Biomedical risk factors
Web article
Release Date:
Section: Determinants of health
Citation
AIHW (Australian Institute of Health and Welfare) (2026) Biomedical risk factors, AIHW, Australian Government, accessed 13 July 2026.

Biomedical risk factors are bodily states that have an impact on a person’s risk of disease. There are several biomedical risk factors that contribute to the risk of developing chronic health conditions. Biomedical risk factors outlined in the National Preventive Health Strategy 2021–2030 include:
- high or low blood pressure (see Hypertension in Australia)
- high blood glucose levels
- overweight or obesity, and underweight (see Overweight and obesity)
- high blood cholesterol
- genetics, epigenetics, and telomere biology (Department of Health 2021).
Biomedical risk factors are closely related to behavioural risk factors such as tobacco use and dietary risk factors (Department of Health 2021). They may also be affected by other determinants of health including social, commercial, and environmental determinants. For more information, see What are determinants of health?
This page focuses on 3 biomedical risk factors – high blood glucose, high blood pressure and high blood lipids – which have been directly linked to specific health outcomes such as cardiovascular disease, including coronary heart disease and stroke, chronic kidney disease and diabetes. Overweight and obesity are discussed in Overweight and obesity.
To report on the 3 biomedical risk factors, this report uses the Australian Bureau of Statistics (ABS) 2022–24 National Health Measures Survey (NHMS), which collected self-reported and measured data on blood pressure, blood glucose and cholesterol.
The ABS 2022 National Health Survey (NHS) is also used to report on hypertension which is a condition when blood pressure is consistently high. The NHS collected measured data on blood pressure as well as linked survey participants’ NHS data with Pharmaceutical Benefits Scheme (PBS) data, which is used to determine whether someone was on medications for hypertension. For more information, see Hypertension in Australia.
For more information on the health surveys, see the ABS’s Intergenerational Health and Mental Health Study.
Key messages
Blood glucose
- High blood plasma glucose (including diabetes) was responsible for 4.2% of total disease burden in Australia and was the fifth leading risk factor contributing to ill health and premature death in 2024.
- An estimated 2.7% of adults aged 18 and over were at risk of diabetes with measured impaired fasting glucose in 2022–24.
Blood pressure
- High blood pressure was responsible for 4.4% of the total disease burden, making it the fourth leading risk factor contributing to ill health and premature death in 2024. High blood pressure contributed to a higher proportion of fatal burden (7.2%) than non-fatal burden (2.0%).
- An estimated 39% of adults aged 18 and over (approximately 7.2 million adults) had hypertension, in 2022–24.
- Of adults with hypertension, 40% had controlled their blood pressure using medications. More females aged 18 and over (42%) than males (37%) had their hypertension controlled.
- 24% of adults had high measured blood pressure in 2022–24 – higher than in 2011–12 (22%). After adjusting for the effects of age, the rate of measured high blood pressure has remained similar over the last decade.
Blood lipids (cholesterol and triglycerides)
- High cholesterol levels were responsible for 2.3% of ill health and premature death in 2024. It contributed to 36% of total coronary heart disease burden and 15% of stroke burden.
- An estimated 30% of adults aged 18 and over had measured high cholesterol in 2022–24.
- 59% of Australian adults had dyslipidaemia (blood lipids outside of the healthy range) in 2022–24. This included 49% with uncontrolled dyslipidaemia and 10% with optimal blood lipid levels who were taking lipid-modifying medication.
Multiple biomedical risk factors
1 in 6 (17%) Australian adults had both measured high blood pressure and dyslipidaemia in 2022–24.
Blood glucose
The inability to regulate blood glucose is a characteristic of diabetes and the initial stages of type 2 diabetes, also known as pre-diabetes.
A person may not currently have diabetes but record glucose levels above the recommended range, either in the fasting or non-fasting state, placing them at significant risk of diabetes. This includes impaired fasting glucose and impaired glucose tolerance.
It is also possible for blood sugar to become too low (hypoglycaemia). This can occur in people with diabetes if they have taken too much medication, have not eaten enough or have been more active than usual, and can be life threatening if not treated (Diabetes Australia n.d.; Health Direct n.d.).
Burden of high blood plasma glucose (including diabetes)
Burden of disease is a measure of the years of healthy life lost from living with illness and injury and dying prematurely. A portion of disease burden is due to modifiable risk factors. Burden of disease analysis estimates the contribution of these risk factors to this burden. These estimates reflect the amount of disease burden that could be avoided if exposure to this risk factor can be avoided or reduced to the lowest possible exposure.
High blood plasma glucose (including diabetes) was responsible for 4.2% of the total burden of ill health and premature death and was the fifth leading risk factor in Australia in 2024 (AIHW 2024). High blood plasma glucose includes the direct and indirect health effects of type 1 diabetes, type 2 diabetes, other diabetes, and high blood plasma glucose (Figure 1).
Type 2 diabetes contributed 2.2% of the total burden of disease in Australia in 2024 (Figure 1). More than half of the high blood plasma glucose attributable burden is from the direct health effects of type 2 diabetes. Much of this burden can be prevented by addressing health determinants which lead to risk factors for type 2 diabetes. Other risk factors include overweight and obesity, dietary risks, insufficient physical activity, air pollution, tobacco smoking, high blood pressure and excess alcohol intake.
For more information, see Australian Burden of Disease Study 2024, Diabetes: Australian facts and Risk factors for diabetes.
