Technical notes
The National Drug Strategy Household Survey (NDSHS) has been conducted every 2 to 3 years since 1985. This is the 14th survey in the series and the 9th to be managed by the Australian Institute of Health and Welfare (AIHW) on behalf of the Department of Health and Aged Care. Roy Morgan Research (RMR) was commissioned by the AIHW to conduct the survey fieldwork.
Methodology
2022–2023 NDSHS results are based on information obtained from people aged 14 and over from all states and territories in Australia. Unless otherwise specified, estimates presented from the NDSHS refer to people in Australia aged 14 and over.
Sample design
In line with the previous NDSHS waves, the sample was selected using stratified, multistage random sampling. There were 15 strata in total, including the capital city and ‘rest of state’ for each state and territory, with the exception of the Australian Capital Territory, which operated as one stratum.
To produce reliable estimates for the smaller states and territories, sample sizes were boosted in Tasmania, the Australian Capital Territory (ACT) and the Northern Territory (NT) with the goal of achieving a minimum of 1,000 completed questionnaires in each jurisdiction.
The sample size allocated to Western Australia (WA) and SA was proportional to the population living in each state, as a fraction of the Australian population. In 2022–2023, an additional 1,509 questionnaires were purchased by South Australia (SA) to improve reliability of results.
The remaining sample was allocated between New South Wales (NSW), Victoria (VIC), and Queensland, in proportion to the population living in each state. This results in an under sampling of these three jurisdictions (proportional to their share of the Australian population) due to the over sampling in Tasmania, ACT and NT.
For capital city strata, statistical areas level 1 (SA1s) were selected with probability proportional to the number of private households calculated from the Australian Bureau of Statistics Household and Family Projections, 2016 to 2041 (ABS 2019).
As in 2019, six large urban areas were identified for sample selection in the same way as major cities. These regional centres of Newcastle and Illawarra in NSW, Geelong in Victoria, Gold Coast, Sunshine Coast, and Cairns in Queensland also used this SA1 selection process, to reduce geographical clustering within the sample.
In 2022–2023, if SA1s with fewer than 50 households (based on Household and Family Projections, 2016 to 2041, ABS 2019) were selected, they were replaced with other SA1s with similar characteristics with respect to region, remoteness status and Socio-Economic Indexes for Areas (SEIFA) status based on the Index of Relative Socioeconomic Advantage and Disadvantage (IRSAD), within the same SA2 where possible.
In all other areas in the ’rest of state’ strata, statistical areas level 2 (SA2s) were selected for the first stage, as this had considerable efficiency benefits. SA2s for each stratum were selected with probability proportional to the number of households calculated from Household and Family Projections, 2016 to 2041 (ABS 2019). Within each selected SA2, SA1s were selected with probability proportional to the number of private households, calculated in the same way.
An additional six SA1s were selected using the same process (that is, beginning from the SA2 selection stage) but were limited to those SA1s classified by the ABS Australian Statistical Geography Standard (ASGS) Remoteness structure as Remote Australia or Very Remote Australia, in an effort to increase the proportion of Remote and Very remote households in the sample.
A starting address within each selected SA1 was randomly selected, and interviewing started at the dwelling next door to the selected household. Interviewers followed a comprehensive set of procedures to select a dwelling, including skip intervals, identifying eligible and ineligible addresses, and dealing with blocks of flats and units.
As in previous surveys, interviewers made 3 attempts to establish face-to-face contact with the selected dwellings. The selected respondent was the household member aged 14 or older who most recently celebrated their birthday. This was a departure from samples from 2004–2016, where the selected respondent was a household member aged 12 or older. In 2019, the NDSHS Technical Advisory Group made the decision to remove 12- and 13-year-olds from the sample. There were some concerns over the reliability of the data collected as the majority of 12- and 13-year-olds reported that their parents were present while completing the survey and that this affected the honesty of their responses. This population group is also captured through other drug and alcohol surveys such as the Australian Secondary Schools Alcohol and other Drug survey. If the selected respondent was aged 14 or 15, permission was sought from a responsible adult for them to complete the survey.
Scope and coverage
The NDSHS contains two sets of estimates. One set reports statistics for households (for example, the proportion of households where residents are exposed to tobacco smoke), and the other reports statistics for people in Australia (for example, the proportion of people who smoke tobacco daily). The scope for these two sets of estimates is:
- Residential households in Australia containing at least one person aged 14 years or over who resides at that household permanently.
- People aged 14 and over who reside in in-scope households (only one person may be selected in each household).
The scope excludes institutional settings such as hospitals and nursing homes, non‑permanent addresses such as motels and hostels, and other environments such as Defence Force barracks or prisons, as well as the people residing in those settings. It also excludes people without a permanent address, such as those experiencing homelessness.
It is not possible to achieve full coverage of this scope within Australia. Any SA1 where the standard NDSHS placement procedures could not be followed was removed from the sample and replaced, due to being out of scope. This includes Aboriginal and Torres Strait Islander (First Nations) communities where First Nations languages are the primary spoken language. It also includes residential households outside the 15 sample strata, and households in SA1s that have fewer than 50 total residences, as well as the people who reside in those households.
As each household could only have one respondent, and in-scope households must have at least one eligible person aged 14 and over residing there, the number of households contacted and the number of people contacted are equivalent for the purposes of response-rate calculations and sample size comparisons.
Cognitive testing, pilot procedures and fieldwork
Cognitive testing was conducted by Roy Morgan between 10 and 24 February 2022. This involved asking twenty-five participants to complete a condensed version of the questionnaire, followed by an interview to understand how they interpreted the questions in the survey to ensure new and updated questions were worded appropriately.
Formal pilot testing was conducted between 26 April and 18 May 2022. This involved conducting interviews in 24 SA1s across Brisbane and Southern Queensland, to test changes to the fieldwork process such as including an incentive.
Fieldwork timing
Initially, the NDSHS was scheduled to be conducted from 20 July 2022 to 7 December 2022. Due to workforce limitations, however, it was estimated that less than two-thirds of the target sample size would be achieved in this timeframe. The Department of Health and Aged Care and the AIHW determined that the priorities for the NDSHS were:
- To achieve a sample size as close to the target as possible.
- To do everything possible to ensure the entire sample could be used to generate NDSHS results (that is, ensure the remaining sample would not be substantially different to the sample collected in 2022).
- To ensure the remaining sample included 14- and 15-year-olds as a priority area of interest for tobacco, vaping, alcohol, and illicit drug statistics.
To meet these priorities, the collection period in 2022 was extended to the 18 December 2022. In addition, a second fieldwork period using the same methodology was scheduled for 2023.
It was expected that alcohol and drug use would change over the Christmas period and holidays at the end of December. To avoid this having an impact on the collected data, the second fieldwork period was not scheduled to begin until 20 March 2023 and continued to 31 May 2023.
Analysis indicated, for a majority of alcohol, tobacco, and illicit drug variables, the two fieldwork periods were comparable. Results from the 2022–2023 NDSHS use data collected throughout both fieldwork periods.
Survey modes
The 2022–2023 survey was conducted using a multi-mode completion methodology, similar to the 2016 and 2019 surveys. Selected individuals could choose to complete the survey via a paper form, an online form, or a telephone interview. In 2022–2023, 28% of respondents chose to complete the survey online, an increase from the 25% of respondents that did so in 2019. Between 2019 and 2022–2023, respondents choosing to complete the survey via paper form dropped from 74% to 72%, while those completing the survey via telephone dropped from 0.3% to 0.1%.
Survey modes have changed over time with survey waves. Table 1 provides a summary of the data collection methodologies and fieldwork timing since 1998, when AIHW began managing the survey. Changes to the methodology should be taken into consideration when making comparisons over time.
