Chronic musculoskeletal conditions:
Osteoporosis and minimal trauma fractures
Web article
Last updated:
Topic: Musculoskeletal conditions
Citation
AIHW (Australian Institute of Health and Welfare) (2024) Osteoporosis and minimal trauma fractures, AIHW, Australian Government, accessed 10 July 2026.
This article is part of Chronic musculoskeletal conditions
- All arthritis
- Back problems
- Chronic musculoskeletal conditions in Australia
- Gout
- Juvenile arthritis
- Osteoarthritis
- Osteoporosis and minimal trauma fractures This page
- Rheumatoid arthritis
Page highlights
- Osteoporosis is a chronic condition defined by low bone mineral density, which increases the risk of fractures.
- Osteopenia refers to bone-mineral density that is lower than normal but not low enough to be classified as osteoporosis.
Around 853,600 (3.4%) people in Australia were estimated to be living with osteoporosis or osteopenia in 2022. The true prevalence, including undiagnosed cases, is likely to be higher than this.
- 29% of fall burden was attributed to low bone mineral density, equivalent to 0.4% of total disease burden in 2018.
- In 2018–19, an estimated $1.2 billion or 29% of expenditure for falls was attributed to low bone mineral density, representing 1.9% of total health system expenditure.
- Osteoporosis contributed to 2,659 deaths or 10.2 deaths per 100,000 population in 2022, representing 1.4% of all deaths.
Treatment and management of osteoporosis and minimal trauma fractures
- In 2021–22, there were 9,500 hospitalisations with a principal diagnosis of osteoporosis (89 hospitalisations per 100,000 population) for people aged 45 and over.
- There were 105,000 hospitalisations for minimal trauma fractures in people aged 45 and over in 2021–22, 28% of these were hip fractures.
- The rate of minimal trauma hip fractures decreased consistently from 2017–18, possibly reflecting measures to reduce risk factors and prevent falls.
In 2022, 79% of people estimated to be living with osteoporosis were also living with one or more other chronic conditions – the top 3 comorbidities were arthritis (44%), back problems (35%) and mental and behavioural conditions (34%).
What is osteoporosis?
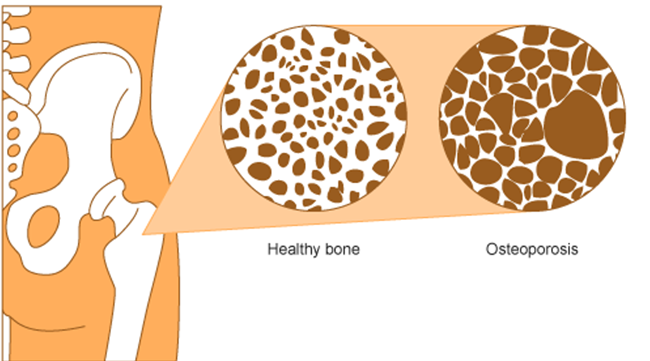
Osteoporosis (meaning 'porous bones') is a condition that arises when bones become less dense, lose minerals such as calcium and are more fragile (Figure 1) (Health Direct 2023; Healthy Bones Australia 2023).
Minimal trauma fractures (broken bones) are a major feature of osteoporosis and are fractures that that occur following little or no trauma. Fractures due to osteoporosis can result in chronic pain, disability, loss of independence and premature death (Bliuc et al. 2013).
Figure 1: Visual representation of a healthy bone and bone with osteoporosis
Osteopenia is a condition where bone density is lower than normal but not low enough to be classified as osteoporosis. It can progress to osteoporosis.
Diagnosis of osteoporosis requires an assessment of bone mineral density (BMD). The most commonly used technique used for this is a specialised X-ray known as a 'Dual energy X-ray Absorptiometry (DXA) scan' (IOF 2017). Scan results are expressed as T‑scores which are compared to an average score of young healthy adults for diagnosis (Table 1) (WHO 1994).
| Normal | Osteopenia | Osteoporosis | |
|---|---|---|---|
| T-Score | 1 to -1 | -1 to -2.5 | -2.5 or lower |
Source: WHO Study Group 1994.
Because osteoporosis has no overt symptoms, it is often not diagnosed until a fracture occurs. It is therefore difficult to determine the true prevalence of the condition and reported prevalence is likely to be an underestimation.
What causes osteoporosis and osteopenia?
Osteoporosis is largely a preventable disease. Risk factors associated with the development of osteoporosis include increasing age, being female, family history of the condition, low vitamin D levels, low intake of calcium, low body weight, smoking, excess alcohol consumption, physical inactivity, long-term corticosteroid use and reduced oestrogen level (Ebeling et al. 2013).
Primary prevention of osteoporosis involves taking calcium and vitamin D supplements, behaviour modification such as regular weight-bearing and resistance exercise, keeping alcohol intake low and not smoking, and fall reduction strategies, such as addressing vision impairment or making home modifications (RACGP 2018).
The goal of the prevention and treatment of osteoporosis is to maintain bone density and reduce a person’s overall fracture risk (RACGP 2018).
How common is osteoporosis?
Around 853,600 (3.4%) people in Australia were estimated to be living with osteoporosis or osteopenia, according to self-reported data in the 2022 Australian Bureau of Statistics (ABS) National Health Survey (NHS) (ABS 2023).
Note: Unless otherwise stated, crude rates are presented for prevalence in this report and as such, these rates have not been adjusted to account for differences in the age structures of different populations. Care should therefore be taken before making comparisons between populations using these data.
In 2022, the prevalence of osteoporosis and osteopenia collectively:
- increased substantially with increasing age, from 0.7% of people aged 35–44, to 17% of people aged 75 and over
- was higher among women compared with men (5.5% and 1.1%, respectively)
- was highest for women aged 75 and over (26%)
- changed little by remoteness or level of disadvantage (also known as socioeconomic area) (Figure 2) (ABS 2023).
After adjusting for different population age structures over time, the prevalence of osteoporosis increased from 1.6% in 2001 to 2.7% in 2022 (ABS 2023).
Figure 2: Prevalence of osteoporosis, by age and sex, over time (2001 to 2022), by population group, 2022
This figure shows that the prevalence of osteoporosis or osteopenia was almost 5 times as high for females compared with males for those aged 55 to 74.

