Medication dispensing
On this page:
Key points
- The majority of ADF members (81%) who died by suicide between 2013 and 2018 were dispensed at least one Pharmaceutical Benefits Scheme (PBS), Repatriation Pharmaceutical Benefits Scheme (RPBS) or Pharmaceutical Integrated Logistics System (PILS) medication in the year before death.
- Between 2012 and 2018, a higher proportion (35%) of all ex-serving members were dispensed at least one mental health-related medication compared to Australians (18%).
- 60% of ex-serving males who died by suicide between 2013 and 2018 were dispensed mental health-related medications in the year before death compared with 54% of Australian males.
- Ex-serving ADF members who died by suicide between 2013 and 2018 and separated involuntarily for medical reasons were more likely to have been dispensed a mental health-related medication in the year before death (77%), compared to those who separated involuntarily for other reasons (47%) Meanwhile in 2018, a higher proportion of all ex-serving members who had separated due to medical reasons (44%) were dispensed a mental health medication, compared to those who separated voluntarily (18%).
- A higher proportion of ADF members who separated involuntary due to medical reasons between 2013 and 2018 were dispensed benzodiazepines (21%) and serotonin-norepinephrine reuptake inhibitors (13%) in the year before separation, compared to those who separated voluntarily (1% and 3%), or involuntarily due to other reasons (0.2 and 0.4%).
This chapter examines medications dispensed to ADF members who died by suicide compared to the Australian population who died by suicide. ADF members can access pharmaceuticals through the Pharmaceutical Benefits Scheme (PBS), the Repatriation Pharmaceutical Benefits Scheme (RPBS), and ADF-specific schemes such as the Pharmaceutical Integrated Logistics System (PILS). In this chapter, the time periods reported for medication dispensing under PBS, RPBS and PILS differs due to data availability. To address the data constraints, comparable time periods for the analysis are used to report on medications dispensing.
The PBS is available for current Medicare card holders (including serving, reserve and ex-serving members), and subsidises prescription medications listed under the scheme, subject to patient entitlement status. The RPBS is available for Department of Veterans’ Affairs Health Card holders (not all ADF members), and subsidises medications listed under the PBS, as well as additional medications and items for eligible ADF members, war widows and widowers, and their dependents.
Serving ADF members may also access medications via ADF-specific schemes such as through Defence pharmacies on barracks and dispensing in the field. Dispensing data from Defence pharmacies are collected and managed by the Pharmaceutical Integrated Logistics System (PILS).
Under the PBS and the RPBS, the Australian Government sets a maximum ‘co-payment’ amount that people pay towards the cost of their medicines. Prescriptions priced above the maximum co-payment for a patient are referred to as ‘subsidised’ (or ‘above co-payment’) prescriptions, and attract a subsidy from the Australian Government. Those priced below are referred to as ‘under co-payment’ prescriptions, and do not receive a subsidy.
Prior to 1 April 2012, the PBS/RPBS claims data did not collect data on under co-payment medications (See Appendix A5 – Pharmaceutical Benefits Scheme/Repatriation Pharmaceutical Benefits Scheme for further information). As such, this chapter focuses on medications dispensed from 1 April 2012 to 31 December 2018, and deaths from 1 April 2013 or 1 April 2014 to 31 December 2018 (when looking at medications dispensed 1 year or 2 years prior to death).
What is and isn’t included in the PBS/RPBS data?
The PBS/RPBS includes data on medications that are dispensed. It does not include information about medications that were prescribed (but not dispensed), or if the patient used the medication. PBS medications are specified by an item code that may include information about the therapeutic indication for which the medication was prescribed.
The PBS/RPBS data does not include medicines supplied to public hospital in-patients, over the counter medicines or private prescriptions. Unlisted medications may be prescribed to eligible RPBS members with DVA authorisation, however the data dare not coded consistently for analytic purposes.
What is and isn’t included in the PILS data?
