Australia's mothers and babies:
Maternal deaths
Web article
Last updated:
Topic: Mothers & babies
Part of Australia's mothers and babies
Citation
AIHW (Australian Institute of Health and Welfare) (2025) Maternal deaths, AIHW, Australian Government, accessed 26 July 2026.
Latest edition
Content warning: This page contains information some readers may find distressing as it relates to maternal deaths, suicide and self-harm, alcohol and drug use, and pregnancy loss.
Maternal deaths in Australia
In Australia, where childbirth is safe for most women, maternal death is rare. In 2023, 27 women were reported to have died during pregnancy or within 42 days of the end of pregnancy. Of these, 23 were classified as directly or indirectly related to the pregnancy, 3 were coincidental and one death has not yet been classified (definitions for these terms are provided below).
Data about the deaths that were directly or indirectly related to pregnancy are the focus of this report.
In 2023:
- The maternal mortality ratio (MMR) in Australia was 8.2 deaths per 100,000 women giving birth (23 maternal deaths). Australia’s MMR trend (since the early 1970s) is presented in Maternal mortality over time.
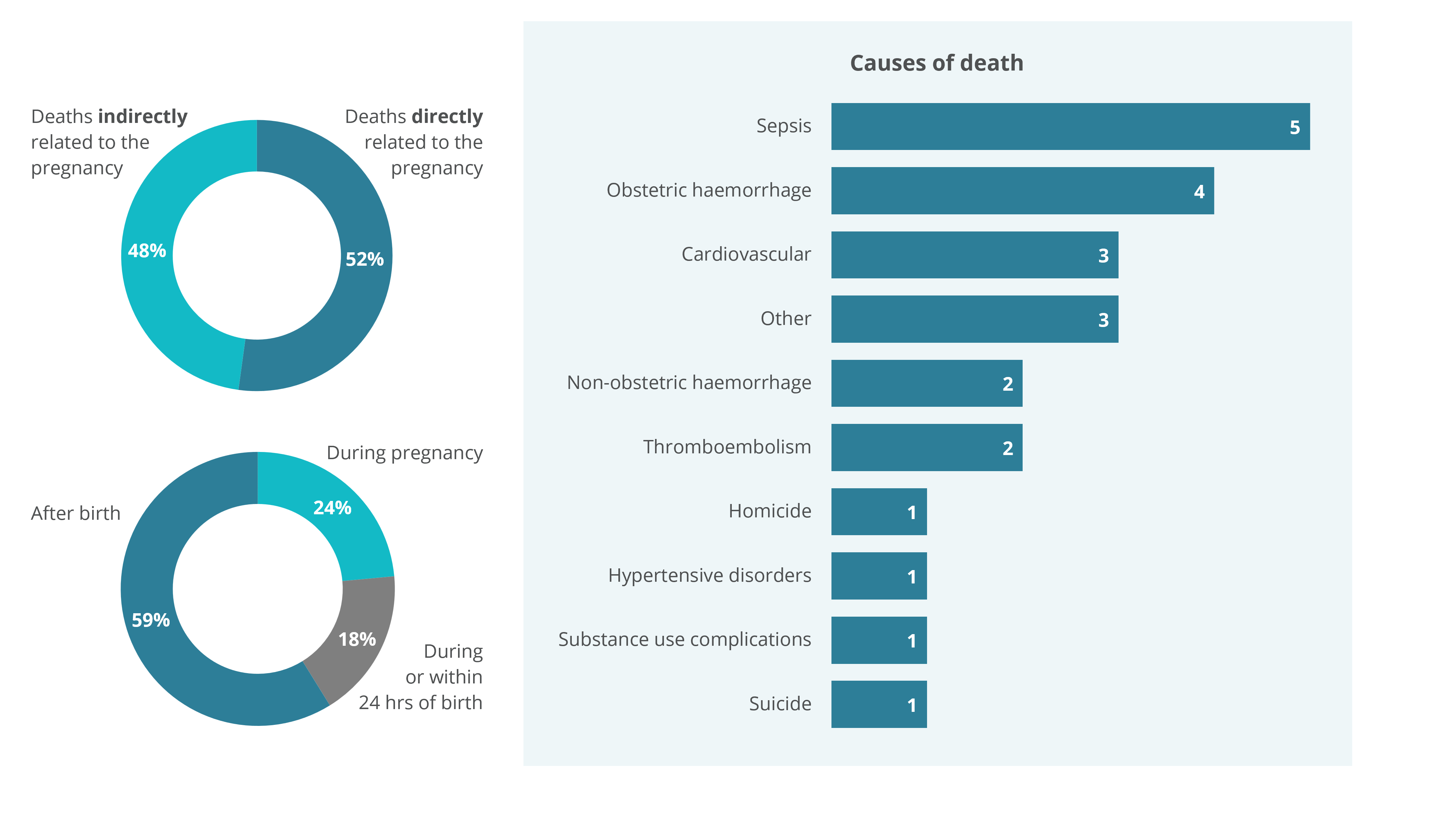
- Of the 23 maternal deaths, 52% were directly related to pregnancy, while 48% were indirectly related (Figure 1).