Figure 1: Burden of disease directly and indirectly attributable to high blood plasma glucose in 2024
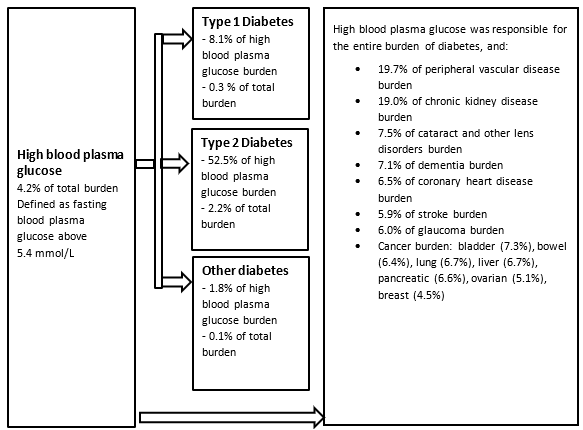
Note: High blood plasma glucose is defined as per the Australian Burden of Disease Study (AIHW 2024)
Source: AIHW 2024
Self-reported data on impaired fasting plasma glucose
In 2022–24, among adults (aged 18 and over), a small number of people (0.5%) who did not have diabetes, reported having high glucose levels measured in their blood or urine (ABS 2025a). This has remained steady since 2017–18 (0.5% of adults) (ABS 2018). Men (0.5%) and women (0.6%) reported similar levels of having high glucose levels measured in their blood or urine (ABS 2025a).
Measured data on impaired fasting plasma glucose
Self-reported data can underestimate the true impact of impaired glucose regulation in the population, as people can be unaware that they have impaired glucose regulation. In the 2022–24 National Health Measures Survey (NHMS), impaired glucose regulation was assessed via measurement of fasting plasma glucose levels (a blood test). The proportion of adults (aged 18 and over) who were identified in 2022–24 as being at high risk of diabetes with impaired fasting plasma glucose was 2.7%. This was higher among men (3.6%) than women (1.7%) (ABS 2025b).
Blood pressure
Blood pressure is the force exerted by the blood on the walls of the arteries as the heart pumps blood around the body.
Measured high blood pressure is when the force of the blood pushing against the wall of the arteries is too high. Hypertension is a diagnosed medical condition when blood pressure is consistently high. This can lead to other serious health conditions and is a major risk factor for many chronic conditions, including stroke, coronary heart disease, heart failure and chronic kidney disease.
Treatment of hypertension is usually through a combination of lifestyle changes (eating a healthy diet, keeping active, avoiding smoking) and taking medication. Well controlled high blood pressure means blood pressure measurements are in the optimal range – where the systolic blood pressure is less than 130 mmHg and/or diastolic blood pressure is less than 80 mmHg. A doctor will advise patients what their ideal blood pressure should be, based on their medical history (Health Direct n.d.; Heart Foundation n.d.).
Definitions
High measured blood pressure
High measured blood pressure is defined as having:
- systolic blood pressure greater than or equal to 140 mmHg and/or
- diastolic blood pressure greater than or equal to 90 mmHg.
A single high measurement indicates a need for further medical follow-up.
Hypertension
Hypertension is defined as:
- having high measured blood pressure (i.e. systolic blood pressure is greater than or equal to 140 mmHg, and/or diastolic blood pressure is greater than or equal to 90 mmHg), and/or
- receiving medication for high blood pressure (Whitworth 2003)
Hypertension diagnosis is based on multiple blood pressure readings on separate occasions. Generally, if you have a high blood pressure reading taken on at least 2 separate days by a health professional, you may have a diagnosis of hypertension (Health Direct n.d.; Heart Foundation n.d).
Controlled and uncontrolled hypertension
Hypertension can be controlled through taking medications to reduce blood pressure (antihypertensive medications).
Controlled hypertension is defined as people who are taking medication for hypertension and have a blood pressure reading within the recommended ranges.
Uncontrolled hypertension is defined as people with blood pressure readings above the recommended ranges, regardless of whether they are taking medications.
Burden of high blood pressure and hypertensive heart disease
High blood pressure
In 2024, high blood pressure contributed to 4.4% of ill health and premature deaths (total disease burden), making it the fourth leading risk factor, after overweight (including obesity), tobacco smoking and dietary risk factors. High blood pressure contributed more to fatal burden (dying prematurely) at 7.2% than non-fatal burden (living with illness and injury) at 2.0% (AIHW 2024).
It was estimated that high blood pressure contributed to 61% of hypertensive heart disease total burden, 40% of coronary heart disease burden, 37% of stroke burden, 35% of chronic kidney disease burden, and 29% of atrial fibrillation and flutter burden in 2024 (AIHW 2024).
Hypertensive heart disease
Australians lost around 16,400 years of healthy life due to living with, and dying from hypertensive heart disease, in 2024. It accounted for 0.3% of total disease burden and 2.4% of the cardiovascular disease burden.
Most of the burden due to hypertensive heart disease was from fatal burden (98.7%), compared with 1.3% from non-fatal burden.
Males experienced more burden (54%) from hypertensive heart disease than females (46%). People aged 60 and over experienced the most burden, accounting for 83% of the burden from the condition (AIHW 2024).
Hypertension
Based on measured blood pressure data and linked PBS dispensed medications data, 39% of Australian adults aged 18 and over were estimated to have hypertension, in 2022. This is approximately 7.2 million adults. There was a similar proportion of males (40%) and females (39%) with hypertension (Figure 2).
Hypertension became more common with increasing age, with the lowest seen in those aged 18–24 (7.0%) and the highest in those aged 75 and over (85%). This pattern was seen in both males and females (Figure 2).
Figure 2: Proportion of adults aged 18 and over with hypertension, by sex and age group, 2022
The bar chart shows rates of hypertension in adults aged 18 and over increasing with age. This increase was seen in both males and females.

Figure 3: Proportion of adults with hypertension who have their hypertension controlled with medication, by sex and age group, 2022
The bar chart shows that females aged 18+ have higher rates of controlled hypertension in younger age groups compared with males, but the difference reduces between the sexes in older age groups.
