Technical notes
Data linkage, also known as data integration, is a process that brings together information relating to an individual from more than one source.
An extract of Department of Defence Personnel Management Key Solution (PMKeyS) data on 5 September 2020 provided records of all persons with ADF service on or after 1 January 2001. The file that was transferred to the AIHW contained 230,663 records. A total of 99,701 records were known by Defence to be of people who were alive and were de-identified before transfer. The remaining 130,962 records containing identifying information were in scope for linkage to the National Death Index (NDI) and Medicare Consumer Directory (MCD). Identifying information were provided for members who had an inactive employment status (i.e. terminated or deceased).
The AIHW undertook data linkage between the PMKeyS and NDI to determine the number of in-scope personnel who have died, and to confirm the cause(s) of death. This linkage was done using a probabilistic linkage procedure, based on the Fellegi and Sunter methodology, matching name, sex, date of birth, date of death and address, followed by a manual clerical review (Fellegi & Sunter 1969).
Linkages to the following data source:
- 130,625 links between PMKeyS and MCD
- 67,240 links between PMKeyS and DVA client data
- 3,239 links between PMKeyS and NDI data
All data linking was carried out by the Data Linkage Unit at the AIHW—one of only three accredited Commonwealth Integrating Authorities. This accreditation requires the AIHW to adhere to stringent criteria and abide by the National Statistical Service High level principles for data integration involving Commonwealth data for statistical and research purposes and Best practice guidelines. As well as these guidelines, data linkage at the AIHW is carried out under the protections of the Privacy Act 1988 and the Australian Institute of Health and Welfare Act 1987 (which carries additional privacy protections for companies and deceased people).
Strict separation of identifiable information and content data is maintained within the Data Linkage Unit in accordance with the AIHW linkage protocols, so that no one person will ever have access to both. Summary results from the linked data set are presented in aggregate format. Personal identifying information is not released, and no individual can be identified in any reporting. The linked data set created for this study will be stored securely on site at the AIHW for 7 years.
For more information on data storage, record retention and the privacy principles governing this study, see appendixes A7 and A8.
The scope of the study is all ADF personnel with at least 1 day of ADF service from 1 January 2001 to 31 December 2018. This means that, to be included in the total analysis set, a record must have a hire date before 1 January 2019, a termination date after 1 January 2001, and at least 1 day of service between the hire date and the termination date. Based on this definition and a number of logical checks performed, 14,023 records were excluded from analysis because they had met one of the following exclusion criteria:
- a termination date on or before 1 January 2001
- zero (0) days of service
- a hire date after the 31 December 2018
- duplicate records
- a date of death before 1 January 2001
- a date of death before the hire date
- a missing date of death
- a reason for separation of ‘Military – Irregular enlistment’ or ‘Military – Failed to enlist’ and less than 1 year of service. Irregular enlist/failed to enlist is considered out of scope as these individuals do not meet the criteria of having served 1 day in the ADF. Individuals within this group complete the enlistment process and do not attend the first day of service; therefore, they never complete 1 day in service.
This left a total of 216,640 unique in-scope records in the analysis data set.
Note, 354 ex-serving members’ records did not link to the MCD but have been included in the ex-serving population denominator in the use of health services and use of medicines analyses. Results from a sensitivity analysis showed a difference of less than 1% of the reported results when these records were excluded. To ensure consistency of denominator across these complex analyses, these unlinked records were included in the ex-serving population denominator.
Lag in cause of death information for the most recent year of data, where a death is registered in the following year.
Analysis in this study is based on year of occurrence of death. The National Death Index (NDI) is the source of information on fact of death in this study. Fact of death information from the NDI is supplemented with cause of death information from the National Mortality Database (NMD).
Analysis of the NMD for all Australian deaths shows that between 4% and 7% of deaths are not registered until the next year (ABS 2018b). These deaths are not captured in cause of death information, until data for the next year become available.
Cause of death data revisions (ABS)
Cause of death information for this report is based on final data for 2016 and preliminary data for 2017 and 2018. Cause of death for a small number of records linked to the 2017 (preliminary) and 2018 (preliminary) cause of death data may change where a death is being investigated by a Coroner and more up to date information becomes available as a result of the ABS revisions process. This may have a small effect on the number of deaths attributed to suicide in these years, as some deaths currently coded as ‘undetermined intent’ could later be identified as ‘intentional self-harm’.
Although this method likely captures the vast majority of suicides, there is potential for some to be missed if coronial findings are finalised or updated more than 4 years after a death.
Australian Bureau of Statistics (ABS) changes to mortality coding over the study period
The following information on mortality coding is sourced from the ABS. For further information, see the ABS Causes of death, Australia report.
Substantial changes to ABS cause of death coding were undertaken in 2006, improving data quality by enabling the revision of cause of death for open coroner’s cases over time. Deaths that are referred to a coroner (including deaths due to suicide) can take time to be fully investigated. To account for this, all coroner-certified deaths registered after 1 January 2006 are subject to a revisions process. This allows cause of death for open coroner’s cases to be included at a later stage where the case is closed during the revision period. Cause of death data are deemed preliminary when first published, with revised and final versions of the data being historically published 12 and 24 months after initial processing. Prior to 2006, revisions did not take place and as such it is recognised by the ABS that deaths by suicide may have been understated during this period (ABS 2018b).
As well as the above changes, new coding guidelines were applied to deaths registered from 1 January 2007. The new guidelines improve data quality by enabling deaths to be coded as suicide by ABS mortality coders if evidence from police reports, toxicology reports, autopsy reports and coroners’ findings indicates the death was due to suicide. Previously, coding rules required a coroner to determine a death as due to suicide for it to be coded as suicide.
The combined result of both changes has been the more complete capture of deaths by suicide, and a reduced number of deaths coded as ‘undetermined intent’, within Australian mortality data.
Detailed information on coding guidelines for intentional self-harm, and administrative and system changes that can have an impact on the mortality data set, can be found in Explanatory Notes 91-100 of Causes of death, Australia report (ABS 2018b).
National Coronial Information System (NCIS)
Information from the National Coronial Information System (NCIS) was used for coding associated causes of death and psychosocial risk factors, and to analyse sociodemographic characteristics. Mortality identifiers, also known as Mortality IDs, were used to identify ADF members who died by suicide in the NCIS. However, records for only 461 of the 465 deaths by suicide were available. Reasons that 4 deceased were not identified in the NCIS include:
- 3 cases did not have a mortality ID:
- 2 cases were identified through the Defence Suicide Database (DSD) but had not been recorded in the National Death Index (NDI) and therefore did not have mortality ID.
- 1 case was recorded in the NDI but had not been assigned a mortality ID. It was advised that this is an uncommon occurrence, however, two possible reasons are (Personal communication with the ABS):
- the person died overseas; or
- the coronial investigation remains open and the family did not require a death certificate. In this case their death may have initial paperwork lodgements with the Registry of Births, Deaths and Marriages but the final death registration has not yet been lodged with the ABS, and no mortality ID provided.