For households electing to complete the paper questionnaire, 3 attempts were made to personally collect the questionnaire. Interviewers also made reminder phone calls or sent an SMS to the selected respondent before each pick-up attempt. If they were still unable to pick up the questionnaire after three attempts, a reply-paid envelope was left for the respondent to mail the completed questionnaire back to Roy Morgan Research. In the follow-up phone call, respondents were given the option to switch from the paper form to the online form.
For respondents electing to complete online, the survey link was provided to the respondent, and was accessible immediately by entering the form number provided on the paper survey. The online survey could also be accessed using a QR code provided on the physical survey form. Where an email address or mobile phone number was provided, an email or SMS invitation was also sent, generally the next day, which linked the respondent directly to their online survey. Up to 3 reminder emails were sent at 3-day intervals to encourage response. A final email or SMS reminder was sent approximately one month after the respondent was selected if the survey had not been completed.
For respondents electing to complete by telephone, the interviewer collected up to four separate times that would be suitable to contact the respondent for an interview. If contact was made at the household, but the respondent was not available, or if the time was no longer suitable for the respondent, an alternative time was arranged to conduct the interview.
If no response had been received from respondents electing to complete online or via phone after three attempts, the face-to-face interviewer visited the household to remind them to complete the survey, including providing the option to complete by paper. A reply-paid envelope was also left, in case the respondent preferred to complete by paper.
| Year | Data collection methodology | Total complete questionnaires | Fieldwork conducted |
|---|---|---|---|
1998 | Personal interviews (40%) | 10,030 | June–September 1998 |
| Drop and collect (60%) | ||
2001 | Personal interviews (8%) | 26,744 | June/July–November 2001 |
| Drop and collect (85%) |
|
|
| CATI (8%) |
|
|
2004 | Drop and collect (82%) | 29,445 | June/July–November 2004 |
| CATI (18%) |
|
|
2007 | Drop and collect (85%) | 23,356 | June/July–November 2007 |
| CATI (15%) |
|
|
2010 | Drop and collect (100%) | 26,648 | April–September 2010 |
2013 | Drop and collect (100%) | 23,855 | July–December 2013 |
2016 | Drop and collect, paper form (78%) | 23,722 | June–November 2016 |
| Online survey (22%) |
|
|
| CATI (0.3%) |
|
|
2019 | Drop and collect, paper form (74%) | 22,274 | April–September 2019 |
| Online survey (25%) |
|
|
| CATI (0.3%) |
|
|
2022–2023 | Drop and collect, paper form (72%) | 21,663 | 20 July–18 December 2022 |
| Online survey (28%) |
| 20 March–31 May 2023 |
| CATI (0.1%) |
|
|
Note: CATI stands for Computer Assisted Telephone Interview.
Source: NDSHS 2022–2023, Table 12.1.
Mode effects
It is possible that the mode used by a respondent could have an impact on the actual information provided, introducing a bias in the data and affecting comparability of data obtained via the different methods.
Like the 2016 and 2019 surveys, respondents who elected to use the online form had different demographic characteristics to respondents who used the paper form. Not only do demographic characteristics of respondents affect their choice of survey mode, they are also related to their likelihood of reporting drug use. For example, young people were more likely to have used e‑cigarettes in the previous 12 months and were also more likely to complete the survey online. Due to this fact, if online completions and paper completions were simply compared, online respondents would appear to be more likely to use e‑cigarettes than paper respondents. As a result, comparisons between modes require adjustments to be made based on demographic differences between the people using the different modes.
Respondents using different modes were significantly different to each other in terms of gender, age, employment status, highest level of education attained, marital status, main language spoken at home, household status, remoteness, socioeconomic area, and sexual orientation. These demographic characteristics need to be taken into account when assessing potential mode effects.
Variables related to the use of tobacco, alcohol, and other illicit drugs were tested for mode effects. The impacts of the significant socio-demographic variables were first tested to understand their impacts on the responses. Logistic regression analysis was used to test for mode effects, controlling for the known demographics of respondents.
Modelling suggested no statistically significant differences between paper and online completions for the following results, after adjusting for known demographic characteristics:
- recent consumption of alcohol,
- recent non‑medical use of pain-killers/pain-relievers and opioids,
- recent non‑medical use of pharmaceutical stimulants,
- recent use of cocaine,
- recent use of ecstasy
- recent use of ketamine,
- recent use of inhalants.
However, compared with people who completed the online form, those who completed the paper form were (after adjusting for known demographic characteristics):
- 1.6 times as likely to consume more than 4 standard drinks in a single day at least once a month.
- 1.5 times as likely to have recently used methamphetamine and amphetamine.
- 1.5 times as likely to have recently used tranquillisers/sleeping pills for non‑medical purposes.
- 1.4 times as likely to consume alcohol at risky levels and to consume more than 10 standard drinks per week on average.
- 1.4 times as likely to currently smoke.
- 1.3 times as likely to have recently used hallucinogens.
- 1.2 times as likely to have recently used cannabis.
These differences between paper and online responses should be taken into account when considering 2022–2023 estimates of drug use prevalence, especially when comparing them to other years. In 2016, the same multi-mode approach was used, and 22% of people completed the survey online, compared to 25% in 2019, and 28% in 2022–2023 (see Table 1).
The increase in online respondents may have caused, for example, a slight decline in the prevalence estimates for smoking, although not enough to account for the significant declines in daily smoking between 2019 and 2022–2023. Surveys conducted before 2016 used various collection methods, so caution should be exercised when comparing 2022–2023 results to previous years.
Weighting
The survey sample was designed to provide a random sample of households within each geographic stratum, with a single person selected within each household to complete the survey. Respondents within each stratum were assigned weights to account for selection probabilities, adjustments for non‑response, and other known differences between the selected sample and the entire population. Weighting also adjusts for the under-sampled and over-sampled strata, to bring them back in line with the proportion of the population living in each stratum.
Two main sets of weights are used in the 2022–2023 NDSHS:
- The main person-level weighting for the 2022–2023 NDSHS considered factors including geographical stratification, household size, age, and gender. Weight totals will match the population estimates for the relevant timeframe.
- The household-level weighting considered geographical stratification and sample selection processes, but not the factors that affected respondent selection such as household size. Weight totals will match the projected household estimates for the relevant timeframe.
Adjusting for changes to sex and gender variables in the 2022–2023 NDSHS
In 2022–2023, the NDSHS was adapted to use questions from the ABS Standard for Sex, Gender, Variations of Sex Characteristics and Sexual Orientation Variables (2020). This change was undertaken to ensure that people would be able to respond to the survey accurately and feel represented, and to allow for results to be presented for cisgender and trans and gender diverse populations.
This has had an impact on the weighting scheme. In prior years, weights were calculated based on the response to the question ‘what is your sex?’. In 2022–2023, two questions were asked, ‘what was your sex recorded at birth’ and ‘how do you describe your gender?’. However, weights must be calculated using population estimates from the 2021 Census, which still used the question ‘what is your sex?’.
To weight against the Census data, the AIHW created a binary weighting variable based primarily on the response to the gender question. Gender was chosen rather than sex at birth because, in the absence of a gender question, people may be likely to respond to a sex question with their gender (ABS 2022a). If the response to the gender question was not male or female, a series of subsequent checks were conducted before using random allocation, reflecting the assignment of the Census variable (ABS 2022a).
This represents a deviation from previous surveys, but due to the small number of responses where this process would result in a different weight being assigned, it does not represent a break in the time-series.
Calculation of weights
The population estimates used for the weighting were based on the latest available age profile using the published ABS Estimated Resident Population data (ABS 2022b). This series provided the necessary level of age breakdown by State/Territory, but not by stratum. The stratum level population estimates were projected from the regional ERP series (ABS 2021).
All estimates in the report are based on the weighted sample. Table 2 provides a comparison of the age and gender profile of both the sample and the estimated resident population.