PILS records data on medications and products that are dispensed. Unlike the PBS, PILS does not include information about the therapeutic indication for which medications have been dispensed. Many nervous system medications have more than one therapeutic indication.
PILS only collected dispensing data from on-barracks pharmacies until 2017, after which “in the field” dispensing is also included. Data for whether dispensing occurred on barracks or in the field is not supplied.
PILS dispensing is not limited to PBS listed medications and includes unlisted nervous system medications, and a range of pharmaceutical and non-pharmaceutical products that would normally be purchased over the counter without a prescription (see Appendix A5 for examples). PILS also includes some historically dispensed products where the data are not coded consistently enough for analytic purposes.
Medication dispensing under PBS, RPBS and PILS
Between 2013 and 2018, 81% of ex-serving ADF members who died by suicide were dispensed at least one product through PBS, RPBS or PILS in the year before death. Over two thirds (68%) were dispensed medications through PBS/RPBS, while 1 in 5 (20%) had any product dispensed through PILS.
The number of serving ADF members dispensed any PILS medication has steadily increased to just over 50,000 patients in 2018. In 2018, nearly all PILS users were dispensed a non‑nervous system-related product (99%), while 9% were dispensed a medication with a mental-health related indication (i.e. antidepressants, antipsychotics, anxiolytics, or hypnotics and sedatives).
How are medicines grouped?
This report uses the Anatomical Therapeutical Chemical (ATC) classification system, which groups medicines into five hierarchical levels according to the body system or organ on which they act. A single medication may have multiple classifications where it is used for multiple indications. For PBS/RPBS dispensing, PBS item codes are linked to a single classification.
Mental health‑related medications include five ATC level 3 groups: antipsychotics (code N05A), anxiolytics (code N05B), hypnotics and sedatives (code N05C), and antidepressants (code N06A) — prescribed by approved PBS prescribers. Psychostimulants, agents used for ADHD and nootropics (code N06B) are typically also included as mental health-related medications, but have been excluded due to small numbers. Some medicines classed as antiepileptics are also used for mental health conditions, but these too have been excluded as it is not possible to determine the reason for use from the available data.
Among ADF members who died by suicide, diazepam was the leading medicine dispensed to members who received at least one medicine, by number of persons dispensed (Table 18). For all Australians who died by suicide, paracetamol and codeine combination product was the most commonly dispensed medicine, and diazepam was the most commonly dispensed mental health medication.
|
Rank(c) |
ADF members, died by suicide(d) |
Australians, died by suicide(e) |
All ex-serving members(f) |
All Australians(g) |
|---|---|---|---|---|
|
#1 |
Diazepam* |
Paracetamol + codeine |
Amoxicillin |
Amoxicillin |
|
#2 |
Paracetamol + codeine |
Cefalexin |
Cefalexin |
Cefalexin |
|
#3 |
Amoxicillin + clavulanic acid |
Amoxicillin |
Amoxicillin + clavulanic acid |
Amoxicillin + clavulanic acid |
|
#4 |
Amoxicillin |
Diazepam* |
Paracetamol + codeine |
Paracetamol + codeine |
|
#5 |
Temazepam* |
Amoxicillin + clavulanic acid |
Oxycodone |
Esomeprazole |
|
#6 |
Cefalexin |
Temazepam* |
Doxycycline |
Atorvastatin |
|
#7 |
Oxycodone |
Oxycodone |
Roxithromycin |
Rosuvastatin |
|
#8 |
Mirtazapine* |
Mirtazapine* |
Meloxicam |
Oxycodone |
|
#9 |
Desvenlafaxine* |
Escitalopram* |
Prednisolone |
Salbutamol |
|
#10 |
Escitalopram* |
Quetiapine* |
Diazepam* |
Roxithromycin |
|
#11 |
Duloxetine* |
Tramadol |
Esomeprazole |
Pantoprazole |
* Medication with any mental health indication (Anxiolytics, Antidepressants, Antipsychotics, and Hypnotics and Sedatives) excluding Psychostimulants.