- 1 case did have a mortality ID however did not have a record in the NCIS.
Psychosocial risk factors (ABS)
Psychosocial risk factors analysed in this report were identified from coronial case investigation reports, coded by analysts at the ABS. As with other causes of death coding, some coronial cases are open at the time of initial coding (above) and further psychosocial risk factors may be identified as the investigation is finalised. The ABS revise the coding of causes of death 2 years after a case is opened, and will publish updated data, including psychosocial factors for Australian suicides, in 2021. The revised coding of causes of death may result in an increase in the proportion of suicides with psychosocial risk factors.
Coding psychosocial risk factors for suicide cases
The ABS piloted a project (ABS 2019b) analysing information from the National Coronial Information System (NCIS) to capture psychosocial risks for deaths referred to the coroner in 2017 (ABS 2019b). The ABS subsequently coded psychosocial risk factors for all Australian suicides 2017–2019 and for all suicides among ADF members between 2001–2018. 461 suicides were identified in the National Coronial System (NCIS) over the study period and are included in the following analyses. The ABS recorded risk factors for each suicide case if they appeared in one or more of the reports in the coronial system: including police, coroner or pathology reports. Psychosocial risk factors primarily arose in police and coronial reports.
Populations
Australian Defence Force
The Department of Defence supplied ADF population data for the serving full time and reserve study groups. Populations were available from 2002 onwards. Population data for the ex-serving group were calculated using the linked PMKeyS–NDI data from 2001 onwards, starting with zero (0) as at 1 January 2001. The analysis of ex-serving personnel was restricted to data from 2002 onwards, in line with reporting for serving and reserve groups. The populations used for analysis in this report were estimated as at 30 June each year.
It is important to note that the annual population size for each of the service status groups differs. While the serving and reserve populations are relatively stable over time at around 55,000 and 42,000 persons per year, respectively, the ex-serving population in the analysis set starts at zero (0) on 1 January 2001 and increases by around 5,000 persons per year. Unlike the serving and reserve populations, the ex-serving population is also ageing over time.
For these reasons, population rates have been used in addition to counts of suicides to illustrate the difference between service status groups.
Australian population
Australian population data used in this report were sourced from the ABS using the most up-to-date estimates available at the time of analysis (ABS 2020).
Rates
In this report, indirect age-standardisation has been applied to control for the difference in age structures between the ADF population (serving, reserve and ex-serving) and the comparison Australian population (see Standardised Mortality Ratios).
The presented rates refer to how often suicides occur in the three ADF service status groups, expressed as a number per 100,000 per year at risk.
Crude suicide rates are presented for service-related characteristics among the ex-serving population and expressed as number per 100,000 per year.
Comparison of proportions to the Australian population
In this report, the Australian comparison populations are age-restricted to the age range of the study population. For example, when comparing use of Medicare-subsidised services by ex-serving male population, the Australian comparison population is age-restricted to the age range of the ex-serving male population.
Standardised Mortality Ratio
Indirect age-standardisation was used to produce Standardised Mortality Ratio (SMR) for suicide. The SMR is a widely recognised measure used to account for differences in age structures when comparing death rates between populations. This method of standardisation can be used when analysing relatively rare events (i.e. where number of deaths is less than 25 for the analysed time period) (Curtin and Klein, 1995). The SMR is used to control for the fact that the three ADF service status groups have a younger age profile than the Australian population, and rates of suicide vary by age in both the study populations and the Australian population. The SMRs control for these differences, enabling comparisons of suicide counts between the three service status groups and Australia without the confounding effect of differences in age structure.
The SMR is calculated as the observed number of events (deaths by suicide) in the study population divided by the number of events that would be expected if the study population had the same age and sex specific rates as the comparison population.
SMRs higher than 1.0 indicate a higher number of suicides in the ADF population than expected; and SMRs less than 1.0 indicate a lower number of suicides than expected in the ADF population.
Confidence intervals and significance testing
Statistical significance is a measure that indicates how likely it is that an observed difference, or a larger one, would occur under the conditions of the null hypothesis. In the context of this study, the random element comes from the selection of the reference period. If a different reference period was used in the analysis, it is likely that some or all the observed rates would also be different. Statistical significance is reported to indicate how likely it is that the observed difference is due to that randomness alone.
To test statistical significance, assumptions must be made about the distribution of the number of deaths by suicide observed in a given time period. Suicide is a rare event within the study populations. If assuming that the chance of suicide is the same for all individuals within a study population and that deaths by suicide are independent of each other, it follows that one can assume that the number of deaths by suicide in the reference period follow a Poisson distribution. This assumption was made in conducting the significance test presented in this report.
In this study, 95% confidence intervals (CIs) are provided for each standardised mortality ratio (SMR) and suicide rates to indicate the level of uncertainty around these estimates due to random fluctuations in the number of suicides. It has been assumed that the number of suicides observed in the Defence population within a given time period is random and follows a Poisson distribution. Estimates produced using low numbers can be sensitive to small changes in numbers of deaths over time and will therefore have wide CIs. 95% CIs are provided within this report as they may account for the variation in absolute numbers of deaths by suicide. It is important to note that there are other sources of uncertainty, such as data collection error and linkage error, that are not captured by the provided CIs.
In this report, the Wald Z-statistic was applied to test whether the difference between rates is significant at the p=0.05 level, based on estimated standard errors for rate difference. The Wald Z-statistic measures how likely the observed difference between groups is due to random variability.
The PMKeyS data underpinning this study were extracted on 05 September 2020. This extract provided a snapshot of a number of demographic and service-related characteristics of ADF personnel as at this date, including rank, service, operational service status, employment status and service banding. A number of extra characteristics were then derived from this information in the original extract including age, service status, length of service, time since separation and vital status.
Length of service
The time between the date of hire and date of separation from the ADF. Analysis by length of service is presented for four broad groups: less than 1 year (<1), 1–<5 years, 5–<10 years, and 10 years or more (10+).
Service
The three broad arms of the ADF—Navy, Army and Air Force.
Service status groups
The three broad groups describing the nature of an individual’s employment with the ADF, namely:
- Serving: ADF members currently serving in a regular capacity in the Royal Australian Navy (Navy), Australian Army (Army) or the Royal Australian Air Force (Air Force) as of 31 December 2019, and still serving in a permanent regular capacity.
- Reserve: ADF members in the active or inactive reserve forces for the Navy, Army or the Air Force as of 31 December 2018, who are still in the reserve forces. Most members leaving full-time service transition to the inactive reserve forces (for a minimum of five years), unless prevented by medical or other grounds. The service status ‘Reserve’ includes members with a wide range of different experience and relationships to the ADF. For example, it includes both active and inactive reserves, as well as those who have only ever been reservists and those who served full time and then entered the reserves.
- Ex-serving: ADF members who served in the Service or Reserve Services between 1 January 2001 and 31 December 2018, but who subsequently separated from active service.