Age | Unweighted | Unweighted | Unweighted | Weighted | Weighted | Weighted |
|---|---|---|---|---|---|---|
14–17 | 1.3 | 1.3 | 2.6 | 3.1 | 2.8 | 6.0 |
18–24 | 2.7 | 3.0 | 5.7 | 5.5 | 4.9 | 10.4 |
25–29 | 2.8 | 3.4 | 6.2 | 4.2 | 4.3 | 8.6 |
30–39 | 7.3 | 9.4 | 16.7 | 8.8 | 8.9 | 17.8 |
40–49 | 7.1 | 8.3 | 15.4 | 7.8 | 7.8 | 15.6 |
50–59 | 7.3 | 8.7 | 16.0 | 7.4 | 7.5 | 14.9 |
60–69 | 8.3 | 9.4 | 17.7 | 6.3 | 6.8 | 13.1 |
70–79 | 7.2 | 7.7 | 14.9 | 4.6 | 4.9 | 9.5 |
80+ | 2.2 | 2.6 | 4.8 | 1.8 | 2.5 | 4.3 |
14+ | 46.2 | 53.8 | 100 | 49.5 | 50.5 | 100 |
Notes
- Population estimates are based on ABS Estimated Resident Population data (ABS 2022b) and Population by Age and Sex data (ABS 2021).
- The 2022–2023 NDSHS sample was weighted to match Estimated Resident Population estimates.
Source: NDSHS 2022–2023, ABS 2021, ABS 2022, Table 12.2.
Response rates
Overall, contact was made with 49,389 in-scope households, from which 21,663 questionnaires were categorised as being complete and usable. This represented a response rate for the 2022–2023 survey of 43.9% (Table 3). This was the lowest rate of all survey waves conducted from 2010 and lower than the previous recorded low response rate for the 2004 survey (47.8%).
The response rate for the NDSHS was calculated using the total number of dwellings where contact was made as the number of eligible reporting units in the sample. If the entire eligible sample for the 2022–2023 NDSHS is used – that is, it includes all cases of non‑contact as part of the denominator (70,134 dwellings, plus 715 dwellings where the selected respondent was not available) – the response rate is reduced to 30.6%, meaning that over two-thirds of the sample did not receive, respond to, or return a completed, useable questionnaire. Again, this was the lowest rate among all surveys conducted from 2010.
Disposition | 2010 | 2013 | 2016 | 2019 | 2022–2023 |
|---|---|---|---|---|---|
Original sample | 81,708 | 75,992 | 70,935 | 69,741 | 72,382 |
Not residential | 1,786 | 1,506 | 1,080 | 908 | 704 |
Selected respondent not available | 604 | 789 | 784 | 648 | 715 |
Other ineligible | 175 | 711 | 550 | 489 | 829 |
Total out-of-scope households | 2,565 | 3,006 | 2,414 | 2,045 | 2,248 |
Eligible sample | 79,143 | 72,986 | 68,521 | 67,696 | 70,134 |
Less households not contacted | 26,453 | 24,407 | 22,034 | 22,215 | 20,745 |
Eligible sample contacted | 52,690 | 48,579 | 46,487 | 45,481 | 49,389 |
Refusals | 13,450 | 13,945 | 12,955 | 14,125 | 17,786 |
Foreign/no English | 979 | 1,063 | 760 | 644 | 383 |
Incapacitated | 370 | 341 | 237 | 220 | 178 |
Other non‑response | 325 | 258 | 797 | 833 | 973 |
Total eligible respondents who did not complete | 15,124 | 15,607 | 14,749 | 15,822 | 19,320 |
Less questionnaire not returned/unusable | 10,918 | 9,117 | 7,966 | 7,385 | 8,406 |
Total completes | 26,648 | 23,855 | 23,772 | 22,274 | 21,663 |
Response rate | 50.6 | 49.1 | 51.1 | 49.0 | 43.9 |
Source: NDSHS 2022–2023, Table 12.3.
Response rate differences by strata
Response rates tend to vary depending on the area that the households are located. This is important to consider when interpreting jurisdictional results. A lower response rate may increase non‑response bias, as a higher proportion of people opt out of completing the survey, and there may be differences between those people who refused to participate and the people who agreed to complete the survey.
In 2022–2023, the response rates varied from 33% in Sydney to 58% in Remainder Northern Territory. Response rates were the lowest recorded over the last five survey waves for Sydney (33%), Melbourne (40%), Brisbane (46%), Perth (41%), Remainder Western Australia (41%), Hobart (46%), Remainder Tasmania (55%), and Darwin (51%). See Table 4 for further results.
State | 2010 | 2013 | 2016 | 2019 | 2022–2023 |
|---|---|---|---|---|---|
NSW | 46 | 46 | 46 | 42 | 37 |
Vic | 48 | 47 | 49 | 48 | 41 |
Qld | 54 | 51 | 52 | 48 | 47 |
SA | 54 | 48 | 56 | 57 | 56 |
WA | 55 | 51 | 58 | 53 | 41 |
Tas | 61 | 61 | 62 | 60 | 50 |
NT(a) | 57 | 58 | 58 | 63 | 54 |
ACT | 59 | 57 | 59 | 53 | 55 |
(a) Data from the 8 remote communities interviewed in the Northern Territory in 2019 are excluded to maintain comparability over time.
Source: NDSHS 2022–2023, Table 12.4.
Non‑response bias and non‑sampling error
Survey estimates are subject to non‑sampling errors that can arise from errors in reporting of responses (for example, failure of respondents’ memories, incorrect completion of the survey form), the unwillingness of respondents to reveal their true responses, and non‑response.
The estimation methods used for the 2022–2023 results take into account non‑response and adjust for any underrepresentation of selected population subgroups in an effort to reduce non‑response bias.
A limitation of the survey is that the data are self-reported, and people may not accurately report information relating to illicit drug use and related behaviours because these activities may be illegal. This means that results relating to illicit drugs may be under-reported. For many illicit drugs, any biases are likely to be relatively consistent at the population level over time, so would not have much of an effect on trend analysis. Changes to legislation involving drugs may lead to an increase or decrease in self-reported drug use, not only because of changes in drug taking behaviours, but also due to changes in how likely people may be to report those behaviours. However, legislation protecting people’s privacy and the use of consistent methodology over time means that the impact of this issue on prevalence is expected to be limited.
Some behaviours may become less socially acceptable over time which may lead to an increase in socially desirable responses rather than accurate responses. Media reporting stigmatising a drug may lead to under-reporting of use of that drug (Chalmers et al. 2014). Any potential increase in self-reported socially desirable behaviours needs to be considered when interpreting survey results over time.
Sampling error
All proportions that are calculated from survey data are estimates rather than true population proportions. This means they have a margin of error due to only a sample of the population being surveyed. This is called sampling error.
There are different ways of measuring sampling error associated with an estimate from a sample survey. The 2022–2023 NDSHS uses both relative standard error and margin of error; these are included in the supplementary tables.
Relative standard error
The standard error (SE) is a measure of the dispersion of estimates calculated from all possible random samples from the same population. This can be estimated using the achieved single sample. The relative standard error (RSE) is the SE expressed as a percentage of the estimate and provides an indication of the size of the SE relative to the size of the estimate.
Results subject to an RSE of between 25% and 50% should be considered with caution and those with an RSE greater than 50% should be considered unreliable for most practical purposes. Estimates that have an RSE of between 25% and 50% are marked in the supplementary tables with *; those with an RSE between 50% and 90% are marked with ** and those with an RSE greater than 90% have not been published. Only estimates with an RSE of less than 25% are considered sufficiently reliable for most purposes.
Margin of error
The Margin of Error (MoE) describes the distance from the estimated value that the population value is likely to be within, at the 95% level of confidence. This means that the “true” proportion for the entire population would be within the margin of error around the reported estimate for 95% of possible samples.