Notes
- Drugs are grouped by active ingredient(s) regardless of associated anatomical therapeutic classifications.
- Dispensing between 1 April 2012 and 31 December 2018. This time frame was chosen so that under co-payment PBS/RPBS data was available for full period. Dispensing is not limited to a specific time before death.
- Ranked by number of unique persons dispensed.
- All ex-serving, reserve, or serving members who served at least one day from 1 January 2001 to 31 December 2018 and died by suicide between 1 April 2012 and 31 December 2018 and were dispensed medications between 1 April 2012 and 31 December 2018.
- The Australian cohort are those who died by suicide between 1 April 2012 and 31 December 2018 and were dispensed medications between 1 April 2012 and 31 December 2018, excluding deaths by suicides by ADF members. The cohorts are restricted to the age range of the ex-serving male and female study population.
- All ex-serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018 and were dispensed medications between 1 April 2012 and 31 December 2018.
- The Australian cohort are all Australians, who were dispensed medications between 1 April 2012 and 31 December 2018. The cohorts are restricted to the age range of ex-serving ADF member study population
Source: AIHW analysis of PMKeyS-NDI-PBS, 2012-2018; Department of Health PBS/RPBS claims data, 2012-2018.
Between 2014 and 2018, among ADF members who died by suicide:
- 67% were dispensed mental health-related medications 2 years before death1 and 59% were dispensed 1 year before death (Figure 24).
- Thirty-one ADF members (16%) were dispensed PBS/RPBS medications or PILS products in the 7 days before death (Figure 24).
- All female ex-serving ADF members (15) were dispensed a medication in the year before death, compared to 82% of male ex-serving ADF members. A similar pattern of medication dispensing was observed for Australians who died by suicide, with 87% of females dispensed any medication compared to 77% of males.
- A higher proportion of ex-serving females was dispensed mental health‑related medication in the year prior to death than ex-serving males (93% compared with 60%), with a similar pattern observed in the Australian population (Figure 25).
Note: 1. It has been shown that significant effects of mental health prescribing on risk of suicide can be periods of up to 2 years before death, potentially due to recurrence or under-treatment of mental health conditions (O'Neill, Graham & Ennis 2019).
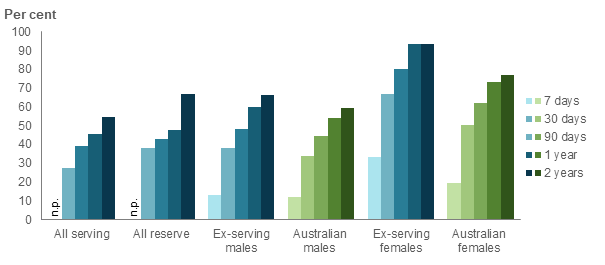
Figure 24: Percentage of ADF members(a) who died by suicide who were dispensed PBS/RPBS or PILS medications, by time before death(b), 2014 to 2018
Notes
- The ADF member cohort is all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 April 2014 and 31 December 2018. This time period was chosen so that under co-payment PBS/RPBS data was available for the full 2 years before each person’s death.
- The time before suicide is inclusive of the person’s death date, and excludes medications dispensed after their date of death. Scripts dispensed before a person was hired/terminated are included (provided they were dispensed within the time period being examined).
Source: AIHW analysis of PMKeyS-NDI-PBS-PILS, 2014-2018.
Figure 25: Percentage of ADF members(a) and Australians(b) who died by suicide who were dispensed PBS/RPBS or PILS mental health-related medication(c) by time period before death(d) and service status, 2014 to 2018(e)
Notes
- The ADF member cohort is all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 April 2014 and 31 December 2018.