Time since separation
The period between separation from the ADF and death for ex-serving personnel who have died. Analysis by the time since separation is presented for four broad groups: less than 1 year (<1 year), 1 to less than 5 (1–<5) years, 5 to less than 10 (5–<10) years and 10 years or more.
Operational experience
There are four broad categories of deployment or operations:
- warlike operational service—warlike/active service deployments
- non-warlike operational service—non-warlike deployments (for example, peace keeping, peace monitoring, United Nations assistance missions)
- overseas operational service—humanitarian/disaster relief (international) or border protection deployments
- domestic operational service—deployment of Defence aid to the civilian community.
Individuals with at least one type of operational experience are counted in ‘Any’; those with no operational experience are counted in ‘None’. While the study scope includes those with at least 1 day of service between 2001 and 2018, individuals may have had operational experience at any time before this during their career. Only operational experience since 1 January 1999 has been consistently identified across these four broad categories. In this report, to ensure comparability, analysis of operational experience includes only those personnel hired on or after 1 January 1999.
Note, there are information on operational experiences for personnel who were hired before 1 January 1999 but it may be incomplete. See Table A5.1 for numbers and proportions of ADF personnel who were hired before or after 1 January 1999, by operational experience.
|
|
Serving |
Serving % |
Reserve Number |
Reserve % |
Ex-serving Number
|
Ex-serving % |
All ADF members Number |
All ADF members % |
|---|---|---|---|---|---|---|---|---|
|
All ADF members |
|
|
|
|
|
|
|
|
|
Hired before 01 January 1999(a) |
10,558 |
19.0 |
14,347 |
33.7 |
55,153 |
46.5 |
80,058 |
37.0 |
|
Any operational experience |
9,563 |
90.6 |
8,885 |
61.9 |
15,706 |
28.5 |
34,154 |
42.7 |
|
No operational experience |
995 |
9.4 |
5,462 |
38.1 |
39,447 |
71.5 |
45,904 |
57.3 |
|
Hired on or after 01 January 1999 |
44,880 |
81.0 |
28,271 |
66.3 |
63,431 |
53.5 |
136,582 |
63.0 |
|
Any operational experience |
32,357 |
72.1 |
16,578 |
58.6 |
16,860 |
26.6 |
65,795 |
48.2 |
|
No operational experience |
12,523 |
27.9 |
11,693 |
41.4 |
46,571 |
73.4 |
70,787 |
51.8 |
|
Total |
55,438(b) |
100.0 |
42,618(b) |
100.0 |
118,584 |
100.0 |
216,640 |
100.0 |
|
ADF members who died by suicide |
|
|
|
|
|
|
|
|
|
Hired before 01 January 1999(a) |
45 |
38.8 |
50 |
61.0 |
110 |
41.2 |
205 |
44.1 |
|
Any operational experience |
30 |
66.7 |
23 |
46.0 |
41 |
37.3 |
94 |
45.9 |
|
No operational experience |
15 |
33.3 |
27 |
54.0 |
69 |
62.7 |
111 |
54.1 |
|
Hired on or after 01 January 1999 |
71 |
61.2 |
32 |
39.0 |
157 |
58.8 |
260 |
55.9 |
|
Any operational experience |
29 |
40.8 |
17 |
53.1 |
32 |
20.4 |
78 |
30.0 |
|
No operational experience |
42 |
59.2 |
15 |
46.9 |
125 |
79.6 |
182 |
70.0 |
|
Total |
116 |
100.0 |
82 |
100.0 |
267 |
100.0 |
465 |
100.0 |
Notes
- Operational experience for personnel hired before 1 January 1999 may be incomplete.
- 8,879 ADF members with 1 day of service since 2001, who became ex-serving between 01 January 2019 and 05 September 2020, were re-assigned to either serving or reserve service status group based on their service status group information from PMKeyS extracted as at 05 September 2020.
Source: AIHW Analysis of PMKeyS–NDI, 2001–2018.
Entry type
Entry type describes the enlistment pathway taken by individuals into the ADF operational hierarchy. In this report, the analysis of service-related characteristics for ADF members suicide uses two categories of entry type. These categories are officers and general enlistees, which represent two entry streams into the ADF. Officer entry usually requires completing or undergoing tertiary qualifications and is geared towards leadership and managerial positions within the ADF. General enlistees make up the bulk of the ADF. Entry into this stream does not require previous experience or qualifications, and may be acceptable without a year-12 certificate.
Rank
Rank describes a person’s position in the hierarchy of the ADF within their specified service branch (i.e. Army, Navy and Air Force). Each service branch has their own nomenclature for each rank within the hierarchy but follow the same rank structure and thus ranks of equal standing across service branches can be determined. Ranks in the ADF can be represented in two broad groups:
- Commissioned officers—Ranks that hold leadership and managerial positions, denoted with the rank code prefix ‘O’ (O01 – O10)
- All other ranks—Ranks that are involved with general operations, denoted with the rank code prefix ‘E’ (E00 – E10)
In this analysis, ranks that were outdated and/or replaced by a modern equivalent were retained, while those that did not possess any rank information were excluded.
Reason for separation
The main reason recorded for a person’s separating (discharging) from the ADF. Analysis by reason for separation is presented for the following groups:
- voluntary separation—includes voluntary redundancies and resignations.
- involuntary separation—includes personnel deemed unsuitable for further duty for disciplinary, medical and operational reasons. Involuntary separation is further divided into separation for medical reasons, and non-medical involuntary separation (which includes being physically unfit for service, training failure and disciplinary reasons).
- Contractual/administration—include contractual change and/or changes in Defence personnel system (e.g. transitioning of payroll system to PMKeyS introduced from 2001).
The last_termination_reason variable in the PMKeyS data was used to group people for separation. Table A5.2 shows how the values for the last_termination_reason variable were allocated to the groups.
|
Separation reason type |
Last termination reason |
|---|---|
|
Voluntary |
APS resignation Comp FTS Discharge–open ended engagement Elective Military—Completed CFTS Military—Failed to enlist(a) Military—Resignation Military—Retired after CRAdate Military—Retired After Age 55 Military—Voluntary redundancy Military—Withdrawal within 90 days of enlistment Optional Own requirement Regulation instrument 088-4-5 Resigned Voluntary redundancy SR Separated Non Attendance SR Separated Non Contactable |
|
Involuntary |
Appointment cancelled Appointment terminated Discharged—unqualified Dismissed Marriage Medically unfit(b) Military—Below fitness standard Military—Civil offence Military—Disciplinary Military—False statement on enlistment Military—Irregular enlistment(a) Military—Management initiated retirement Military—Medically unfit for service(b) Military—Retention not in service interest Military—Training failure Military—Unsuitable for service (Defence personnel regulation 87-1-e) Not in interest Not required Physical standard Physically unfit Separated in service interest (Defence personnel regulation 70-SR) Resign Unq Separate—Other Reason Discharged in absence Military—In Absence Military—Compulsory Retire Age |
|
Contractual/Admin |
Cadet – Discharge/Retirement Cadet – ReHire Cadet – Reduction in Rank Cadet Transfer between Service Ceased Comp SSC Eng Expire Data Migration Requirement Military – Contract Completed Promotion for Cadets Rev O/Svc Serceas Tfr O/Svc Tfr REL Tfr Rsvs |
Notes
- Excluded from data set where length of service was less than 1 year.
