Hospital procedures for the treatment of atrial fibrillation
The hospital procedures in this report are a selection of procedures provided in hospital to admitted patients to treat AF (Data table 11).
Cardioversion
Electrical cardioversion is a therapeutic procedure which delivers a small electric shock to the heart to restore and maintain normal rhythm.
In 2017–18, there were 19,900 cardioversion procedures performed on persons with a principal diagnosis of AF, at a rate of 27 per 100 AF hospitalisations. The rate had declined during the early 2000s, but then rose to be similar to the rate in 2000–01 of 28 per 100 AF hospitalisations (Figure 6).
Cardiac ablation
Cardiac ablation is a therapeutic procedure where small areas of tissue in the heart responsible for AF are inactivated through application of heat or intense cold.
In 2017–18, there were 8,000 cardiac ablation procedures performed on persons with a principal diagnosis of AF, at a rate of 11 per 100 AF hospitalisations. This rate has increased from 0.3 per 100 AF hospitalisations in 2000–01 (Figure 6).
Figure 6: Rate of cardioversion and ablation procedures where principal diagnosis is atrial fibrillation, 2000–01 to 2017–18
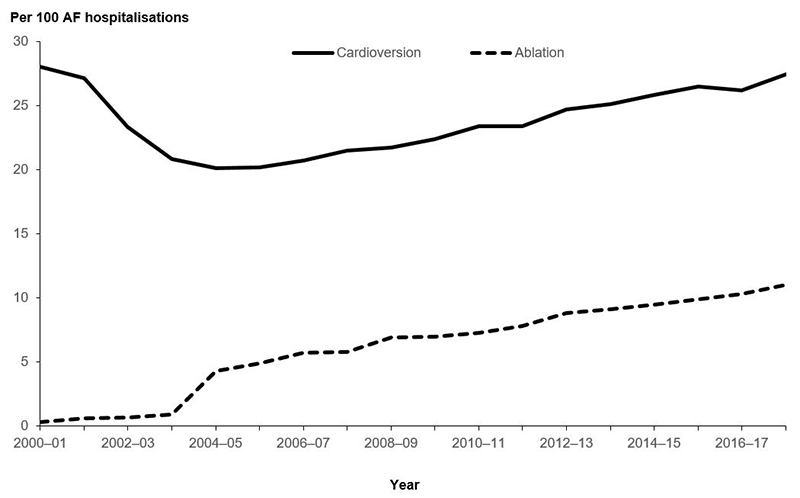
Note: Cardioversion includes Australian Classification of Health Interventions (ACHI) (10th edition) procedure code 13400-00. Cardiac ablation includes ACHI block number 601 plus procedure code 38212-01.
Source: AIHW National Hospital Morbidity Database. (Data table 12)
Population groups
Different population group patterns emerged among AF hospitalisations which included a cardioversion or ablation procedure compared with AF hospitalisations which did not (Figure 7).
In 2017–18, the proportion of AF hospitalisations that included either a cardioversion or an ablation procedure was higher for males compared with females. For males, the age-standardised rate of AF hospitalisations which included either a cardioversion or an ablation procedure was 135 per 100,000 population compared with 164 per 100,000 population for AF hospitalisations which did not. For females, the age-standardised rate of AF hospitalisations which included either a cardioversion or an ablation procedure was 57 per 100,000 population compared with 142 per 100,000 population for AF hospitalisations that did not.
Figure 7: Atrial fibrillation hospitalisation rates, principal diagnosis, with and without cardioversion or ablation procedure, by population group, 2017–18
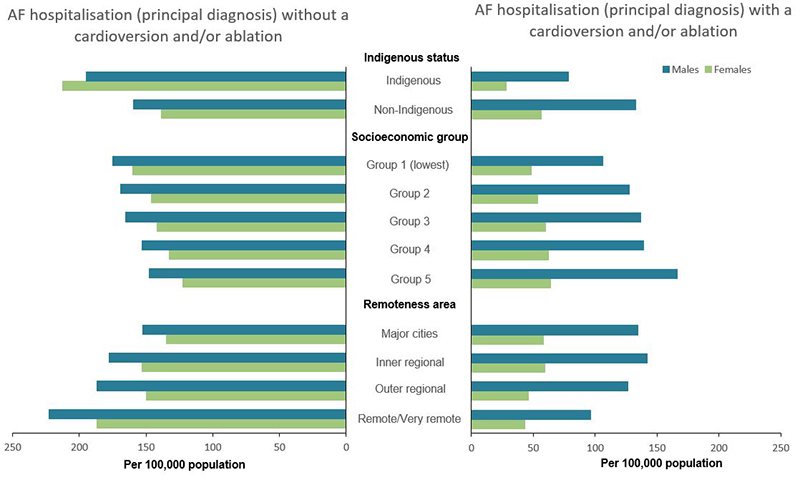
Source: AIHW National Hospital Morbidity Database. (Data table 13)
In 2017–18, there were 254 hospitalisations of Aboriginal and Torres Strait Islander people where AF was a principal diagnosis and a cardioversion or ablation procedure was performed. This represented a rate of 31 per 100,000 population. There were 888 hospitalisations of Aboriginal and Torres Strait Islander people where AF was a principal diagnosis and no cardioversion or ablation procedure was performed. This represented a rate of 108 per 100,000 population (Data table 14).
The age-standardised rates of hospitalisation with a principal diagnosis of AF and with a cardioversion or ablation procedure were:
- 1.8 times as high in non-Indigenous Australians compared with Indigenous Australians (94 and 52 per 100,000 population)
- 1.4 times as high in Inner regional areas compared with Remote and very remote areas (100 and 72 per 100,000 population)
- 1.5 times as high in the least disadvantaged group compare with the most disadvantaged group, by area (113 and 77 per 100,000 population) (Figure 7).
The reverse patterns were seen for hospitalisations with a principal diagnosis of AF which did not include a cardioversion or ablation procedure. The age-standardised rates were:
- 1.4 times as high in Remote and very remote areas compared with Major cities (206 and 145 per 100,000 population)
- 1.2 times as high in the most disadvantaged group compared with the least disadvantaged group, by area (168 and 136 per 100,000 population)
- 1.4 times as high in Indigenous Australians compared with non-Indigenous Australians (207 and 150 per 100,000 population) (Figure 7).
Multiple factors underlie the differences in AF procedure rates among population groups. Geographical disparities in services and in clinical expertise are a barrier to accessing timely treatment for a number of cardiovascular conditions including AF, most notably affecting Indigenous Australians living in remote areas (AIHW 2019a).
High rates of cardioversion and ablation in males compared with females have been observed in European AF registry data (Schnabel 2017). In Australia, females also have lower CVD procedure rates than males for coronary angiography, percutaneous coronary intervention, coronary artery bypass graft, cardiac defibrillator implant and carotid endarterectomy (AIHW 2019b).
Clinical factors such as hospital admission practices, severity of AF, presence of comorbid conditions, and socioeconomic factors such as levels of private health insurance coverage, can also affect cardiac procedure rates among population groups (AIHW 2015).