows that the prevalence of rheumatoid arthritis is lowest for people aged 44 and under and increases with increasing age.

Figure 3: Burden of disease due to rheumatoid arthritis by age and sex, 2003, 2011, 2015, 2018 and 2023
This figure shows the rate of total burden of disease for rheumatoid arthritis was highest for people aged 60–64 in 2023.

Figure 4: Burden of disease due to rheumatoid arthritis for remoteness area and socioeconomic area by sex, 2011, 2015 and 2018
This figure shows that the rate of total burden of disease for rheumatoid arthritis was highest for females living in the lowest socioeconomic areas in 2018.

Figure 5: Rheumatoid arthritis expenditure attributed to each area of the health system, with comparison to all disease groups, 2020–21
This figure shows that the primary care proportion of rheumatoid arthritis expenditure was $828 million (86%) in 2020-21.

Figure 6: Proportion of expenditure attributed to rheumatoid arthritis, for each area of the health system, 2020–21
This figure shows that rheumatoid arthritis accounted for 0.6% of pathology expenditure in 2020–21.

Figure 7: Age distribution for rheumatoid arthritis mortality, by sex, 2012 to 2022
This figure shows that in 2022, the death rate due to rheumatoid arthritis was highest for people aged 85 and over (89 deaths per 100,000 population).
Chart temporarily unavailable
Figure 8: Trends over time for rheumatoid arthritis mortality, 2012 to 2022
This figure shows that between 2012 and 2022, deaths rates due to rheumatoid arthritis increased from 3.8 to 5.1 deaths per 100,000 population.
Chart temporarily unavailable
Figure 9: Age distribution for rheumatoid arthritis hospitalisations, by sex, 2011–12 to 2021–22
This figure shows that the hospitalisation rate for rheumatoid arthritis increased with increasing age up to the 75–79 age group, decreasing thereafter.

Figure 10: Trends over time for rheumatoid arthritis hospitalisations, 2011–12 to 2021–22
This figure shows that between 2011–12 and 2021–22, hospitalisation rates for rheumatoid arthritis were consistently higher for females compared with males.