- Included in the ‘Involuntary separation for medical reasons’ group.
Medicare-subsidised services
Medicare service groups are defined by the MBS item billed for the service, not the health care providers’ specialty. Data are reported by the date the service occurred, not the date of processing. For detailed information on the reported services and MBS items, see the Australian Government Department of Health MBS Online website.
|
MBS service |
MBS groups/items |
Notes |
|---|---|---|
|
Psychiatry |
Group A08; Items 855, 857, 858, 861, 864, 866, 14224, 134, 136, 138, 140, 142 |
Although there have been some changes to psychiatry MBS items over the years, use has been relatively consistent. |
|
GP mental health |
Groups A06, A20; Subgroups A07.4, A07.9, A18.4, A19.4, A30.3; Items 894, 896, 898, 20104 |
Interpret with caution: From 2000 to 2006, there were a limited number of GP mental health items so GPs claimed 'general' items instead (e.g. item 23). In 2002 and 2006 a range of mental health items were introduced, however GPs may still claim 'general' items. |
|
Allied mental health |
Groups M06, M07; Items 10956, 10968, 82000, 82015, 81325, 81355 |
This group combines the ‘Clinical Psychologist’, ‘Other Psychologist’ and ‘Other allied mental health’ groups to protect patient confidentiality. Interpret with caution: From 2000 to 2003, 100% of allied mental health services were not claimable through Medicare. From 2004 to now, an unknown percentage is claimed through Medicare. People can pay completely out-of-pocket, or access through other schemes (e.g. private health insurance, workers comp, public hospital visits, DVA, Employee Assistance Program etc.) |
|
GP attendances |
BTOS 101, 102, 103 |
|
|
Allied health |
BTOS 150, 900 |
Interpret with caution: From 2000 to 2003, allied health services were not claimable through Medicare. From 2004 to now, an unknown percentage is claimed through Medicare. People can pay completely out-of-pocket, or access through other schemes (e.g. private health insurance, workers comp, public hospital visits, DVA, etc.) |
What’s not in the MBS claims data?
Medicare does not cover all health services—reserve and ex-serving ADF members may access similar medical services through DVA funded programs (where eligible), while serving and reserve members can use Defence Health services. In addition, all Australians (including ADF members) may access services through other arrangements, such as private health insurance or workers’ compensation. These services are not captured in the MBS claims data.
In particular, caution should be taken when interpreting use of Medicare-subsidised allied health services (including psychologist services), as they are generally only available to patients with chronic, developmental or mental health conditions with a referral from a GP or specialist medical practitioner. Some Australians also access allied health services through their general (‘ancillary’ or ‘extras’) private health insurance, or pay for services entirely out‑of‑pocket.
Importantly, use of Medicare-subsidised services is not a measure of the prevalence of a health condition, as people may be using other services not captured in the MBS claims data, or may not access health care. There is no ideal rate of health care use and this report draws no conclusions about whether a higher or lower rate of service use is desirable for a particular cohort, nor does it try to assess the degree to which patient needs are being met.
DVA-funded health services
Services Australia, through Medicare, assesses claims and makes payments to allied health, medical and hospital providers who treat eligible ADF members, spouses and dependents on behalf of the Department of Veterans' Affairs (DVA). Groups for these services were in accordance with Table A5.3. Services provided through Medicare for eligible ADF members are the same as those provided to the Australian population. However, conditions of service need to be clarified with DVA. For example, Medicare benefits are available to the Australian population for up to 10 mental health services per patient per calendar year.
DVA also provides other out-of-hospital services that are not available through Medicare (Table A5.4). These services include dental, allied health, nursing care, prosthetic, operational equipment and pharmacy items. These items were grouped according to the ‘DVA Claiming Channel Overview – Items by Category’ information provided on the DVA website. In this study, where DVA-funded allied health services are similar to MBS allied health items, these services were grouped as ‘Allied health’ and/or ‘Allied health mental health’ services. For detailed information see the DVA Fee schedules.
|
Health services |
Items |
|---|---|
|
Clinical Psychology |
US01─US10, US43─US44, US50─US51, US55, US90, US99 |
|
Psychologists |
US11─US20, US41─US42, US52─54, US92, US98 |
|
Social worker (mental health) |
US21─US30, US93, US97 |
|
Occupational therapists (mental health) |
US31─US40, US45─US46 |
|
Neuropsychologists |
CL20─CL30 |
|
Mental Health Nurse |
MT22 |
|
Physiotherapy |
PH01─PH99 |
|
Optometrical Services |
OP01─OP99 |
|
Chiropractic |
CH01─CH99 |
|
Exercise Physiology |
EP01─EP99 |
|
Diabetes Educator |
CD01─CD99 |
|
Osteopathy |
OM01─OM99 |
|
Orthoptics |
OR10─OR99 |
|
Orthotists |
UT01─UT40 |
|
Podiatry (including footwear services) |
F004─F548, F604─F625, F660─F661, F670─F671, F680─F681, F984─F991, F999 |
|
Occupational therapists |
OT01─OT99 |
|
Social worker |
SW01─SW99 |
|
Dietitian |
DT01─DT99 |
|
Speech pathology |
SH01─SH99 |
DVA also funds hospital-based services. The data provided by DVA includes information on the care provided for non-admitted patients registered for care in emergency departments in selected public hospitals, and a compilation of episode-level records from admitted patient morbidity data collection systems from hospitals across Australia. An admitted patient undergoes a hospital’s formal admission process to receive treatment and/or care. This may be provided as a day-only or overnight admission. Day-only admissions are generally for treatment or care of at least 4 hours’ duration i.e. brief outpatient clinic appointments for consultation, review or testing are not captured in this data.
Separation is the term used to refer to an episode of admitted care, which can be a total hospital stay, or a portion of a hospital stay when there is a change in care type e.g. from acute care to rehabilitation care. Most episodes represent a single hospital stay. ‘Separation’ also refers to the completion of an epsiode of care i.e. changing care type, transferring to another hospital, discharge or death.
The principal diagnosis is the diagnosis established after study to be chiefly responsible for occasioning the patient’s episode of admitted patient care. An additional or secondary diagnosis is a condition or complaint that either coexists with the principal diagnosis, or arises during the episode of care. Generally, a secondary diagnosis should only be recorded if the condition affects patient management for that episode of care i.e.it cannot be assumed that the patient does not have a particular condition if it is not recorded. The diagnoses are coded according to International Statistical Classification of Disease and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM; Table A5.5).