- The Australian cohorts are males and females who died by suicide between 1 April 2014 and 31 December 2018, excluding ADF members. The cohorts are restricted to the age range of the ex-serving male and female study population .
- Mental health-related medications include anxiolytics, antidepressants, antipsychotics, and hypnotics and sedatives, but exclude psychostimulants due to small numbers.
- Time periods before death are inclusive of the person’s death date, and excludes medicines dispensed after their date of death. Medications dispensed before a person was hired/terminated are included (provided they were dispensed within the period).
- The 2014-2018 period was chosen so that under co-payment PBS/RPBS data was available for the full 2 years before each person’s death.
Source: AIHW analysis of PMKeyS-NDI-PBS-PILS, 2014-2018.
For ex-serving members who died by suicide between 2013 and 2018, antidepressants were the most commonly dispensed PBS/RPBS medication within 1 year of death, by number of persons dispensed (52%). This was followed by anxiolytics (25%), opioids (24%), ‘beta-lactam antibacterials, penicillins’ (23%), and antipsychotics (20%). This dispensing pattern was similar for Australians who died by suicide in the same period, for whom the leading medication type was antidepressants (46%), followed by opioids (25%), ‘beta-lactam antibacterials, penicillins’ (25%), anxiolytics (25%) and antipsychotics (20%).
Between 2012 and 20181 beta-lactam antibacterials, penicillins were the most commonly dispensed medication to all ex-serving ADF members: just over half (53%) were dispensed this medication at least once. This was followed by opioids (42%), ‘anti-inflammatory and antirheumatic products, non-steroids’ (35%), ‘other beta-lactam antibacterials’ (34%), and antidepressants (27%).
Four of the top 10 ATC 3 groups were mental health-related for ex-serving ADF members who died by suicide (antidepressants, anxiolytics, antipsychotics and hypnotics/sedatives), while just one mental health ATC 3 group was in the top 10 for the whole ex-serving population (antidepressants).
Note: 1. 1 April 2012 to 31 December 2018. This period includes under co-payment and subsidised PBS/RPBS data.
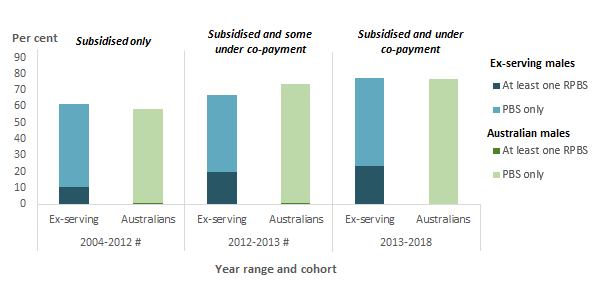
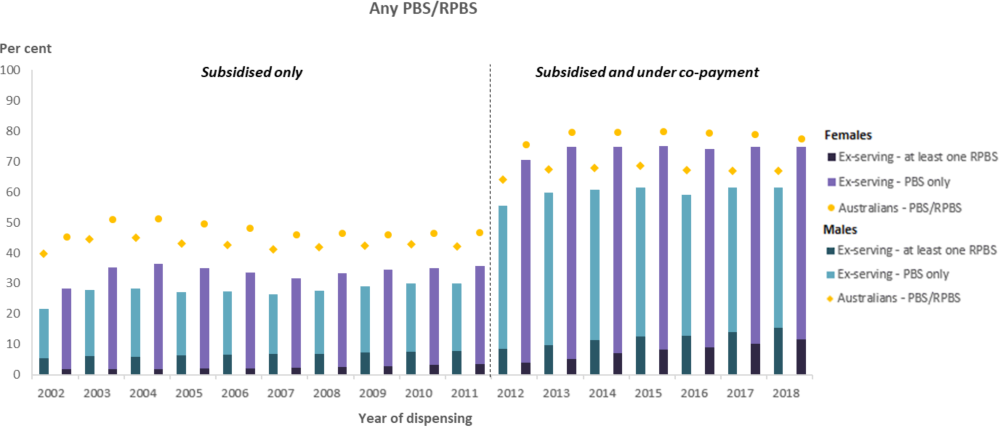
Around a quarter (23%) of ex-serving male ADF members who died by suicide between 2013 and 2018 were dispensed at least one RPBS-subsidised medication in the year before death (Figure 26). In comparison, the proportion of all ex-serving males who were dispensed a RPBS medication in a year ranged from 9% in 2012 to 15% in 2018 (Figure 27).
