Australian Bureau of Statistics (ABS) changes to mortality coding over the study period
The following information on mortality coding is sourced from the ABS. For further information, see the ABS Causes of death, Australia report (ABS 2018).
Substantial changes to ABS cause of death coding were undertaken in 2006, improving data quality by enabling the revision of cause of death for open coroner’s cases over time. Deaths that are referred to a coroner (including deaths due to suicide) can take time to be fully investigated. To account for this, all coroner-certified deaths registered after 1 January 2006 are subject to a revisions process. This allows cause of death for open coroner’s cases to be included at a later stage where the case is closed during the revision period. Cause of death data are deemed preliminary when first published, with revised and final versions of the data being historically published 12 and 24 months after initial processing. Between 2001 and 2005, revisions did not take place and as such it is recognised by the ABS that deaths by suicide may have been understated during this period (ABS 2018).
As well as the above changes, new coding guidelines were applied to deaths registered from 1 January 2007. The new guidelines improve data quality by enabling deaths to be coded as suicide by ABS mortality coders if evidence from police reports, toxicology reports, autopsy reports and coroners’ findings indicates the death was due to suicide. Previously, coding rules required a coroner to determine a death as due to suicide for it to be coded as suicide.
The combined result of both changes has been the more complete capture of deaths by suicide, and a reduced number of deaths coded as ‘undetermined intent’, within Australian mortality data. The NCIS also continually makes improvements and enhancements to their system which allows for ABS coding to be accessed in a more timely fashion.
Detailed information on coding guidelines for intentional self-harm, and administrative and system changes that can have an impact on the mortality data set, can be found in Explanatory Notes 91-100 of Causes of death, Australia report (ABS 2018).
Rates based on small numbers
Rates based on small numbers of events can fluctuate from year to year for reasons other than a true change in the underlying risk of the event.
In this report, rates are not reported when there are fewer than 5 events, as rates produced using small numbers can be sensitive to small changes in counts of deaths over time.
Suicide incidence rates
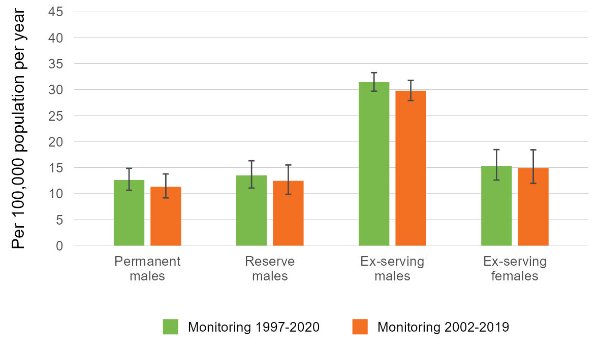
This report uses incidence rates to measure how often suicide occurs amongst the three ADF service groups, as well as in the Australian population. The incidence rate is the total number of deaths by suicide in a population over a specific period of time, divided by population time at risk during this time. In this study, the sum of the population at 30 June in each year of the relevant period is used as a proxy for population time at risk. Suicide incidence rates are expressed as the number of deaths per 100,000 population per year.
Rehires
In previous years, a complex procedure was used to identify rehires between Defence personnel (PMKeyS) data extracts, and include these individuals in the ex-serving population in the time between re-hires. This was not possible this year, so it may be that the total ex-serving population is slightly underestimated.
Potential disparity due to dates mismatch between study cohort and suicide monitoring
The study population used in this report comprises of all members with ADF service since 1 January 1985, whereas suicide rates are calculated from 1997 to 2020. This gap between the beginning of the study period (1985) and the monitoring period (1997), meaning there are suicides from the period 1985 to 1996 that are not captured in this analysis.
This approach risks introducing uncertainty, since the suicide rates before 1997 are unknown, and unable to be determined due to the data limitations. While regrettable, ultimately the study gains a lot by including this cohort.
This is not an issue for the Cox Proportional Hazards section, where the study population only includes those who separated during or after 1997 (or 2003).
Standardised mortality ratios
Age-adjusted comparisons between the suicide rate in each of the three ADF service status groups and the Australian population were calculated using Standardised Mortality Ratios (SMRs). The SMR is a widely recognised measure used to account for differences in age structures when comparing death rates between populations. This method of standardisation can be used when analysing relatively rare events, that is, where number of deaths is less than 25 for the analysed time period. The SMR is used to control for the fact that the three ADF service status groups have a younger age profile than the Australian population, and rates of suicide vary by age in both the study populations and the Australian population. The SMRs control for these differences, enabling comparisons of suicide counts between the three service status groups and Australia without the confounding effect of differences in age.