Significance testing
When comparing two different estimates, it is important to determine whether the difference could reasonably be due to sampling error. This process is called ‘significance testing’. There are a number of variables that are used to calculate whether two estimates are significantly different – the size of the difference, the variability in the sample collected, which indicates the level of sampling error present, and the size of the sample. In this report, a difference is deemed to be statistically significant if the chance of seeing the observed difference under the null hypothesis was less than 5% (p <0.05).
All time-series tables, unless otherwise specified, have been tested for statistically significant changes between 2019 and 2022–2023, but not for other comparisons (such as differences between genders or between age groups). All increases or decreases described in the 2022–2023 NDSHS report are statistically significant at the 95% level of confidence (unless otherwise specified). If a difference is statistically significant, it has been marked with a ‘#’ symbol in the supplementary tables.
Sometimes, even large apparent differences may not be statistically significant. This is particularly the case for small populations because the small sample size means that there is not enough power to identify even large differences as statistically significant. Conversely, large samples can have the power to identify small differences as statistically significant.
Unless otherwise specified, changes between 2019 and 2022–2023 described in NDSHS reporting were found to be statistically significant (p <0.05).
Sample representativeness
No sample will ever be fully representative of the population, but if the sample is carefully designed and implemented, it will still be possible to draw conclusions about characteristics of the population. To assist in understanding the level of representativeness, the 2022–2023 sample was compared to the known benchmark of the 2021 Census (ABS, Census of Population and Housing, 2021, TableBuilder).
Comparison to the 2021 Census
A comparison between the 2021 Census and the weighted NDSHS sample indicates that:
- a higher proportion of employed people were captured in the sample, while a lower proportion of people not in the labour force were captured.
- people who completed Year 12 and those having certificate qualifications were over-represented in the sample; people with diploma qualification were under-represented.
- couple families were over-represented, while single person households and single parent households were under‑represented.
- married people were over-represented in the sample, while unmarried people were under-represented.
- people who did not speak English as their main language at home were under‑represented.
- people who lived in the most disadvantaged socio-economic areas were under-represented in the sample.
Comparison to 2019 sample
In comparison to the unweighted 2019 sample:
- Those currently employed showed a higher likelihood of responding to the 2022–2023 survey, while those engaged in studying or seeking employment were less likely to participate.
- People who finished year 12 or held bachelor or higher degree were more likely to participate in the 2022–2023 survey, while those whose highest level of school completion was year 11 or lower were less likely to take part.
- A lower proportion of people who lived in the most disadvantaged socioeconomic areas completed the survey in 2022–2023.
Efforts to improve response rates
Several other strategies were also used in 2022–2023 in an attempt to minimise cases of non‑contact and non‑response by the originally selected respondent.
Interim Placement Follow-up (IPF)
As in 2016 and 2019, the IPF was applied in 2022–2023 with adjustment from previous waves. When the selected respondent was unavailable at the time of placing the questionnaire, and the interviewer had placed the questionnaire with another member of the household, the interviewer attempted to contact the selected respondent again via a follow up phone call (or if in the neighbourhood, via a visit) to explain how to complete the questionnaire. The respondent could also elect to change the mode they intended to use to complete the survey.
If contact was only made with another household member during the initial call, a subsequent attempt was scheduled to reach the respondent. If arranging a time for contact was not possible, the questionnaire was treated as placed with another household member, and pick-up procedures followed the standard protocols implemented in 2016.
If the selected respondent refused to participate, the household was coded as a refusal. The interviewer then attempted to place an additional questionnaire in that area, to maintain the placement target for each SA1.
Advertising on social media in selected regions
In the 2022–2023 survey, advertising on social media in selected regions during the fieldwork period was employed to help increase awareness of the survey and potentially improve the response rate.
Awareness of the NDSHS did have a positive impact on acceptance and completion of the survey itself, however very few people who received the survey recalled seeing online advertisements for the survey.
QR code usage
As with the 2019 survey, a QR code was placed on paper questionnaire in 2022–2023 allowing respondents access to the online survey directly from the paper form. For respondents electing to complete online, the link to the survey was accessible immediately through accessing the general survey URL and entering the form number provided on the paper questionnaire, using the QR code provided on the paper questionnaire.
The inclusion of a QR code and online URL on the paper questionnaire may have influenced some paper respondents to switch to online completion after initially electing to complete the survey on paper.
Survey translation
For the first time, respondents had the option to complete the NDSHS online in a language other than English. The survey form was translated into Arabic, Mandarin/Simplified Chinese, Cantonese/Traditional Chinese, Greek, Italian and Vietnamese.
Other survey materials, including the approach letter, the Roy Morgan webpage and the Frequently Asked Questions (FAQ) section of the AIHW web page, were translated into the same languages, and indicated that the online survey could be completed in languages other than English.
Gated community approach strategy
In 2022–2023, a gated community approach strategy was implemented for households that have barriers that may prevent or limit access by interviewers, such as gated communities and apartment buildings where access is only available via a buzzer or intercom. A fortnight before commencing fieldwork, experienced interviewers visited SA1s where the starting address was identified as potentially being difficult to access, to ascertain whether access permission was necessary. If so, permission for access to interview was sought from the relevant parties (usually building managers) via a formal letter.
If access was granted, interviewing commenced as normal. If access was not granted, Roy Morgan assessed the SA1 to see if the survey could be distributed among other households, or if the SA1 would need to be replaced with a similar SA1 nearby.
Prize draw
In 2022–2023, as in 2019, an incentive was offered to all respondents to complete the survey. During the initial survey placement, respondents were informed that if they completed the survey, they would be eligible to enter 1 of 30 prize draws for a $500 EFTPOS card. Respondents could choose to opt out of the prize draw if they did not wish to participate.
Questionnaire changes in 2022–2023
The 2022–2023 questionnaire was modelled on the 2019 version, to maintain maximum comparability and preserve trend data. Some refinements were made to ensure that old questions remained relevant, and new questions could be implemented to address contemporary issues in the alcohol and other drug (AOD) sector. All changes to the questionnaire were tested through cognitive interviews.
This section describes the major changes made to the survey that are most likely to impact interpretations of results in the report or created changes to multiple supplementary tables. A full list of questionnaire changes in the 2022–2023 NDSHS is available on request.
Demographics
- Question 1 asking about respondent’s sex was replaced with two questions from Standard for Sex, Gender, Variations of Sex Characteristics and Sexual Orientation Variables(ABS 2020). These questions were renumbered to 1a and 1b accordingly. Question 1a asked about the participant’s sex recorded at birth. Question 1b asked how participants describe their gender.
Section A – Perceptions
- Revised questions A1 and A4:
- Adjusted examples for ‘Marijuana/Cannabis’, ‘Cocaine’, ‘Pain-killers/opioids’, and ‘Methadone/Buprenorphine’.
- Removed Steroids and added Hallucinogens, GHB, GBL or 1,4-BD, and Tranquilisers/sleeping pills as response codes.
- Added ‘Tranquilisers and sleeping pills’ and revised examples in questions A2 and A3.
- In question A5, changed header option from ‘Marijuana/Cannabis’ to ‘Marijuana/Cannabis for non‑medical use’.
- In questions A5, A6, and A7 rephrased header to emphasise ‘non‑medical use’ of marijuana/cannabis.
- Moved questions from individual drug sections to question A8 concerning opportunities over the past 12 months to use illicit substances.
Section B – General Health
- In Question B3, removed ‘Herbal and alternative medicines, vitamin and mineral supplements, etc.’ and added ‘Medical Marijuana/Cannabis’ to the response options.
