Medicare-subsidised palliative medicine attendance and case conference services
Figure 1.1: This interactive data visualisation shows the number and rate (per 100,000 population) of people receiving MBS-subsidised palliative medicine attendance and/or case conference services provided by palliative medicine physicians/specialists by sex in 2021–22. The number and rate (per 100,000 population) of males receiving these services were slightly higher than females.
Figure 1.2: This interactive data visualisation shows the age distribution of people receiving MBS-subsidised palliative medicine attendance and/or case conference services provided by palliative medicine physicians/specialists, both the number and rate (per 100,000 population) in 2021–22. The number of people receiving these services increased with age to age 75–84 and then declined for those aged 85 and over. The age-specific rate (per 100,000 population) of people receiving these services also increased steeply with age, with the highest rate for those aged 85 and over.
Figure 1.3: This interactive data visualisation shows the number and rate (per 100,000 population) of people receiving MBS-subsidised palliative medicine attendance and/or case conference services provided by palliative medicine physicians/specialists by remoteness areas of usual residence in 2021–22. Major Cities had the highest number and rate (per 100,000 population) of people receiving these services.
Figure 1.4: This interactive data visualisation shows the number and rate (per 100,000 population) of people receiving MBS-subsidised palliative medicine attendance and/or case conference services provided by palliative medicine physicians/specialists by states and territories in 2021–22. New South Wales had the highest number of people receiving these services, while Northern Territory had the lowest. Queensland had the highest rate of people (per 100,000 population) receiving these services while Australian Capital Territory had the lowest.

Figure 2.1: This interactive data visualisation shows the number, rate (per 100,000 population) and services per person of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists, by sex in 2021–22. The number and rate (per 100,000 population) of these services for males were slightly higher than females. While the services per person was slightly higher in females compared to males.
Figure 2.2: This interactive data visualisation shows the age distribution of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists, including number, rate (per 100,000 population) and services per person in 2021–22. The number of these services increased with age to age 75–84 and then declined for those aged 85 and over. The age-specific rate (per 100,000 population) of these services also increased steeply with age, with the highest rate of services for those aged 85 and over. The highest number of services per person was for age 55-64 years.
Figure 2.3: This interactive data visualisation shows the number and proportion of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists by MBS item groups in 2021–22. Attendance in a consulting room or hospital was the most common MBS item for palliative medicine attendances, while organising and coordinating a discharge case conference was the most common MBS item for palliative medicine case conferences.
Figure 2.4: This interactive data visualisation shows the number, rate (per 100,000 population) and services per person of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists, by service group and remoteness areas of usual residence in 2021–22. Major cities had the highest number and rate (per 100,000 population) of palliative medicine attendances and case conferences, followed by Inner regional areas. Major cities had the highest services per person for the palliative medicine attendances and Outer regional areas had the highest services per person for the palliative medicine case conferences.
Figure 2.5: This interactive data visualisation shows the number, rate (per 100,000 population) and services per person of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists, by service group and states and territories in 2021–22. Queensland had the highest number of services for palliative medicine attendances and New South Wales had the highest number of services for palliative medicine case conferences. Western Australia had the highest rate (per 100,000 population) of services for palliative medicine attendances and Queensland had the highest rate (per 100,000 population) of services for palliative medicine case conferences. Western Australia had the highest number of services per person for palliative medicine attendances and case conferences.

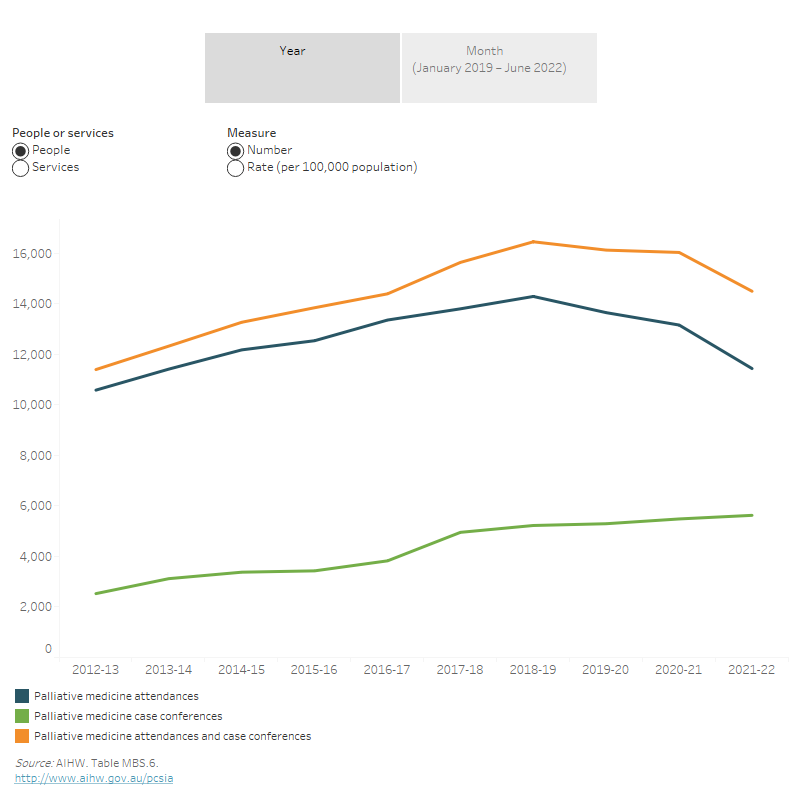
Figure 3.1: This interactive data visualisation shows the number and rate (per 100,000 population) of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists and people receiving them by service group each year between 2012–13 and 2021–22. It showed that the number and rate (per 100,000 population) of palliative medicine attendances and people receiving them increased between 2012–13 and 2018–19 and then declined to 2020–21 and 2021–22. However, palliative medicine case conferences and people receiving them gradually increased between 2012–13 and 2021–22.
Figure 3.2: This interactive data visualisation shows the number and rate (per 100,000 population) of MBS-subsidised palliative medicine attendance and case conference services provided by palliative medicine physicians/specialists and people receiving them by service group each month from January 2019 to June 2022. It showed that the number of palliative medicine attendances and case conferences and people receiving them had the largest drop between March and April 2020 and a second largest drop in January and April 2022. While the number of palliative medicine attendances and case conferences and people receiving them increased between April 2020 and March 2021.