A similar proportion of ex-serving males who died by suicide between 2013 and 2018 (78%) and Australian males who died by suicide in the same period (76%) were dispensed any PBS or RPBS subsidised medication in the year before death (Figure 26).
Figure 26: Percentage of ex-serving(a) and Australian(b) males who died by suicide that were dispensed medication within 1 year of death(c), by year range of death(d), 2004 to 2018
Notes:
# Interpret with caution. Prior to 1 April 2012, only subsidised medications were included in the PBS/RPBS claims data. From 1 April 2012, both subsidised and under co-payment medications are included. As such data for the three time periods are not comparable.
- The ADF member cohort is all ex-serving, reserve and serving males who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 July 2004 and 31 December 2018.
- The Australian cohorts are males and females who died by suicide between 1 July 2004 and 31 December 2018, excluding ADF members. The cohorts are restricted to the age range of the ex-serving male and female study population.
- 'Within 1 year of death' is inclusive of the person’s death date, and excludes medicines dispensed after their date of death. Medications dispensed before a person was hired/terminated are included (provided they were dispensed within 1 year of death).
- The 2004-2012 reporting period refers to deaths between 1 July 2004 and 31 March 2012 (looking at medications dispensed 1 year before death). These medications were subsidised only. The 2012-2013 reporting period refers to deaths between 1 April 2012 and 31 March 2013, which will miss any under co-payment medications dispensed before 1 April 2012. The 2013-2018 reporting period refers to deaths between 1 April 2013 and 31 December 2018, which includes subsidised and under co-payment medications.
Source: AIHW analysis of PMKeyS-NDI-PBS, 2004-2018.
Figure 27: Percentage of ex-serving members(a) and Australians(b) dispensed PBS and RPBS medications(c), by sex and year, 2002 to 2018
Notes
- The ADF member cohort is all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 April 2014 and 31 December 2018.
- The Australian cohorts are males and females who died by suicide between 1 April 2014 and 31 December 2018. The cohorts are restricted to the age range of ex-serving male and female study populations.
- Medications dispensed to ex-serving members before they were terminated were excluded from the analysis (i.e. while they were serving or before they were hired). The denominator is the number of individuals who were ex-serving for at least one day in the reporting period. Interpret 2002 to 2012 with caution, as prior to 1 April 2012, only subsidised medications were included in the PBS claims data. From 1 April 2012, both subsidised and under co-payment medications are included. As such data is not comparable across the two time periods.
Source: AIHW analysis of PMKeyS-NDI-PBS, 2002-2018; Department of Health PBS/RPBS claims data, 2002-2018; ABS ERP 2002-2018.
Mental health-related medications
The proportion of all ex-serving ADF members who were dispensed PBS/RPBS mental health-related medications per year increased from 16% in 2012 to 21% in 2018 (Figure 28). Overall, 35% of the ex-serving population had at least one mental health-related medication dispensed over the 7-year period (while they were ex-serving), compared to 18% of Australians in the same period. Dispensing of mental health‑related medications should be interpreted with some caution, as some medications have more than one therapeutic indication, and may be prescribed to treat non-mental health, or off-label conditions, such as some antidepressants which are used off-label for neuropathic pain.