Section C – Tobacco
- In 2019, Section D included questions on tobacco and electronic cigarette/vape use. In 2022–2023, Section D was amended to focus solely on electronic cigarettes/vapes use, and tobacco questions were moved to section C. All questions were labelled and renumbered accordingly.
- Added response option ‘Menthol cigarettes (manufactured or roll-your-own)’, and relabelled – ‘Water pipe with tobacco (e.g. shisha, hookah, nargillas)’ in question C14.
- Removed questions:
- D18. In the last 12 months, on average how much do you think you have cut down on your cigarette smoking?
- D24. Do you avoid places where you may be exposed to other people’s cigarette smoke?
- D38. During the last 12 months when you smoked unbranded tobacco (also called ‘chop chop’) was that...?
- Added ‘Heated (or heat-not-burn) tobacco products’ with a note indicating that these are not the same as e‑cigarettes/vapes to response option in question C23.
Section D – Electronic Cigarettes/Vapes
- Questions D26 to D30 from 2019 were relabelled as questions D1 to D5 in Section D in 2022–2023.
- New questions were added to Section D:
- Question D6. Thinking about the last time you used an electronic cigarette/vape, did it contain nicotine?
- Question D7. The last time you used an electronic cigarette/vape containing nicotine, was it obtained via a prescription?
- Question D8. During the last 12 months, did you find that you couldn’t stop or cut down on your use of electronic cigarettes/vapes, even though you wanted to or tried to?
- Question D9. During the past 30 days, on how many days did you use electronic cigarettes/vapes?
Section E – Alcohol
- Removed ‘Less often’ from response codes and added ‘Every few months’ and ‘Once or twice a year’ to response code in question E7.
- Included a new response code in question E10 (where do you usually obtain your alcohol?) ‘Purchase it myself to have it delivered to me (e.g. buy online, buy by phone)’.
- In question E11, revised response code from ‘Switched to drinking more low-alcoholic drinks than you used to’ to ‘Switched to drinking more low-alcohol drinks than you used to’; added response code ‘Switched to drinking more zero-alcohol beer/wine/spirits than you used to’.
- Added cider to the standard drinks chart.
- Moved question E23 to Section Z and relabelled as Z4a.
- Removed questions:
- E25 Has someone else been injured because of your drinking?
- E27 As far as you know, is the number of “standard drinks” shown on cans and bottles of alcoholic beverages?
- Added question E27 ‘Before today, did you know that Australia has alcohol guidelines that provide advice on how to reduce your health risks from drinking alcohol?’
- Added question E28. ‘Do you think your drink has ever been spiked (someone adding alcohol, a drug or other substance to your drink without your knowledge) with the intention of taking advantage of you in some way?’
Section F – Pain-killers/Pain-relievers and Opioids
- Updated definition of the term ‘non‑medical use/purposes’.
- Revised and updated response codes in question F4b:
- Included new response code ‘Tapentadol (e.g. Palexia)’.
- Changed response code from ‘Gabapentinoids (e.g. Lyrica)’ to ‘Gabapentin or Pregabalin (e.g. Lyrica, Neurontin)’.
- Changed response code from ‘Other prescription Pain-killers/Pain-relievers and Opioids’ to ‘Other (Please write in)’.
- Changed question F5 to read ‘During the last 12 months, did you find that you couldn’t stop or cut down on your use of Pain-killers/Pain-relievers and Opioids for non‑medical purposes even though you wanted to or tried to?’.
- Amended response codes in question F11:
- ‘Meth/amphetamine for non‑medical purposes’ changed to ‘Methamphetamine or Amphetamine’.
- ‘GHB’ changed to ‘GHB, GBL or 1,4-BD’.
- Changed the wording in question F12 to ‘During the last 3 months, has anyone expressed concern about your use of Pain-killers/Pain-relievers and Opioids for non‑medical purposes?’.
Section G – Tranquillisers/Sleeping pills
- Changed introduction paragraph: ‘This section asks about the use of Tranquillisers and Sleeping pills (e.g. Benzodiazepines, Sleepers, Diazepam, Tranks, Temazepam, Mogadon, Rivotril, Serapax, Xanax, Stilnox, Rohypnol, Hypnodorm, Valium, Alprax, Alprazolam).’
Section H – Pharmaceutical Stimulants
- This is a new section included in the 2022–2023 NDSHS questionnaire to understand non‑medical use of pharmaceutical stimulants.
- Question H1. Have you ever used any of the following pharmaceutical stimulants for non‑medical purposes?
- Question H2. Which of the following pharmaceutical stimulants have you used for non‑medical purposes in the past 12 months?
Section I – Steroids
- Adjusted steroids section from section H in 2019 to section I in 2022–2023.
- Removed questions H1, H3, H5-H8 about steroid consumption timeline and inability to stop using steroids for non‑medical purposes.
Section J – Kava
- This is a new section added in the 2022–2023 NDSHS questionnaire to understand how kava is accessed and people’s experiences of having kava in Australia.
- Six questions were added:
- Question J1 Have you ever had Kava in Australia?
- Question J2 Have you had Kava in Australia in the last 12 months?
- Question J3 In the last 12 months, how often did you have Kava in Australia?
- Question J4 In the last 12 months, what form of Kava did you have/use in Australia?
- Question J5 In the last 12 months, which of the following did you use at the same time, on at least one occasion that you had Kava in Australia?
- Question J6 In the last 12 months, where did you usually obtain Kava to have in Australia?
Section K – Methamphetamine and Amphetamine
- Section name was relabelled from ‘Meth/amphetamine’ to ‘Methamphetamine and Amphetamine’, and all questions were changed accordingly.
- Removed questions K1a, K1b and K1d.
- Removed response options ‘Doctor shopping/forged script’ and ‘Prescription for medical condition” from questions K8a and K8b.
- Removed question K10.
- For questions K11a to K11c, relabelled response options ‘Tablets/Pills’, and removed response option ‘Prescription amphetamine for non‑medical purposes’.
- Updated examples of drugs in response codes for question K13; relabelled to ‘GHB, GBL or 1,4-BD’ and ‘Pain-killers/Pain-relievers and Opioids for non‑medical use’.
Section L – Marijuana/Cannabis
- Removed questions L1a and L1b, renumbered L1c to L1 in 2022–2023.
- Replaced L10 with new question ‘What is the main form of Marijuana/Cannabis you have used in the last 12 months, the one you used most often?’
- Replaced L11 with new question ‘What other forms of Marijuana/Cannabis have you used in the last 12 months?’
- Removed L12 (2019), added new questions L12a ‘What is the main way you used Marijuana Cannabis in the last 12 months, the way that you used it most often?’ and L12b ‘What other ways have you used Marijuana/Cannabis in the last 12 months?’.
- Relabelled response options in L13 to ‘Methamphetamine or Amphetamine’, ‘GHB, GBL or 1,4-BD’, and ‘Pain-killers/Pain-relievers and Opioids for non‑medical use’.
Section O – Cocaine
- Removed questions O1a and O1b, renumbered question O1c in 2019 NDSHS as O1 in 2022–2023.
- Removed question O10.
- Relabelled response options for question O13 to ‘Methamphetamine or Amphetamine’, ‘GHB, GBL or 1,4-BD’, and ‘Pain-killers/Pain-relievers and Opioids for non‑medical use’.
Section Q – Ecstasy
- Removed questions Q1a and Q1b, renumbered question Q1c in 2019 as question Q1 in 2022–2023.
- Removed question Q11 in 2019.
- Relabelled response options in question Q11 to ’Methamphetamine or Amphetamine’, ‘GHB, GBL or 1,4-BD’, and ‘Pain-killers/Pain-relievers and Opioids for non‑medical use’.
Section S – GHB, GBL and 1,4-BD
- Updated section title and all relevant questions from ‘GHB’ to ‘GHB, GBL and 1,4-BD’.