- Nearly two thirds (59%) of maternal deaths occurred after birth, while 18% occurred during or within 24 hours of birth, and 24% occurred during pregnancy (Figure 1).
Figure 1: Maternal deaths in Australia, 2023
1. One death from 2023 has not yet been classified as either a maternal death or coincidental and is therefore not included in this report. The classification will be updated once the jurisdictional maternal mortality review committee has reviewed the death.
2. Data may not add to the total due to rounding.
Source: AIHW analysis of the National Maternal Mortality Data Collection.
Definitions
All deaths that occur during pregnancy or within 42 days of the end of a pregnancy are reviewed by health professionals to determine the likely cause and whether the pregnancy contributed to the death. Following review, deaths are classified as maternal (direct, indirect or not further classified) coincidental, or unclassified.
Maternal deaths
Maternal death is the death of a woman while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and outcome of the pregnancy, from any cause related to or aggravated by the pregnancy or the associated care received but not from accidental or incidental causes. Maternal deaths are divided into 2 categories:
- Direct maternal deaths are those resulting from complications of pregnancy or birth and/or the associated clinical care; and
- Indirect maternal deaths are those resulting from diseases or conditions that were not due to a direct obstetric cause, but were aggravated by the pregnancy or birth.
Coincidental deaths
Coincidental deaths are defined as those that are reported to have occurred during pregnancy or within 42 days of the end of pregnancy, but are considered to be causally unrelated to pregnancy. Unlike direct and indirect maternal deaths, coincidental deaths are excluded from analysis and maternal mortality ratio (MMR) calculations.
There were 45 coincidental deaths in Australia from 2014–2023. The most common causes of these deaths were motor vehicle trauma and cancer. Although not the focus of this report, some additional data on these deaths, such as causes, can be found in Tables 1 & 2 of the supplementary tables (Data tables: National Maternal Mortality Data Collection annual update 2023).
Maternal mortality ratio
The incidence of maternal death is expressed as the maternal mortality ratio (MMR). The MMR is calculated using direct, indirect and not classified maternal deaths and expressed as per 100,000 women giving birth. Coincidental deaths and deaths awaiting classification are not included in MMR calculations.
Maternal mortality over time
Due to the small number of maternal deaths that occur in a year, small variations in the number can lead to large fluctuations in the MMR making it difficult to interpret the trend in maternal mortality over time using single year rates. Using a ‘triennia’ approach (aggregating three years of data) can assist. Over the past 50 years, the rate has fluctuated at times but overall Australia’s MMR has significantly declined from 12.7 per 100,000 women giving birth in 1973–1975, to 6.7 in 2021–2023.
Prior to the most recent period, the rate of maternal death had decreased in each of the preceding 4 triennia, from 7.7 in 2009–2011 to 6.3 in 2018–2020. However, this triennium (2021–2023) shows an increase in the MMR, to 6.7 per 100,000 women giving birth. The MMR will be monitored as more data are available.
Internationally, Australia has one of the lowest MMRs. Compared with other countries that are signatories to the United Nations’ Sustainable Development Goals (SDGs), Australia and New Zealand had the lowest MMR across the SDG regions in 2023 (WHO, 2025). For more information on Australia’s MMR in an international context see: Maternal Deaths in Australia 2018–2020.
Data on maternal mortality ratios over time can be explored in the interactive data visualisation below, with data also presented in Table 1 of the supplementary data tables (Data tables: National Maternal Mortality Data Collection annual update 2023).
Figure 3: Number of maternal deaths, by cause of death, 2014–2023
For the period 2014 to 2023 cardiovascular disease was the leading cause of maternal death, with 27 deaths.

Figure 4: Number of maternal deaths, by timing of death, 2014–2023
For the period 2014 to 2023, 73 deaths occurred after birth

Figure 5: Maternal mortality ratio of women who gave birth, by selected maternal characteristic, 2014–2023
For the period 2014 to 2023, the maternal mortality ratio for women aged under 20 was 19.2 per 100,000 women giving birth.