The ICD-10-AM is used to classify diagnoses in the the Australian health sector. It is used in public and private hospitals, and in community and residential mental health care services. Although the ICD is primarily designed for the diseases and injuries with a formal diagnosis, it also classifies a wide variety of signs, symptoms, abnormal findings, complaints and social circumstances that may stand in place of a diagnosis. It is important to note that diagnostic classifications and coding standards have changed over time. There is also variation in the quality, completeness and depth of coding across services, and state-specific standards. These factors can impact on the accuracy of diagnostic information.
| Principal diagnosis (ICD-10-AM Chapter) | ICD-10-AM code range |
|---|---|
|
A00-A99, B00-B99 |
|
C00-C96, D00-D09, D37-D48 |
|
D50-D89 |
|
E00-E89 |
|
F00-F99 |
|
G00-G99 |
|
H00-H59 |
|
H60-H95 |
|
I00-I99 |
|
J00-J99 |
|
K00-K93 |
|
L00-L99 |
|
M00-M99 |
|
N00-N99 |
|
O00-O99 |
|
P00-P96 |
|
Q00-Q99 |
|
R00-R99 |
|
S00-T98 |
|
U50-Y98 |
|
Z00-Z99 |
|
U00-U49 |
A mental health flag indicating that a DVA client had received treatment or support for a mental health condition at least once, was derived from principal and secondary diagnoses in accordance with AIHW conventions1. This included primarily formal diagnoses but also symptoms, mental health assessment and psychosocial factors. The ICD-10-AM codes used to construct mental health diagnostic groups are included in Table A5.6.
Note: 1. AIHW (2021) Mental health services in Australia/classifications and technical notes
|
Principal diagnosis (ICD-10-AM Chapter) |
ICD-10-AM codes |
|---|---|
|
Stress-related disorders |
F43 |
|
Depressive disorders (excluding bipolar) |
F32 |
|
Drug and alcohol disorders |
F10-F19, Z502-3, Z714-5 |
|
Anxiety disorders |
F40-2, F44-8 |
|
Bipolar and mixed mood disorders |
F30-1, F33-9 |
|
Dementia |
F00-3, F051, G30 |
|
Schizophrenia and related disorders |
F20-9 |
Health Service Contract Off-base
The Health Service Contract (HSC) data collection contains health services provided to ADF members while serving. Defence contracts service providers including Medibank (from November 2012 to 30 June 2019) and Bupa (from 1 July 2019 to present) to deliver a range of health services such as services provided through Medicare that are the same as those provided to the Australian population.
Defence also provides other services that are not available through Medicare. These services include dental, allied health, hospitals, prosthetic, operational equipment and pharmacy items. In this report, where Defence-funded allied health services are similar to MBS allied health items, these services were grouped as ‘Allied health’ and/or ‘Allied health mental health’ services. Additionally, where Defence funded services that were categorised as ‘Mental health’ or ‘Psychiatry’ and are not available in Medicare, these services were classified as ‘Any mental health services’ in the report.
Table A5.7 shows allocation of service items across Medicare-subsidised, DVA-funded health services and Defence HSC Offbase to health service groups presented in this report.
Data quality issues were noted for records prior to 1 July 2013 (Personal communication with Defence) and as a consequent, analysis of services 1 year prior to death by suicide for ADF members who died in first half of 2014 would be an underestimate.
|
Health service |
Groups/items in MBS |
Items in DVA-funded services |
Items in HSC Offbase |
|---|---|---|---|
|
Psychiatry |
Group A08; Items 855, 857, 858, 861, 864, 866, 14224, 134, 136, 138, 140, 142 |
Groups/items as per MBS |
Groups/items as per MBS; Item Subcategory in ‘Psychiatry’. |
|
GP mental health |
Groups A06, A20; Subgroups A07.4, A07.9, A18.4, A19.4, A30.3; Items 894, 896, 898, 20104 |
Groups/items as per MBS |
Groups/items as per MBS |
|
Allied mental health |
Groups M06, M07; Items 10956, 10968, 82000, 82015, 81325, 81355 |
Groups/items as per MBS; US─US99; CL20─CL30; MT22. |
Groups/items as per MBS; US─US99; CL20─CL30; MT22. Item Subcategory in ‘Allied health’; Item Groups as ‘Psychology’ or ‘Mental Health’. |
|
Any mental health |
All items in Psychiatry, GP mental health, and Allied mental health |
All items in Psychiatry, GP mental health, and Allied mental health. |
All items in Psychiatry, GP mental health, and Allied mental health. Item Subcategory in ‘Mental Health’ and Item Group in ‘Mental Health’ or ‘Treatment Program’. |
|
GP attendances |
BTOS 101, 102, 103 |
Groups/items as per MBS |
Groups/items as per MBS. Item Subcategory in ‘GP Attendances’. |
|
Allied health |
BTOS 150, 900 |
Groups/items as per MBS; US─US99; CL20─CL30; MT22; CH01─CH99; EP01─EP99; CD01─CD99; OM01─OM99; OR10─OR99; OP01─OP99; PH01─PH99; UT01─UT40; F004─F548, F604─F625, F660─F661, F670─F671, F680─F681, F984─F991, F999; OT01─OT99; SW01─SW99; DT01─DT99; SH01─SH99 |
Groups/items as per MBS; Item Subcategory in ‘Allied Health’ and Item Groups in ‘Acupuncture’ ‘Audiology’ ‘Chiropractor’ ‘Diabetes Education’ ‘Dietetics’ ‘Exercise Physiology’ ‘Psychology’ ‘Physiotherapy’ ‘Podiatry’ ‘Occupational Therapy’ ‘Optometry’ ‘Remedial Massage’ ‘Speech Pathology’ ‘Treatment Program’. |
Pharmaceutical Benefits Scheme/Repatriation Pharmaceutical Benefits Scheme medications
PBS/RPBS data are presented by the date of supply, that is, when the prescription was dispensed to the patient.
Medicine groups are defined by the Anatomical Therapeutical Chemical (ATC) classification system, which groups medicines into five hierarchical levels according to the body system or organ on which they act.
The ATC classification version used is the primary classification as it appears in the PBS Schedule of Pharmaceutical Benefits (Table A5.8). This can differ slightly from the WHO version. There are three differences between the WHO ATC classification and the PBS Schedule classification that have a bearing on mental health data:
- Prochlorperazine is regarded as an antiemetic (A04A) in the PBS Schedule while it is an antipsychotic (N05A) according to the WHO classification. This means that information on prochlorperazine will not appear in the data provided as it is not listed as a mental health drug in the PBS Schedule.
- Also not appearing in the data is bupropion, listed as an anti-smoking drug (N07B) in the PBS Schedule while it is an antidepressant (N06A) according to the WHO classification.
- Lithium carbonate, on the other hand is classified as an antidepressant (N06A) in the PBS Schedule while it is an antipsychotic (N05A) according to the WHO classification. This means that lithium carbonate will appear in the data as an antidepressant rather than an antipsychotic1. In addition, some medicines in the mental health-related medicine groups may also be prescribed for non-mental health-related reasons (e.g. neuropathic pain).