- Added question S7: Which of the following have you used in the last 12 months?
Section V – Injectable Drugs
- Updated examples of drugs in response codes for questions V3 and V4; relabelled to ‘GHB, GBL or 1,4-BD’ and ‘Pain-killers/Pain-relievers and Opioids for non‑medical use’.
Section W – Experiences Using Illicit Drugs
- Revised question W1:
- Changed question text ‘Name all the factors that influenced your decision to first use an illicit drug (including Marijuana/Cannabis for non‑medical purposes)’.
- Added response option ‘Celebrities/Social influencers were using it’.
- Added response option ‘Influence of celebrities/social influencers’ to questions W2a and W2b.
- Removed response option "None of the above" and added “Yes” or “No” response options for each item (activities undertaken under the influence of drugs) to question W3.
Section X – Attitudes
- Relabelled response options for question X1 to ‘Methamphetamine or Amphetamine’, and ‘GHB, GBL or 1,4-BD’.
- Changed question text for question X2 ‘What factors influenced your decision never to try illicit drugs?’
Section Z – Lifestyle
- Changed question text for question Z1 ‘In the last 3 months, how many days of work did you miss because of any illness or injury?’ and revised response code from ‘Not applicable (don’t work or study)’ to ‘Not applicable (don’t work)’.
- Changed question text for questions Z2 and Z3 to exclude study (school, TAFE or university) missed as a result of illness/injury, alcohol or illegal drug consumption.
- Moved question E23 from alcohol section in 2019 NDSHS to section Z and relabelled as Z4a in 2022–2023.
- Removed response option ‘None of the above’ from question Z4a, added response option ‘I did not drink alcohol in the last 12 months’, and reformatted to ‘Yes/No’ responses for each item (activities undertaken under the influence of alcohol).
- Added question Z4b ‘Are you or your partner currently planning a pregnancy and actively trying to conceive?’
- Added question Z7a ‘In the last 12 months when you were pregnant or breastfeeding, did anyone give you advice related to alcohol consumption?’
- Added question Z7b ‘Who gave you advice related to alcohol when you were pregnant or breastfeeding?’
- Removed questions Z9, Z9c, Z10, Z11and Z12 from the 2019 questionnaire.
Section YY (Policy Support)
- Changed question YY1:
- Removed response code ‘Support for regulation of alcohol supply to minors on private premises’.
- Added response codes ‘Pricing controls to prevent the sale of very cheap alcohol at bottle shops (e.g. alcohol cannot be sold for less than $1.5 per standard drink)’, ‘Restrictions on where zero-alcohol products with an alcohol brand can be displayed and sold in stores’ and ‘Limiting alcohol advertising online and on social media’.
- Revised question YY2:
- Deleted response options ‘Stricter enforcement of the law against supplying cigarettes to customers who are under age’, ‘Stricter penalties for the sale or supply of tobacco products to those under 18 years of age’, ‘Restrictions on where and when electronic cigarettes can be advertised’, ‘Restricting the use of electronic cigarettes in public places (similar to the current restrictions for cigarettes)’, and ‘Prohibiting the sale of electronic cigarettes to people under 18 years of age’.
- Rephrased response option ‘Banning all additives (e.g. flavouring) in cigarettes to make them less attractive to young people’.
- Added options ‘Banning the advertising of tobacco products on social media (e.g. Facebook, Instagram)’, and ‘Banning the sale of tobacco products in places where people are consuming alcohol’.
- Added question YY2a ‘Thinking now about the problems associated with electronic cigarette/vape use, to what extent would you support or oppose measures such as…’:
- Banning all additives (e.g. flavouring) in electronic cigarettes/vapes, to make them less attractive to young people.
- Restricting the use of electronic cigarettes/vapes in public places (similar to the current restrictions for cigarettes).
- Prohibiting the sale of electronic cigarettes/vapes, including those without nicotine, to people under 18 years of age.
- Strengthening restrictions on the advertising and promotion of electronic cigarettes/vapes.
- Relabelled response option for questions YY4 and YY5 to ‘Methamphetamine or amphetamine’.
- Relabelled response option for question YY6 to ‘Allowing people to test their pills/drugs at designated sites. The test will inform them of the purity and the substances the drug contains’.
- Removed question YY9 in 2019.
Section ZZ – Demographics
- Added question ZZ3a ‘Which language did you first speak as a child?’
- Added question ZZ3b ‘Do you consider you speak English very well, well, or not well?’
- Reworded ZZ4 ‘How do you describe your sexual orientation?’
- Added question ZZ6a ‘How many hours per week do you usually work at your current main job (i.e., the job you worked the most hours in)?’
- Added question ZZ6b ‘How many hours per week do you usually work across all of your current jobs?’
- Added question ZZ8a ‘Have you ever served in the Australian Defence Force, either in Regular Service or Reserves?’
Analysis changes and updates in 2022–2023
Sex and gender analysis
In the 2022–2023 NDSHS survey, two questions from the Standard for Sex, Gender, Variations of Sex Characteristics and Sexual Orientation Variables (ABS 2020) were included in the opening demographics section. The question about the participant’s sex recorded at birth, and another about how they describe their gender, were used to replace the question from previous survey waves asking about the participant’s sex at the time of the survey.
These questions were incorporated to ensure that respondents would be able to respond to the survey accurately and feel represented. Their inclusion also allows for results to be presented for cisgender and trans and gender diverse populations.
This represents a substantial change to a key variable in the NDSHS, as the previously included question (‘what is your sex’) was used for many disaggregations in 2019 and earlier survey years. The 2022–2023 NDSHS results are instead disaggregated by gender. In tables that disaggregate results by gender, results for 2019 and earlier years are disaggregated by the previous ‘What is your sex’ question. Caution is advised when considering timeseries comparisons.
Results for cisgender and trans and gender diverse people
The ‘two-step method’ outlined in the Standard for Sex, Gender, Variations of Sex Characteristics and Sexual Orientation Variables (ABS 2020) to derive the cisgender and trans and gender diverse classification was used to generate 2022–2023 NDSHS results. This classification was based on Questions 1a and 1b.
Impact of split fieldwork periods on drug use statistics
The 2022–2023 NDSHS fieldwork was conducted in two stages, the first from 20 July to 18 December 2022, and the second from 20 March to 31 May 2023. This represents a change from previous NDSHS waves and needs to be assessed for changes to the data.
A binomial logistic regression was run on all ‘recent use of drugs’ results, similar to the method used to assess mode effects. This method takes other variables (most notably strata) into account, to ensure that any differences between 2022 and 2023 were not due to other factors, such as the different areas being surveyed in each year.
The results (Figure 1) show that people responding in 2023 were slightly more likely to report use of most drugs, but the only substantial changes occurred for recent use of methamphetamine and amphetamine, and ecstasy. This indicates that most drug types are comparable across fieldwork periods.
Figure 1: Odds ratios for smoking, drinking, and recent(a) use of drugs in 2023 compared to 2022
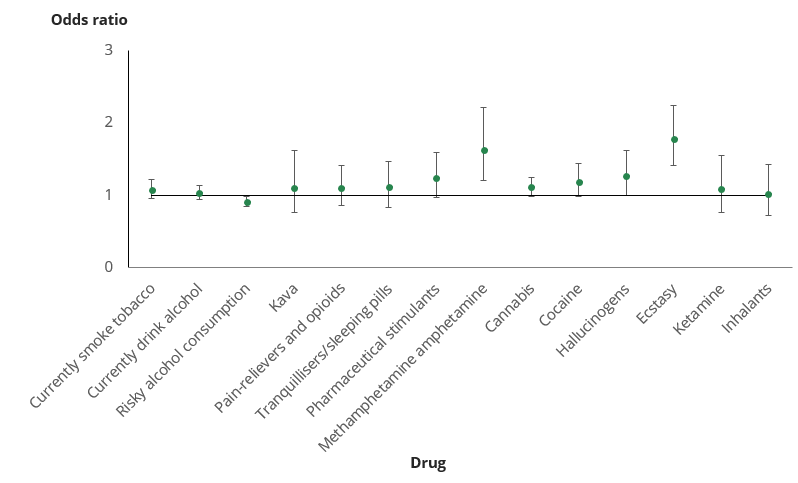
(a) Used in the previous 12 months.