The SMR is calculated as the observed number of events (deaths by suicide) in the study population divided by the number of events that would be expected if the study population had the same age and sex specific rates as the comparison population. SMRs greater than 1.0 indicate a greater number of suicides in the ADF population than expected; and SMRs less than 1.0 indicate a lower number of suicides than expected in the ADF population.
Unlike suicide rates, SMRs only provide information about the two populations the statistic is based on. Comparing SMRs cannot be used to draw conclusions about the relative adjusted mortality rates of the study populations. This is because each SMR measure provides a comparison that is specific to the two populations involved.
Comparisons with the Australian population are not calculated for other breakdowns such as by rank and reason for separation as only adjusting for age and sex does not account for all the differences in the populations. In addition, it is considered more useful to compare between the different levels of these groups rather than with the Australian population.
Age-standardised rates
Age-standardised rates are incidence rates that enable comparisons between populations that have different age structures and over time as the age structure of the population of interest may change. This effectively removes the influence of the age structure on the summary rate—it is the overall death rate that would have prevailed in the standard population if it had experienced at each age the death rates of the population under study.
Direct standardisation was used in this report. To calculate age-standardised rates, age-specific rates were multiplied against a standard population. Directly age-standardised rates were adjusted using the current Australian standard population (that is, the non-recast Australian estimated resident population (ERP) as at 30 June 2001).
Rates are expressed as per 100,000 per population years (AIHW 2022).
Cox proportional hazards model
Survival analysis models the time it takes for an ‘event’ to occur after some ‘intervention’, termed ‘survival time’. The Cox proportional hazards regression model (Cox 1972) is the most common tool for studying the dependency of survival time on one or more predictor variables.
In this report the event measured is death by suicide, and the intervention is separation from the ADF. Each individual enters the model on their separation date, and is censored from further contribution at the point of their death (not by suicide) or on data extract date (31 December 2020) if they are alive. Calculations are then made based on the occurrences of suicide among the model population.
The ‘survival’ package in the statistical computing software R was used to fit the Cox models presented in this study (Fox 2018).
The purpose of modelling is to evaluate simultaneously the effect of multiple factors on the risk of death by suicide at a point in time. This risk is referred to as the hazard rate. The hazard ratios (HRs) that are reported in this study compare hazard rates between groups within a variable relative to a reference group.
- A HR > 1 indicates that a group is associated with a higher occurrence of suicide
- HR < 1 indicates that a group is associated with a lower occurrence of suicide
- HR = 1 suggests no effect.
If the HR 95% CI includes the value 1, then that suggests there is no strong evidence the group has an effect on the occurrence of suicide. HRs within models can be directly compared, giving rates of interactions between variables while holding all other values constant.
A key assumption of the Cox model is that the effect or hazard for each group within a variable remains proportional over time (the proportional hazards assumption). Tests for proportional hazards were performed on the models presented and, for each variable and each model, the proportional hazards assumption was supported.
Confidence Intervals
This report uses confidence intervals of 95% in the calculation of rates, SMRs and HRs. Broadly speaking wider CIs imply less certainty around a calculated value, and narrower CIs imply more certainty. Specifically, a CI at 95% suggests that repeated samples calculating the CI in the same manner would contain the true value 95% of the time.
Using confidence intervals to test for statistical significance
Statistical significance is based on a measure that indicates how likely it is that an observed difference, or a larger one, would occur under the conditions of the null hypothesis.
In this study, 95% confidence intervals (CIs) are provided for each standardised mortality ratio (SMR) and suicide rate to indicate the level of uncertainty around these estimates due to random fluctuations in the number of suicides over time. Estimates produced using low numbers can be sensitive to small changes in numbers of deaths over time and will therefore have wide CIs. CIs at 95% are provided within this report as they may account for the variation in absolute numbers of deaths by suicide over time (related to the small sample size). These assume that the suicide counts used in this analysis can be described by a Poisson distribution.
It is important to note that there are other sources of uncertainty, such as the linkage error, that are not captured by the provided CIs.
Use of CIs is the simplest way to test for significant differences between service groups and Australian comparison groups. For the purpose of this report, differences are deemed to be statistically significant if CIs do not overlap with each other (when comparing suicide rates) or 1.0 (in the case of an SMR). The CIs in this report cannot be used to determine the significance of differences between rates calculated for overlapping 3-year time periods.
Where the CIs are wide, for example in the case of the SMR for ex-serving females, sensitivity analysis was conducted. This analysis found that slight changes to the numbers of suicides did not significantly alter the result.