Note: 1. AIHW 2020. Mental health services in Australia: Pharmaceutical Benefits Scheme and Repatriation Pharmaceutical Benefits Scheme data. Canberra: AIHW. Viewed 31 March 2021.
|
Medication type |
Classification |
|---|---|
|
ATC 3 codes N05A, N05B, N05C or N06A |
|
|
Antipsychotics |
ATC 3 code N05A |
|
Anxiolytics |
ATC 3 code N05B |
|
Hypnotics and sedatives |
ATC 3 code N05C |
|
Antidepressants |
ATC 3 code N06A |
|
Analgesics |
ATC 2 code N02 |
|
Other nervous system |
ATC1 code N and ATC2 code not N02 and ATC3 codes not N05A, N05B, N05C or N06A |
|
Non-nervous system |
ATC1 code not N |
|
Non-mental health |
ATC 3 code not N05A, N05B, N05C or N06A |
|
Any RPBS |
Patient category code R0 and R1 |
N06B (Psychostimulants) would normally be classified as a mental health medication, but has been excluded due to small numbers and has been included in other nervous system medications.
What’s in the PBS/RPBS data?
The PBS is available for current Medicare card holders (including ADF members), and subsidises prescription medicines listed under the scheme, subject to patient entitlement status. The RPBS is available for DVA Health Card holders (i.e. not all ADF members), and subsidises medicines listed under the PBS, as well as additional medicines and items for eligible ADF members, war widows and widowers, and their dependents.
Under both the PBS and the RPBS, the Australian Government sets a maximum ‘co‑payment’ that people pay towards the cost of their medicines. Prescriptions priced above the maximum co-payment are referred to as ‘subsidised’ (or ‘above co-payment’), and attract a subsidy. Those priced below are referred to as ‘under co-payment’, and do not receive a subsidy.
Prior to 1 April 2012, the PBS/RPBS data did not include data on under co-payment medicines. As such, this chapter focuses on medicines dispensed between 1 April 2012 and 31 December 2018, and deaths between 1 April 2014 and 31 December 2018 (when looking at medications dispensed 2 years prior to death).
The PBS/RPBS includes data on medications that are dispensed. It does not include information about medications that were prescribed and not dispensed, or if the patient used the medication.
The PBS/RPBS data also does not include information about medicines supplied to public hospital in-patients, non-RPBS over the counter medicines, medicines supplied through ADF specific-schemes, or private dispensing. Some over the counter medicines and other unlisted medications may be prescribed to eligible RPBS members, however the data does not contain sufficient information for analytic purposes.
Pharmaceutical Integrated Logistics System medications and other products
PILS data is presented by the date of supply, that is, when the prescription was dispensed to the patient.
Unlike PBS data, PILS products do not have an ATC assigned and the therapeutic indication for which the product has been dispensed is not specified. For example, gabapentin may be classified as an antiepileptic (N03A), or with other analgesics and antipyretics (N02B). Where a medication’s ATC classifications result in it being assigned to more than one medication type group, analysis on these groups show the margin of error ranging from all ambiguous items removed, to all ambiguous items included. The figure used for calculating proportions is the median of these two values. Affected groupings are Analgesics, other nervous system, non-nervous system, and one dispensing event for hypnotics and sedatives (and thus also any mental health) in 2002. Figure A1 shows the number of patients dispensed from PILS and the degree of ambiguity by drug class and year.
In addition to PBS/RPBS listed medications, PILS contains unlisted medications; over-the-counter (OTC) and pharmacist only medications; vitamins and supplements; and non-pharmaceutical consumer health products such as joint braces, bandages, and orthotics. Non-pharmaceutical items are included in non-nervous system, and consequently non-mental health and any dispensing.
PILS contains a number of over-the-counter medications with a nervous system related ATC. These have been assigned to a new group OTC nervous system medications rather than the group dictated by their ATC. These include:
- Paracetamol (excluding paracetamol combinations)
- Nicotine
- Caffeine
- Valerian root (Valerian officinalis) extract
- St John’s Wort (Hypericium perforatum) extract.
Figure A5. 1: Number of ADF members(a) dispensed from PILS(b)(c), by product group(d) and year, 2001 to 2018
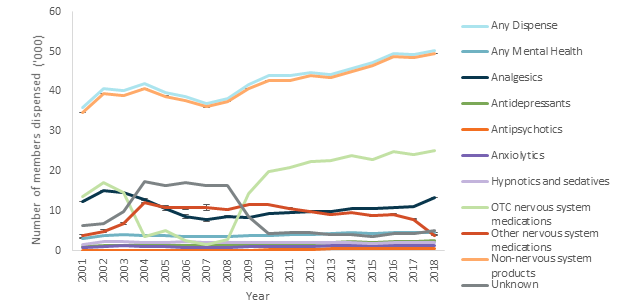
Notes
(a) The ADF member cohort is all ex-serving, reserve and serving personnel (all ages, males & females) who served at least one day from 1 January 2001 to 31 December 2018, and died by suicide between 1 January 2001 and 31 December 2018.
(b) Excludes PILS dispensing records marked as cancelled.
(c) Only on barracks dispensing is available until PILS was extended to off-barracks operations in 2017. Consequently, the number of members dispensed will vary according to historical deployment patterns prior to 2017.
(d) Ambiguous classification is shown with error bars.
Source: AIHW analysis of PMKeyS-NDI-PILS, 2012-2018.
What’s in the PILS data?
PILS data contains records for items dispensed from defence pharmacies to ADF members. Only on-barracks dispensing was captured until an unspecified point in 2017, after which in the field dispensing is also captured.
PILS data includes medications that are PBS/RPBS listed, unlisted medications including over-the-counter and pharmacist only medications, and non-pharmaceutical consumer health products such as joint braces, bandages, and orthotics.
Some products in PILS do not have sufficient information to determine the medication class, however reviewing the number of patients dispensed each medication group by year shows an increase in persons dispensed unidentified products between 2004 and 2008, and a corresponding decrease in persons dispensed OTC nervous system medications.