Figure 3: Age distribution for osteoporosis mortality, by sex, 2012 to 2022
This figure shows that death rates due to osteoporosis increased after the age group 65–69 and were highest for people aged 85 and over in 2022.
Chart temporarily unavailable
Figure 4: Trends over time for osteoporosis mortality, 2012 to 2022
This figure shows that between 2012 and 2022, death rates due to osteoporosis were highest in 2022 and lowest in 2013.
Chart temporarily unavailable
Figure 5: Age distribution for osteoporosis hospitalisations, by sex, 2021–22
This figure shows that there were 2,600 hospitalisations with a principal diagnosis of osteoporosis for people aged 85 and over in 2021-22.

Figure 6: Trends over time for osteoporosis hospitalisations, 2011–12 to 2021–22
This figure shows that between 2011–12 to 2021–22, the number of hospitalisations with a principal diagnosis of osteoporosis increased from 6,400 to 10,100.

Figure 7: Trends over time for minimal trauma fracture hospitalisations, by fracture site, age and sex, 2015–16 to 2021–22
This figure shows minimal trauma fracture hospitalisations for persons aged 45 and over were higher for females for all fracture sites compared with males.

Figure 8: Age distribution for minimal trauma fracture hospitalisations, by sex, 2015–16 to 2021–22
This figure shows minimal trauma fracture hospitalisations for people aged 85 and over were higher for hip fractures compared with other fracture sites.

Figure 9: Number of selected chronic conditions and types of comorbidity in people with osteoporosis, 2022
This figure shows that 20% of people estimated to be living with osteoporosis reported not having any of the other selected chronic conditions.
