Atrial fibrillation as a principal or additional diagnosis
On this page
In hospitalisations where AF coexisted with a different principal diagnosis, and affected the care provided during hospitalisation, it was recorded as an additional diagnosis.
There were over 218,000 hospitalisations where AF was either the principal or additional diagnosis in 2017–18—an age-standardised rate of 729 hospitalisations per 100,000 population. Of these, one-third (33%) recorded AF as the principal diagnosis and two-thirds (66%) recorded AF as an additional diagnosis.
Hospitalisation of persons with AF as either the principal or additional diagnosis accounted for 1.9% of all hospitalisations in 2017–18.
Hospitalisations with AF as an additional diagnosis were more likely to involve a longer length of stay than admissions where AF was the principal diagnosis. The average length of stay for hospitalisations with either a principal or additional diagnosis of AF was 9.9 bed-days, with 6.2% of hospitalisations discharged on the same day.
Principal diagnoses where atrial fibrillation was an additional diagnosis
In 2017–18, the leading principal diagnoses where AF was an additional diagnosis included:
- other CVDs: heart failure, cerebral infarction (stroke), acute myocardial infarction (heart attack) and chronic ischaemic heart disease
- pneumonia
- sepsis
- chronic obstructive pulmonary disease (COPD)
- fracture of femur (Data table 10).
Population groups
Among population groups, when AF is considered as either a principal or an additional diagnosis, different patterns emerge compared to principal diagnosis alone. In 2017–18, AF hospitalisation rates (combined principal and additional diagnosis) were higher among Indigenous Australians, and increased with remoteness and socioeconomic disadvantage (Figures 4 and 5).
Aboriginal and Torres Strait Islander people
In 2017–18, there were 4,400 hospitalisations, where AF was the principal or additional diagnosis, for Aboriginal and Torres Strait Islander people. This represents a crude rate of 531 hospitalisations per 100,000 population
The hospitalisation rate, where AF was the principal or additional diagnosis, was:
- higher for Indigenous Australians than for non-Indigenous Australians across sex and age groups, with the exception of males aged 75 and over
- 2.0 times as high for Indigenous males aged 55–64 compared with non-Indigenous males aged 55–64 years (2,459 and 1,260 per 100,000 population)
- 3.3 times as high for Indigenous females aged 55–64 compared with non-Indigenous females aged 55–64 years (1,789 and 547 per 100,000 population) (Figure 4).
After adjusting for differences in the age structures between the population, the rate of hospitalisations, where AF was the principal or additional diagnosis, was 1.6 times as high for Indigenous Australians compared with non-Indigenous persons (1,123 and 710 per 100,000 population).
Figure 4: Atrial fibrillation hospitalisation rates, principal and additional diagnosis, by Indigenous status, age and sex, 2017–18
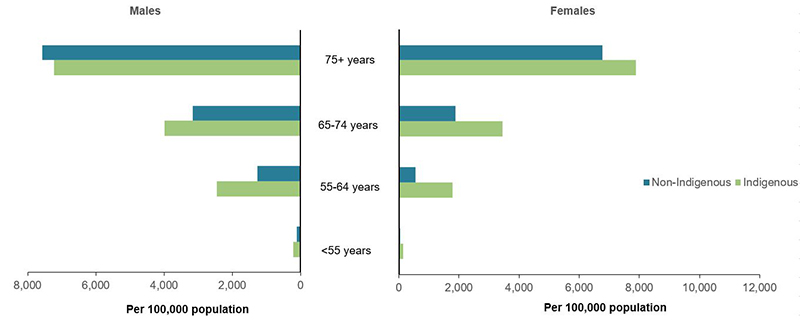
Source: AIHW National Hospital Morbidity Database. (Data table 7)
Figure 5: Atrial fibrillation hospitalisation rates, principal and additional diagnosis, by sex and population group, 2017–18
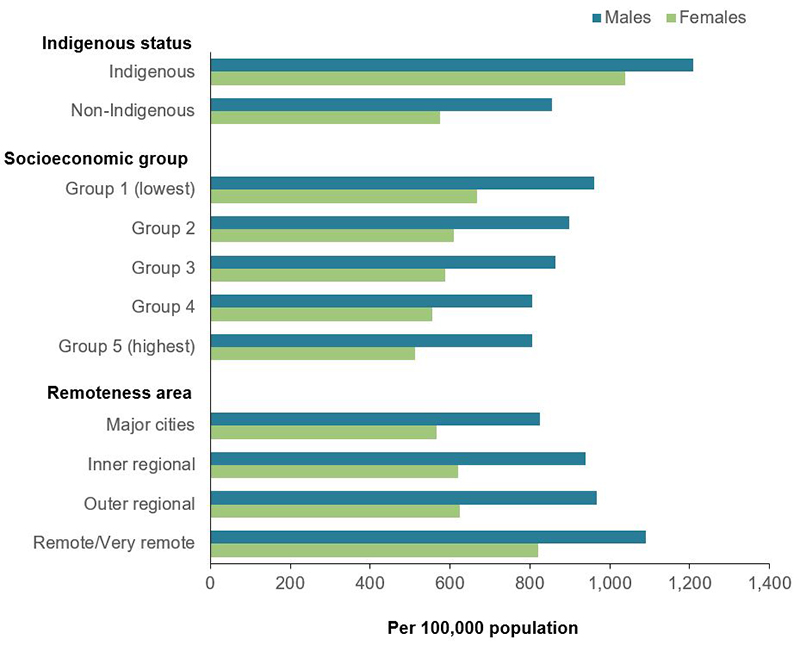
Note: Age-standardised to the 2001 Australian population.
Source: AIHW National Hospital Morbidity Database. (Data table 6)
Remoteness and socioeconomic position
In 2017–18, hospitalisation rates where AF was the principal or additional diagnosis were:
- 1.2 times as high in the lowest socioeconomic group compared with the highest socioeconomic group, based on area of usual residence (809 and 652 per 100,000 population)
- 1.4 times as high in Remote and very remote areas compared with Major cities (965 and 690 per 100,000 population) (Figure 5).
These patterns suggest that individual risk factors and social determinants, along with health service system factors such as recognition and diagnosis of AF, and access to elective investigation and management influence variation in hospitalisation rates among population groups (ACSQHC 2017; Katzenellenbogen et al. 2015).
A study using Western Australian data showed that Indigenous Australians with a first-time hospitalisation for AF were more likely to be younger and female than non-Indigenous Australians with a first-time hospitalisation for AF. Many of the CVD conditions associated with AF in the study had substantially higher incidence rates among Indigenous Australians, with differences in rates being much higher at younger ages and among women (Katzenellenbogen et al. 2015).
Primary Health Networks
The age-standardised rate of hospitalisation for AF as a principal or additional diagnosis was 2.6 times as high in the PHN region with the highest rate (Northern Territory, 1,293 per 100,000 population), compared with the PHN region with the lowest rate (Australian Capital Territory, 502 per 100,000 population) (Data table 9).
References
ACSQHC (Australian Commission on Safety and Quality in Health Care) 2017. The second Australian atlas of healthcare variation. Sydney: ACSQHC.
Katzenellenbogen JM, Teng THK, Lopez D, Hung J, Knuiman MW, Sanfilippo FM et al. 2015. Initial hospitalisation for atrial fibrillation in Aboriginal and non-Aboriginal populations in Western Australia. Heart 101:712–9.