Select mental health medications with suspected suicidal side effects
Selected medications with suspected suicidal side effects were investigated as part of the integrated pharmaceutical dispensing analyses. Drugs included, their classification, and search terms used to identify records in PBS/RPBS/PILS are detailed below (Table A5.9), noting that not all requested drugs were identified in the data, and some classes were expanded to include additional drugs (vortioxetine & desvenlafaxine).
|
Drug group |
Drug name |
Search terms |
Persons with any PBS dispense events (2001-2018) |
Persons with any PiLs dispense events (2001-2018) |
Comment |
|---|---|---|---|---|---|
|
Benzodiazepines |
ALPRAZOLAM |
Alprazolam, Xanax, Alprax, Kalma |
62 |
109 |
|
|
|
DIAZEPAM |
Diazepam, Valium, Valpam, Antenex |
1558 |
4834 |
|
|
|
LORAZEPAM |
Lorazepam, Ativan |
0 |
0 |
No dispense events |
|
|
NITRAZEPAM |
Nitrazepam, Mogadon, Alodorm |
52 |
73 |
|
|
|
OXAZEPAM |
Oxazepam, Serapax, Alepam, Murelax, Serepax |
244 |
316 |
|
|
|
TEMAZEPAM |
Temazepam, Norminson, Temaze, Temtabs, Normison |
1354 |
8113 |
|
|
Selective serotonin reuptake inhibitors (SSRIs)
|
ESCITALOPRAM |
Escitalopram, Lexapro, Esipram, Cilopam-S, Lexam, LoxaLate |
1116 |
913 |
|
|
|
FLUOXETINE |
Fluoxetine, Prozac, Zactin, Lovan |
442 |
306 |
|
|
|
PAROXETINE |
Paroxetine, Aropax, Oxetine, Paxtine, Paxil, Extine, Roxet |
224 |
243 |
|
|
|
VORTIOXETINE |
Vortioxetine, Trintellix, Brintellix |
0 |
0 |
Added. No dispense events |
|
Serotonin-norepinephrine reuptake inhibitors (SNRIs) |
DESVENLAFAXINE |
Desvenlafaxine, Pristiq, Desfax, Ellefore, Desven |
520 |
297 |
Added |
|
|
DULOXETINE |
Duloxetine, Cymbalta, Dytrex, Duloxecor, Tixol |
433 |
524 |
|
|
|
VENLAFAXINE |
Venlafaxine, Effexor, Efexor, Elaxine, Enlafax |
574 |
659 |
|
|
Tetracyclic antidepressants |
MIRTAZAPINE |
Mirtazapine, Aurozapine, Axit, Remeron, Mirtanza, Mirtazon, Avanza, Milivin |
641 |
668 |
|
|
Tricyclic antidepressants |
AMITRIPTYLINE |
Amitriptyline, Endep, Entrip |
674 |
1740 |
|
|
|
DOSULEPIN (DOTHIEPIN) |
Dothiepin, Dosulepin, Dothep, Prothiaden |
49 |
48 |
|
|
|
IMIPRAMINE |
Imipramine, Tofranil |
25 |
25 |
|
|
Other antidepressants |
TRAZODONE |
Trazodone |
0 |
0 |
Not PBS listed/Not found in PiLs |
|
Quinoline antimalarials |
MEFLOQUINE |
Mefloquine, Lariam, Mephaquin, Mefliam |
0 |
0 |
Not PBS listed/Not found in PiLs |
|
|
TAFENOQUINE |
Tafenoquine, Kodatef, Kozenis |
0 |
0 |
Not PBS listed/Not found in PiLs |
In this report, a DVA client is defined as a veteran who satisfies at least one of the following criteria:
- has been issued a White or Gold card, or
- had at least one processed claim for a health or disability condition acquired during service, or
- received benefits or payment in the form of income support or compensation through the Military Compensation Scheme, or
- had at least one health service or support service through the DVA National Treatment Account.
Who is a DVA client?
DVA clients include serving, reserve, or ex-serving ADF members, or a partner or their dependents who receive support from DVA. A DVA client can be a DVA card holder, a benefit or income recipient and/or a user of health services or support services funded by DVA.
ADF members are eligible for benefits or payments in the form of compensation or income support if they have sustained an injury or health condition relating to their service. ADF members are also eligible for a service pension if they have provided qualifying service in an operational area.
Veteran cards are provided to identify the eligibility of current and former ADF members, and their dependents for a range of benefits. These can include health care, pharmaceutical benefits and concessional travel. There are several types of cards issued to DVA clients with the White card being the most common card type.
Between 2001 and 2018, policy changes have affected the types of conditions that qualify for benefit, the entitlements for benefit, and the process for submitting claims to DVA.1 For example, since July 2017 all current and former ADF personnel have been entitled to non‑liability health care for all mental health conditions. Since July 2018, all personnel discharged from the ADF have been automatically issued with a DVA health card (formerly a white card) that entitles them to non-liability health care for any mental health condition for the rest of their lives. ADF members are considered DVA clients from the date they first use this card.
Gold Cards
Holders of a Gold Card are entitled to DVA funding for all clinically necessary health services related to all health conditions, regardless of whether or not they resulted from service (DVA, 2021).
White Cards
White Card holders are entitled to health services related only to conditions accepted as resulting from service (DVA, 2019). However, cases of malignant cancer, pulmonary tuberculosis, and any mental-health condition do not have to be due to service-related causes.
From 1 July 2018, eligibility for treatment of any mental health condition expanded to include Reservists who have rendered Reserve Service Days with disaster relief service, border protection service or involvement in a serious service-related training incident. In addition, the White Card on Transition project commenced, with DVA issuing White Cards to transitioning members as they separate from the ADF.
Note: 1. The claim has been assessed by DVA with a decision outcome for the claimed condition under the relevant legislation: Military and Rehabilitation Compensation Act (MRCA) 2004, Veterans’ Entitlements Act (VEA) 1986, Safety Rehabilitation Compensation Act (SRCA) 1988 or Safety Rehabilitation Compensation (Defence-related Claims) (DRCA) Act 1988.
What is a processed claim?
In this report, a processed claim refers to:
- a claim a DVA client has lodged for compensation relating to a health or disability condition acquired during service;
and;
- has been assessed by DVA with a decision outcome (accepted or rejected) for the claimed condition under the appropriate legislation
These legislation include Military and Rehabilitation Compensation Act (MRCA) 2004, Veterans’ Entitlements Act (VEA) 1986, Safety Rehabilitation Compensation Act (SRCA) 1988 or Safety Rehabilitation Compensation (Defence-related Claims) (DRCA) Act 1988. Additionally, under non-liability health care arrangement, DVA clients are covered for treatment costs related to select health conditions, including cancer, pulmonary tuberculosis and a range of mental health conditions (DVA, 2021).
It is important to note that a DVA client can list multiple health or disability conditions on the one claim. The dataset received by the AIHW contains data at the condition level rather than the claims level (see Attachment E: Length of processing for more information). This means that it is appropriate to determine the number of people with a mental health or physical health condition related processed claim. The number of health or disability conditions as a measure of number of claims would not be reflective of the number of claims lodged by DVA clients.
Mental health processed claim
A processed claim relating to a mental health condition. See Technical Note below for search terms used for grouping of mental health conditions.
Accepted or Rejected claims
Accepted processed claims include the following decision outcomes: accepted, aggravated by war service (eligible for treatment), attributable to war service (eligible for treatment), paired organs and limbs policy applied or remitted.
Rejected processed claims include the following decision outcomes: deferred, no incapacity found, no jurisdiction, refused to deal with, rejected or suspended.