Note: Error bars represent a 95% confidence interval.
Source: AIHW analysis of NDSHS 2022–2023.
Further analysis showed the differences between methamphetamine and amphetamine data collected in 2022 and 2023 may be caused by seasonality effects. As a comparison, results were run for 2019, comparing data collected in April and May to data collected in August and September (Table 5). Methamphetamine and amphetamine and Ecstasy use showed a significant impact of fieldwork period. Cannabis and Cocaine did not, and are shown for comparison.
Drug use | Apr–May 2019 | Aug–Sep 2019 | July–Dec 2022 | Mar–May 2023 |
|---|---|---|---|---|
Ecstasy in past 12 months | 2.8% | 3.1% | 1.7% | 2.7% |
Ecstasy in past month | 1.0% | 1.2% | 0.5% | 1.1% |
Methamphetamine in past 12 months | 1.6% | 1.1% | 0.9% | 1.2% |
Methamphetamine in past month | 0.6% | 0.5% | 0.4% | 0.5% |
Cannabis in past 12 months | 10.5% | 12.6% | 11.1% | 12.1% |
Cannabis in past month | 6.3% | 7.2% | 6.6% | 6.9% |
Cocaine in past 12 months | 4.1% | 4.6% | 4.2% | 5.0% |
Cocaine in past month | 1.4% | 1.6% | 1.5% | 1.8% |
Source: AIHW analysis of NDSHS 2022–2023.
These results give some indication that the differences in use of methamphetamine and amphetamine are to be expected from the general seasonality of the data. The difference between 2022 and 2023 was 0.3 percentage points, lower than the difference between April–May 2019 and August–September 2019 (0.5 percentage points). Positively, the ‘use in the last month’ question remained stable between fieldwork periods, showing that restarting fieldwork in March of 2023 likely left a large enough interval for any deviation in drug use associated with the holiday period to settle down.
Ecstasy showed a more prominent difference between 2022 and 2023, for both use in the last 12 months and use in the last month. It is possible that this is a real difference at the national level, as opportunities to use ecstasy in mid-to-late 2022 (for example, events) were still limited by the impacts of health restrictions implemented in response to the COVID-19 pandemic. This is explored further in the ecstasy web article.
Reporting of methamphetamine and amphetamine, and ecstasy
AIHW recommends the following:
- Drug use statistics for all major drug types, including methamphetamine and amphetamine, should combine data from the entire survey fieldwork period (that is, both 2022 and 2023 results should be included in key findings).
- In key findings and general reporting, use of ecstasy should incorporate data from both 2022 and 2023, with a footnote indicating that it is aggregated over two periods with different levels of use.
Measuring risky alcohol consumption
In 2021, the AIHW published a technical paper providing a methodology for measuring risky alcohol consumption according to the Australian Guidelines to Reduce Health Risks from Drinking Alcohol (NHMRC, 2020). Full details of the methodology can be found online.
The estimation of risky drinking in 2022–2023 was based on Guideline 1, which comprises two specific recommendations that applied to NDSHS data:
Any person who, in the past 12 months:
- Consumed no more than 10 standard drinks per week on average; and
- Never consumed more than 4 standard drinks on a single day (or did so less often than once per month on average)
is classified as having consumed alcohol in ways that reduced their risk of experiencing alcohol-related disease or injury.
In contrast, people who reported drinking more than 10 standard drinks per week or who drank more than 4 standard drinks on a single day at least once a month on average are classified as having consumed alcohol in ways that increased their risk of harm.
Data on alcohol consumption from the NDSHS between 2001 and 2019 were also re-analysed according to the 2020 alcohol guidelines, so that results from 2022–2023 could be compared to previous surveys (even if different alcohol advice was available at the time).
Terminology
Unbranded and illicit branded tobacco
Illicit tobacco includes both unbranded tobacco and branded tobacco products on which no excise, customs duty or GST was paid. Unbranded tobacco (commonly known as chop-chop) is finely cut, unprocessed loose tobacco that has been grown, distributed, and sold without government intervention or taxation (ANAO 2002).
Illicit branded tobacco products include overseas-produced cigarettes (or packets of smoking tobacco) designed to comply with packaging laws in countries other than Australia, but which make their way into Australia, without payment of customs duty, for sale to consumers in Australia.
Electronic cigarettes
Electronic cigarettes (also known as e‑cigarettes, e‑cigs, electronic nicotine delivery systems, electronic non‑nicotine delivery systems, alternative nicotine delivery systems, personal vaporisers, e-hookahs, vape pens or vapes) are devices designed to deliver nicotine and/or other chemicals via an aerosol vapour that the user inhales (Greenhalgh & Scollo 2018). E‑cigarettes contain a battery, which is used to heat a liquid to deliver an aerosol that is inhaled (Department of Health and Aged Care 2023).
The 2022–2023 NDSHS used the definition for electronic cigarettes included in the 2019 survey with minor revisions. All questions relating to electronic cigarette use were changed in reference to this definition.
Electronic cigarettes/e‑cigarettes or vapes are personal vaping devices where users inhale vapour rather than smoke. The inhaled vapour usually contains flavourings and may contain nicotine as well.
This definition is broad enough to capture the use of most vaporising devices but does not include heated tobacco products (sometimes referred to as heat-not-burn products).
Alcohol risk
The alcohol risk data presented in the 2022–2023 report and supplementary tables are reported against The Australian guidelines to reduce health risks from drinking alcohol released by the National Health and Medical Research Council (NHMRC 2020). Results referencing ’risky drinking’ or ‘risky alcohol consumption’ report against Guideline 1. See Box 1 for further details.
Box TI.1: The 2020 Australian guidelines to reduce health risks from drinking alcohol
In summary, there are 3 guidelines:
- Guideline 1: To reduce the risk of harm from alcohol-related disease or injury, healthy men and women should drink no more than 10 standard drinks a week and no more 4 standard drinks on any one day. The less you drink, the lower your risk of harm from alcohol.
- Guideline 2: To reduce the risk of injury and other harms to health, children and people under 18 years of age should not drink alcohol.
- Guideline 3: To prevent harm from alcohol to their unborn child, women who are pregnant or planning a pregnancy should not drink alcohol. For women who are breastfeeding, not drinking alcohol is safest for their baby.
Illicit use of drugs
In the 2022–2023 survey, as in the past, respondents were asked about their use of some drugs that have legitimate medical uses. These include pharmaceuticals (pain-killers/pain-relievers and opioids, tranquillisers/sleeping pills, steroids, pharmaceutical stimulants and methadone/buprenorphine), as well as medical use of cannabis. The focus of the survey and corresponding data are on the use of these drugs for non‑medical purposes.
The term ‘illicit drugs’ in this report includes the following: illegal drugs (such as cocaine), pharmaceutical drugs (such as pain-relievers and opioids) when used for non‑medical purposes (strictly an illicit behaviour), and other substances used inappropriately such as inhalants (see Box TI.2 for further details). Note that where each of these licit/illicit drugs is central to the analysis, it is their illicit use that is analysed.
Box TI.2: Definition of illicit use of drugs
‘Illicit use of a drug’ can encompass a number of broad categories including:
- Illegal drugs – drugs that are prohibited from manufacture, sale or possession in Australia – for example, ecstasy, cocaine, heroin and amphetamine type stimulants.