Figure 28: Percentage of ex-serving members(a) dispensed PBS/RPBS mental health-related medications, by type of medication and year, 2012 to 2018
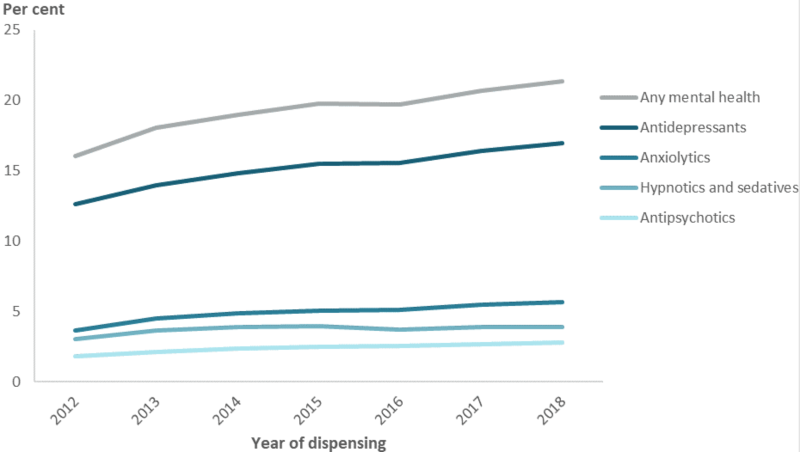
Note: (a) Medications dispensed to ex-serving members before they were terminated were excluded from the analysis (i.e. while they were serving or before they were hired). The denominator is the number of individuals who were ex-serving for at least one day in the reporting period.
Source: AIHW analysis of PMKeyS-NDI-PBS, 2012-2018.
Between 2013 and 2018, among those who died by suicide, a higher proportion of females were dispensed mental health-related medications in the year before death compared to males. This pattern can be observed in both the ex-serving (94% of females compared with 57% of males) and the Australian population (73% of females compared with 54% of males) (Figure 29).
A similar pattern is also observed by type of mental health-related medications dispensed. For example, 88% of ex-serving females were dispensed anti-depressants in the year before death compared with 47% of ex-serving males (Figure 29).
Figure 29: Percentage ADF members(a) and Australians(b) who died by suicide that were dispensed mental health-related medications within 1 year of death(c), by service status, 2013 to 2018(d)
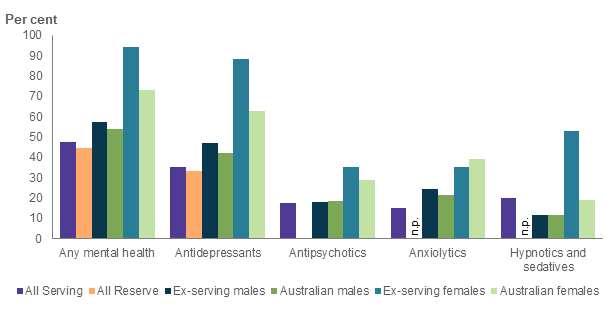
Interpret with caution–Some subcategories contain small numbers, refer to data tables for more information.
Notes
- The ADF member cohorts are all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 April 2013 and 31 December 2018.
- The Australian cohorts are males and females who died by suicide between 1 April 2013 and 31 December 2018, excluding ADF members The cohorts are restricted to the age range of the ex-serving male and female study population.
- 'Within 1 year of death' is inclusive of the person’s death date, and excludes medicines dispensed after their date of death. Medications dispensed before a person was hired/terminated are included (provided they were dispensed within 1 year of death).
- The 2013-2018 reporting period was chosen so that under co-payment PBS/RPBS data was available for year before each person’s death.
Source: AIHW analysis of PMKeyS-NDI-PBS-PILS, 2012-2018.
