Stroke and atrial fibrillation
AF greatly increases the risk of stroke, and this risk varies with the presence of risk factors and modifiers. Avoidance of stroke is 1 of the 3 patient management focal points of the ‘Atrial fibrillation Better Care (ABC) holistic pathway: ('A' Anticoagulation/Avoid stroke; ‘B’ Better symptom management; ‘C’ Cardiovascular and Comorbidity optimization (Hindricks et al. 2020).
Stroke hospitalisation with atrial fibrillation as an additional diagnosis
In 2017–18, there were 39,053 acute hospitalisations with the principal diagnosis of stroke, and of these 6,059 (15.5%) had AF listed as an additional diagnosis. For female stroke hospitalisations, 16.5% had AF listed as an additional diagnosis and for males, 14.7%.
Between 2000–01 and 2017–18, the age-standardised rate of hospitalisation with a principal diagnosis of stroke was stable, from 169 per 100,000 population in 2000–01 to 133 per 100,000 population in 2017–18. The age-standardised rate of hospitalisation for stroke with an additional diagnosis for AF follow a similar trend, from 25 per 100,000 population in 2000–01 to 20 per 100,000 population in 2017–18 (Data table 21).
The percentage of hospitalisations for stroke in which AF was an additional diagnosis has remained relatively steady between 2000–01 and 2017–18 (Figure 14).
Figure 14: Percentage of hospitalisations for stroke, principal diagnosis, which had an additional diagnosis of AF, by sex, 2000–01 to 2017–18
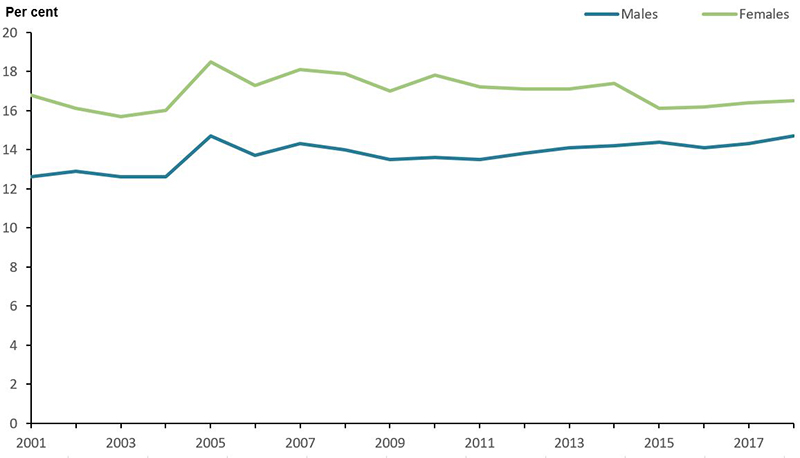
Source: AIHW National Hospital Morbidity Database. (Data table 21)
Stroke deaths with atrial fibrillation as an associated cause
In 2018, stroke was the underlying cause of 8,420 deaths—1,041 (12%) of these had AF listed as an associated cause. While more females died of stroke in 2018, (4,940 compared with 3,480 for males) the proportion of the deaths in which AF was listed as an associated cause was similar for males and females (both 12%).
Between 2001 and 2018, the age-standardised rate of stroke deaths decreased from 45 to 26 per 100,000 population. The age-standardised rate of stroke death with AF listed as an associated caused remained stable between 2001 and 2018, from 2.7 to 3.1 per 100,000 (Data table 22). The proportion of stroke death in which AF was listed as an associated cause increased over this period from 6% to 12% (Figure 15).
Figure 15: Percentage of stroke deaths, underlying cause, which had an associated cause of AF, by sex, 2000–01 to 2017–18
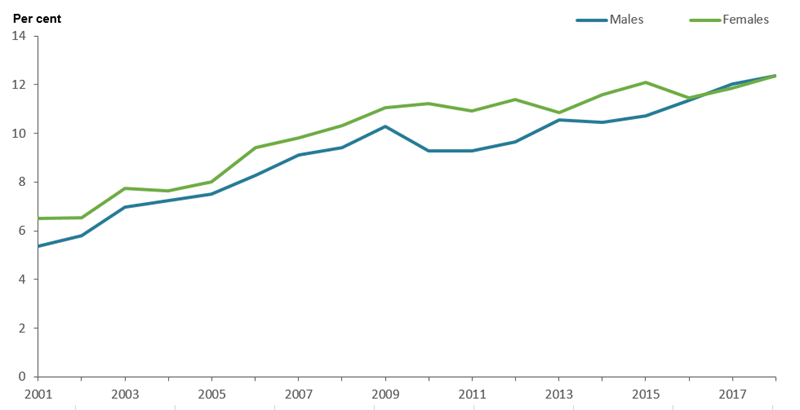
Source: AIHW National Mortality Database. (Data table 22)
References
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax J, Blomström-Lundqvist C et al. 2020. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC, European Heart Journal