- Pharmaceuticals – drugs that are available from a pharmacy, over the counter or by prescription, which may be subject to non‑medical use – for example, opioid-based pain relief medications, opioid substitution therapies, benzodiazepines, and steroids.
- Other psychoactive substances, legal or illegal, that can potentially be used in a harmful way – for example, synthetic cannabis and other synthetic drugs, or inhalants such as petrol, paint or glue (MCDS 2011).
Medical use and recent use of cannabis
Prior to 2016, Australian law generally considered cannabis to be an illegal narcotic. However, in February 2016, the Narcotics Drug Act 1967 was amended, and medicinal cannabis products were made available for specific patient groups under strict medical supervision. For the purposes of the NDSHS, marijuana/cannabis is not considered a pharmaceutical, and is not grouped with non‑medical use of other drugs such as opioids and steroids. In order to analyse illicit marijuana/cannabis use, two new questions were included regarding medical use of cannabis in 2019:
- Have you used Marijuana/Cannabis for medical purposes in the last 12 months?
- Was the medical Marijuana/Cannabis prescribed by a doctor?
People that reported only using marijuana/cannabis for medical purposes in the previous 12 months, and only using it when it was prescribed by a doctor, are not included in “recent use of cannabis” results. They are however still included in lifetime use results, as the questions regarding medical use of cannabis only refer to the previous 12 months. All other respondents that indicated using marijuana/cannabis for any reason in the previous 12 months are included in recent use results.
ASSIST-Lite
The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) was developed by the World Health Organisation (WHO) to identify people whose substance use may be causing them harm. The ASSIST screens for harmful use of alcohol and tobacco, as well as illicit drugs and pharmaceuticals.
ASSIST scores are categorised as ‘low risk’, ‘moderate risk’ or ‘high risk’. High risk scores are likely to indicate a substance dependence issue, while moderate risk scores indicate substance use that may be hazardous or harmful to the person’s health.
The ASSIST-Lite is an abridged version of the ASSIST, consisting of 3 to 4 questions for each substance. It was incorporated into the NDSHS in 2019 to estimate how many people may show signs of substance dependence, or a pattern of use that may be hazardous to their health. Results also have implications for alcohol and other drug treatment services in Australia: people that receive a high risk score are likely to require specialist assessment and treatment for their substance use, while people that receive a moderate risk score are likely to benefit from a brief intervention or education of some kind.
It is worth noting that the questions included in the NDSHS are not exactly the same as the questions in the ASSIST-Lite (see Ali et al. 2013 for further information on the ASSIST-Lite). However, all differences were confirmed with the authors of the ASSIST-Lite, to ensure the questions in the NDSHS were comparable. Existing questions were used where it was agreed that they were equivalent, and some were altered to include equivalent response options.
Update to ASSIST-Lite scoring thresholds for risky cannabis use
Choosing cut-off points for moderate and high-risk scores in the ASSIST-Lite requires consideration of the impacts they may have in clinical settings. If they are set too low, the tool will give false positives, classifying people as moderate or high risk when their use is not risky. However, if they are set too high, they risk missing some people whose substance use may be harmful to their health.
Previous evidence indicated that the cannabis scoring in the ASSIST, and as a result the ASSIST-Lite, was classifying many people as moderate risk when their use of cannabis was not risky (Davis et al. 2009). This is partially due to the increase in the prevalence of medical cannabis, which may be used frequently without causing harm to the person using it. The ASSIST-Lite is being updated to increase the threshold for moderate risk from a score of 1 to a score of 2, while a score of 3 remains high risk (R Ali 2020, pers. comm., 18 May 2020).
As in 2019, cannabis results published in the 2022–2023 NDSHS report and supplementary tables use this changed threshold and may not be comparable to other ASSIST or ASSIST-Lite results published elsewhere.
Emerging psychoactive substances
Emerging psychoactive substances (EPS), or new psychoactive substances, include substances not controlled by the 1961 Convention on Narcotic Drugs or the 1971 Convention of Psychotropic Substances, or substances that are relatively new to the recreational drug market and have mind-altering effects. EPS often mimic the effects of existing illicit psychoactive drugs such as cannabis, ecstasy (MDMA) and LSD, or have a chemical structure very similar to existing illicit substances. Other names given to this group of drugs include: research chemicals, analogues, or bath salts.
This section has been changed to ‘Other synthetic drugs’ since 2019. Examples were updated in the 2022–2023 NDSHS, with the introductory text reading ‘Other synthetic drugs, also known as Emerging Psychoactive Substances, are drugs that often mimic the effects of more established illegal drugs. These are sometimes referred to as research chemicals, analogues, or bath salts. Some of the more well-known substances include Mephedrone, NBOMe, Methylone, Flakka, MDPV, 2C-I, BZP, Etizolam, Carfentanyl, Acetylfentanyl and other synthetic forms of fentanyl.
Presentation of estimates
Proportions are shown as percentages rounded to 1 decimal place when less than 20% and rounded to a whole number when over 20%. All data presented in the body of the report are unadjusted estimates of proportions and have not been age-standardised unless indicated.
Means and Medians
In some cases, estimates are presented as medians as well as means. This has been done for tables when there was a concern that the means may be skewed by outliers. For example, when considering the average number of cigarettes that people smoke per week, a vast majority of people report numbers between 0 and 100. However, a small number of people do report numbers much greater than 100.
As the mean is a summary of all of the data points, it will be distorted by very large outliers. In contrast, the median is simply a description of the mid-point of all of the data. Half of the responses will be below the median, and half will be above. As a result, the median is not affected greatly by a small number of outliers.
Throughout the report, medians are only used in cases where the mean was noticeably affected by outliers or a skewed distribution. All means and medians in the report have been indicated.
Population estimates
Population estimates are calculated by applying survey prevalence rates to the relevant population count and were based on the June 2023 ABS estimated resident population. Population estimates are shown to the nearest 100,000 or 10,000, depending on the size of the estimate.
Household estimates
Household estimates are similarly calculated by applying survey prevalence rates to the relevant household counts, which are calculated from household and family projections, 2016–2041 (ABS 2019). Series II projections are used, assuming a linear increase from June 2022 to June 2023 to estimate the projected number of households in September 2022. Additionally, only estimates from the geographical strata are used, so other territories are excluded. This method matches the number of households used in the sample weighting. Household estimates are shown to the nearest 100,000 or 10,000, depending on the size of the estimate.
Age standardisation
The age profile of Australians varies across jurisdictions, other geographic classifications, such as remoteness areas, periods of time and/or population subgroups (for example, between First Nations and non‑Indigenous populations). Age-standardisation is a process that accounts for the differences in the age compositions of 2 or more populations, to allow comparisons between these populations having adjusted for differences in their age structures.
Age-standardisation is important in this publication, as drug-related behaviours can be age related. Age-standardisation accounts for this by allowing comparisons between groups having adjusted for their differing age profiles. A standard age composition is used against which subpopulations are standardised, in this case the age composition of the 30 June 2001 Australian estimated resident population.
Age-standardisation was applied to some social characteristics data, but only where differing age profiles were shown to have a meaningful impact on the comparisons between population groups. It was not applied to the majority of data presented in the report or the supplementary data tables. Age-standardisation was undertaken using the direct method.
Access to the CURF
A public-use Confidentialised Unit Record File (CURF) will be available to researchers through the Australian Data Archive (ADA) at the Australian National University, from May 2024.
Some transformations will be made to the public-use CURF to protect respondent confidentiality. For a full list of transformations, please check the CURF supplementary material on the ADA website from May 2024.
Applications for research access to the master data set, which contains all the data items, or selected variables of interest not included in the CURF, may be approved, subject to the agreement of the AIHW’s Ethics Committee. Contact the Tobacco, Alcohol and Other Drugs unit by email at [email protected] for additional information.