There has historically been concern that some classes of mental health-related medications may precipitate or increase the risk of suicidal ideation and behaviour (Möller et al 2008), however, evidence for this effect is mixed. A Therapeutic Goods Administration (2021) investigation into the risk of suicide for young people found that the current research is insufficient to conclude a causal relationship between antidepressant use and suicidal ideation; recognising that clinical worsening of symptoms and suicidality is a feature of depression itself in addition to a potential risk with the use of antidepressant medications. Meanwhile the relationship between benzodiazepine use and increased suicidality or suicide completion is unclear, being complicated by a range of confounding factors (Dodds 2017; Rothschild & Shindul-Rothschild 2017). This section explores the dispensing rates of antidepressants and benzodiazepines. Appendix A5 details the specific drugs selected for this analysis.
Among those who died by suicide:
- 33% of all serving, 19% of all reserve, and 30% of male ex-serving ADF members were dispensed benzodiazepines in the year before death (Figure 30).
- A higher proportion of female ex-serving ADF members were dispensed benzodiazepines in the year before death (65%) compared to male ex-serving members (30%), while similar proportions were dispensed selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) (Figure 30).
Figure 30: Proportion of ADF members(a) and Australians(b) who died by suicide who were dispensed selected drugs(c) within 1 year of death(d), by service status, 2013 to 2018(e)
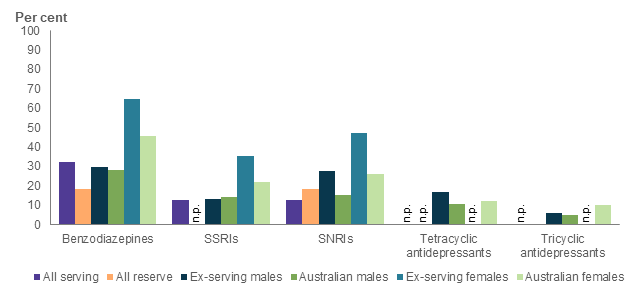
Interpret with caution–Some subcategories contain small numbers, refer to data tables for more information.
Notes
- The ADF member cohort is all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 April 2013 and 31 December 2018.
- The Australian cohorts are males and females who died by suicide between 1 April 2013 and 31 December 2018, excluding ADF members The cohorts are restricted to the age range of ex-serving male and female study population.
- Drugs include Benzopdiazepines: Temazepam, lorazepam, nitrazepam, diazepam, oxazepam, alprazolam; Selective serotonin reuptake inhibitors (SSRIs): Fluoxetine, paroxetine, escitalopram, vortioxetine; Serotonin-norepinephrine reuptake inhibitors (SNRIs): Venlafaxine, duloxetine, desvenlafaxine; Tetracyclic antidepressants: Mirtazapine; Tricyclic antidepressants: Amitriptyline, dosulepin (dothiepin), imipramine.
- 'Within 1 year of death' is inclusive of the person’s death date, and excludes medicines dispensed after their date of death. Medications dispensed before a person was hired/terminated are included (provided they were dispensed within 1 year of death).
- The 2013-2018 reporting period was chosen so that under co-payment PBS/RPBS data was available for the full year before each person’s death.
Source: AIHW analysis of PMKeyS-NDI-PBS-PILS, 2012-2018.
Between 2013 and 2018, ex-serving ADF members who died by suicide and separated involuntarily due to medical reasons were more likely to be dispensed mental health-related medications in the year before death (77%), compared to members who left involuntarily for other reasons (47%). In the same period, 64% of voluntary separations were dispensed any mental health-related medication in the year before death. Meanwhile in the total ex-serving ADF population between 2012 and 2018, a higher proportion (61%) of the medically separated cohort were dispensed mental health-related medication, compared to 30% of voluntary and 34% of other involuntary separations.
Between 2012 and 2018, the proportion of all ex-serving members who separated for medical reasons and were dispensed mental health medications in a year steadily increased from 33% in 2012, to 44% in 2018. This increase was higher than for those who left involuntarily for other reasons (from 14% to 19% over the same period) and voluntarily (from 14% to 18%) (Figure 31).