Mental Health Groupings
To identify the mental health conditions in the DVA Decisions data set, a library of key words was first established by conducting an exploratory search of the listed condition descriptions. Terms from the ICD-AM-10 were used to inform the search. In total, 159 terms were used to identify the mental health claims, which included iterations of mental health terms to account for misspelling of condition descriptions.
The terms were broadly grouped according to ICD-AM-10 chapter classifications (Table A6. 1: Groupings of Mental Health claims). The conditions listed under F43 (acute stress reaction, post-traumatic stress disorder, adjustment disorders) were placed in their own group. A miscellaneous group captured broad statements that did not fall into a specific grouping (e.g. psychological). The groups identified are listed below:
|
Mental Health Conditions |
ICD-10 Classifications |
|---|---|
|
Suicidal Ideation and Self-Harm |
R45.81, R45.89 |
|
Mood (Affective) Disorders |
F30 - F39 |
|
Post-traumatic stress disorder, acute stress reaction, adjustment disorders |
F43 |
|
Neurotic, Stress-Related and Somatoform Disorders |
F40 - F48 (excluding F43) |
|
Mental and Behavioural Disorders due to Psychoactive Substance Use |
F10 - F19 |
|
Behavioural Syndromes Associated with Physiological Disturbances and Physical Factors |
F50-F59 |
|
Schizophrenia, Schizotypal and Delusional Disorders |
F20-F29 |
|
Disorders of Adult Personality and Behaviour |
F60-F69 |
|
Organic, including Symptomatic, Mental Disorders |
F00 - F09 |
|
Disorders of Psychological Development |
F80-F89 |
|
Behavioural and Emotional Disorders with Onset Usually Occurring in Childhood and Adolescence |
F90-F98 |
|
Miscellaneous terms (e.g., behavioural, psychological, psychiatric) |
N/A |
Data provided and created for this study are stored as per AIHW information security protocols. No third parties (including DVA) have access to any identified data. Any data provided to DVA by the AIHW are in aggregated and de-identified form and stored in accordance with DVA’s security processes and procedures.
Data stored and analysed at the AIHW are protected under the Privacy Act 1988 and the Australian Institute of Health and Welfare Act 1987. The AIHW is subject to the Public Service Act 1999 and the APS Code of Conduct. As well, it has issued formal Guidelines for the Custody of Institute Data as a further measure to ensure data protection.
The AIHW performs data linkage projects on a separate secure private network to which only Data Integration Services Centre (DISC) staff and the Systems Manager have access. Dedicated DISC infrastructure capabilities replicate the hardware already used with success on other large data integration projects across the AIHW. This environment is separate from any other AIHW systems. The AIHW connects, via the Intra Government Communications Network, to an internet gateway provider accredited by the Australian Signals Directorate; the AIHW‘s internet gateway is certified to the PROTECTED level. DISC projects are undertaken on a separate secure network not connected to the internet.
The AIHW uses best practice technology, procedures and policies to protect its information and communication technology assets. A layered system of security is in place, with different technologies and techniques used at different levels. In line with the Australian Government Protective Security Policy Framework:
- passwords are changed regularly;
- accounts are locked out after three failed attempts;
- Operating System patching of desktops, networking equipment and servers is done in line with Australian Signals Directorate guidelines;
- application software updates are tested and applied as soon as practical after release;
- access to the data centre is controlled by swipe card;
- the network has a state-of-the art firewall to protect against external intrusion, beyond which the accredited gateway has its firewalls;
- anti-virus software is constantly updated;
- regular backups are taken, including rotation to a secure off-site storage facility; and,
- desktops have been hardened to prevent users from installing software or tampering with the system.
These security measures are backed up by an auditing regime, based around tightly controlled separate information domains (staging, linking, and consolidation domains) that exist for each stage of creating the project data. Each project in each information domain is in a separate storage location, with access limited by user (different users in different information domains for separation requirements).
This architecture determines who can access what data at any time, and access is therefore predetermined and logged. Work logs of basic user and time/date information are generated when code is run against these data and are stored as part of the audit trail.
In summary, access is provided to individuals for each stage of a project. This allows the AIHW to determine and log all access rights to the data throughout the process. At the completion of the project, and in line with the data retention date, the AIHW uses Sdelete (Microsoft) to remove all files relating to a project from the hard disk. In line with DISC data retention/backup cycle procedures, data are overwritten on a 4-weekly cycle. Data are encrypted as part of the archival process using Commvault.
This study is conducted under strict privacy guidelines and the oversight of organisational ethics committees.
Privacy principles
The Privacy Act 1988 sets out 13 Australian Privacy Principles that govern agencies of the Australian Government in their collection, storage, use, disclosure and management of data containing personal information. The Privacy Act permits the handling of health information for health and medical research purposes in certain circumstances, where researchers are unable to seek individuals’ consent. This recognises the need to protect health information from unexpected uses beyond individual health care as well as the important role of health and medical research in advancing public health.
The Privacy Commissioner has approved two sets of legally binding guidelines, issued by the National Health and Medical Research Council. Researchers must follow these guidelines when handling health information for research purposes without individuals’ consent. The guidelines also assist Human Research Ethics Committees (HRECs) in deciding whether to approve research applications. The guidelines are produced under sections 95 and 95A of the Privacy Act, detailing procedures that HRECs and researchers must follow when personal information is disclosed from an Australian Government agency for medical research purposes, and providing a framework for HRECs to assess proposals to handle health information for health and medical research (without individuals’ consent). They ensure that the public interest in the research activities substantially outweighs the public interest in the protection of privacy.
Ethics approval
The AIHW Ethics Committee, and the Defence-DVA Human Research Ethics Committee accepted that the public interest in the research activities of this project substantially outweighs the public interest in the protection of privacy, and approved the study pursuant to Section 95 of the Privacy Act.
NCIS: privacy and confidentiality
On 5 May 2020, the AIHW Ethics Committee (EC) approved the data sets required by the AIHW and the ACSQHC for the purposes of the Review, including the secure transfer of a list of non-identifiable pins (Mortality ID) relating to suicides among ADF members from the AIHW to the ABS to enable ICD coding of deaths, including psycho-social risk factors that have been identified as suicides among ADF members. This was noting that psycho-social coding is not currently included in the ABS Cause of Death information in the National Death Index. As this is for deceased persons only, the Privacy Act does not apply.
The use of ‘Mortality ID’ is required to identify relevant cases in the online NCIS system and facilitate the ICD coding of NCIS data by the ABS, including coding of psychosocial risk factors. To facilitate this process, the AIHW provided ABS with the Mortality IDs for the suicides between 1 January 2001 and 31 December 2018 identified through linkage between Defence personnel data (PMKeyS) and the National Death Index.
Data governance
AIHW is an Integrating Authority. This means it has met stringent criteria covering project governance, capability and data management. It abides by the principles for data integration involving Australian Government data for statistical and research purposes, and the best practice guidelines. It can integrate Australian data for high-risk research projects because it upholds strict privacy and confidentiality requirements.