Figure 31: Percentage of ex-serving ADF members(a) who were dispensed a mental health medication, by separation reason and year, 2012 to 2018
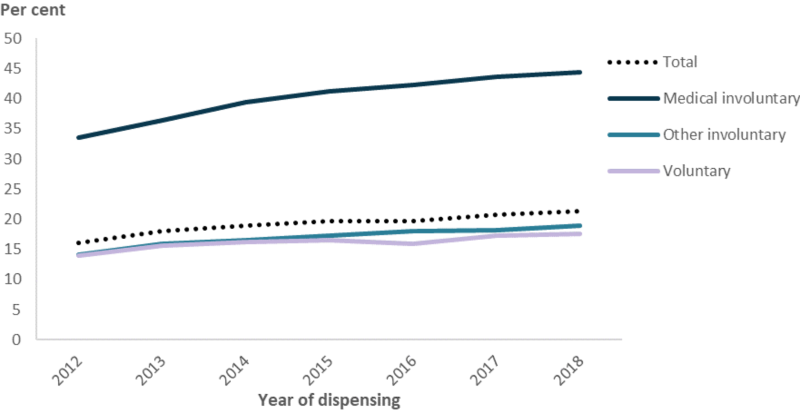
Note: (a) Medications dispensed to ex-serving personnel before they were terminated were excluded from the analysis (i.e. while they were serving or before they were hired). The denominator is the number of individuals who were ex-serving for at least one day in the reporting period.
Source: AIHW analysis of PMKeyS-NDI-PBS, 2012-2018.
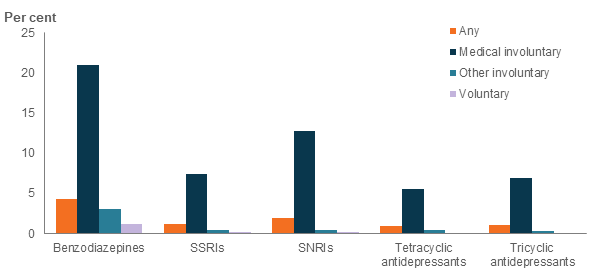
Prior to separation, ex-serving members had prescribed access to mental health-related medication from the Defence PILS dispensing system. Of all members who became ex-serving1, 8% were dispensed mental-health related medication from PILS in the year before separation and 4% were prescribed benzodiazepines (Figure 32). Of those who separated involuntarily due to medically reasons, 42% were dispensed any mental health medication from PILS in the year before separation, including 21% who were dispensed benzodiazepines, and 13% who were dispensed SNRI antidepressants.
Note: 1. Includes ADF members who became ex-serving between 2002 and 2018, or who became ex-serving prior to 2002 but who were hired on or after 1 January 2001 (i.e. PILS dispensing data is available for a minimum of 1 year before separation, or for the member's entire serving period).
Figure 32: Proportion of ex-serving ADF members(a) who were dispensed selected drugs(b) from PILS within 1 year of separation(c), by separation type, 2001 to 2018
Notes
- The ADF member cohort is all ex-serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and who separated on or after 1 January 2002 or were hired on or after 1 January 2001. This cohort was selected so that 1 year of service prior to separation or the member’s entire service period was available for analysis in the PILS data.
- Drugs include Benzopdiazepines: Temazepam, lorazepam, nitrazepam, diazepam, oxazepam, alprazolam; Selective serotonin reuptake inhibitors (SSRIs): Fluoxetine, paroxetine, escitalopram, vortioxetine; Serotonin-norepinephrine reuptake inhibitors (SNRIs): Venlafaxine, duloxetine, desvenlafaxine; Tetracyclic antidepressants: Mirtazapine; Tricyclic antidepressants: Amitriptyline, dosulepin (dothiepin), imipramine.
- 'Within 1 year of separation” includes the date of separation, and excludes dispensing events after their date of separation.
Source: AIHW analysis of PMKeyS-NDI-PILS, 2001-2018.