About the psychosocial risk factors coding work
The findings presented in the psychosocial risk factors section are from analysis of data produced as an extension of causes of death coding conducted by the Australian Bureau of Statistics (ABS) (see ABS 2021a). Mortality data and statistics are produced through collaboration of multiple jurisdictions and organisations. Registries of Births, Deaths and Marriages in each State and Territory register deaths in their respective jurisdictions and supply information about the cause of death (including from medical practitioners and coroners) to the ABS. The ABS uses this information and coronial reports sourced from the National Coronial Information System (NCIS) to review and code causes of death in each case, using the International Statistical Classification of Diseases and Related Health Problems, version 10 (ICD-10) (WHO 2019). For deaths by suicide, the ABS relies on NCIS reports, including police, toxicology, autopsy and coronial findings. The causes of death codes determined by the ABS are used in reporting on Australian mortality statistics (collated in the National Mortality Database).
The ABS code multiple causes of death to codes for individual deaths, identifying one underlying cause of death as well as associated causes of death. While the underlying cause of death is the primary cause, the associated causes of death are ‘any intervening causes, and those conditions that contributed to death but were not related to the disease or condition causing death’ (ABS 2021a). Since 2017, the ABS has expanded on the associated causes captured to include psychosocial risk factors for deaths referred to a coroner, funded by the National Suicide and Self-harm Monitoring Project (see ABS 2019; AIHW 2021a).
How is psychosocial and other risk factor coding conducted?
This report presents information on risk factors which were coded by analysts at the ABS from coronial case investigation reports contained in the National Coronial Information System (NCIS). Police, toxicology, pathology and coronial finding reports were all analysed in order to assign ICD-10 codes that represent risk factors that may have affected a person’s decision to take their own life. In addition, the ABS reviewed the underlying cause of death and injury for each ADF member and updated these if necessary.
The definition of risk factors included mental and behavioural disorders, drug and alcohol use, chronic disease, chronic pain and lifestyle factors. In addition to this the underlying cause of death and injury was reviewed for each case and updated if necessary.
|
Category
|
Description
|
ICD Chapter Reference
|
Examples
|
|
Natural Disease
|
Natural disease, as defined by the ABS, includes ‘all disease and health related conditions with the exclusion of mental and behavioural disorders, injuries, and external causes’ (ABS 2019). Excludes some terminal conditions.
Note that natural disease codes cover currently active disease and that past issues with health status and care that affected lifestyle are generally captured in psychosocial risk factors.
|
These correspond with the ICD‑10 codes A00-E90 and G00-R99, U071-U072, U08-U09. Excludes G93, J96, I46, I49, R688, R57, R58.
|
Chronic pain, insomnia, findings of drugs and alcohol in blood.
|
|
Mental and Behavioural Disorders
|
Mental and behavioural disorders, defined as ‘a clinically recognizable set of symptoms or behaviours associated in most cases with distress and with interference with personal functions’ (WHO 1992).
|
ICD-10 codes F00-F99.
|
Depression, post-traumatic stress disorder (PTSD), anxiety disorders.
|
|
Psychosocial Risk Factors
|
ABS define psychosocial risk factors ‘social processes and social structures which can have an interaction with individual thought or behaviour and health outcomes’ (ABS 2019).
|
ICD-10 codes Z00-Z99
|
Family disruption, employment status, legal issues.
|
Note that for the Australian population, the presence of natural disease risk factors was confirmed by the assessment of ICD codes present in part 2, line 6 of an individual's death certificate. This was to ensure that natural disease ICD-10 codes were indeed associated causes of death and not modes of death. It is acknowledged that the natural disease associated causes may be recorded elsewhere on a death certificate due to the space limitations if many associated causes were recorded for an individual, and therefore would not be included in this analysis. However, this affects a small number of individual records.
For further information on the methodology developed by the ABS, in consultation with stakeholders, see Psychosocial risk factors as they relate to coroner-referred deaths in Australia | Australian Bureau of Statistics (abs.gov.au) (ABS 2019).
Scope of psychosocial risk factor coding
This report presents information on psychosocial risk factors for ADF members who died by suicide between 1 January 2001 and 31 December 2020, and who had served at least one day since 1 January 1985.
The ABS used information (coronial reports) from the National Coronial Information System (NCIS) for coding associated causes of death and psychosocial risk factors. The NCIS is limited in that it only includes a nationally complete set of records from 1 January 2001 onwards, there is no centralised death information available prior to this. Therefore, the ABS coding is limited to deaths after 1 January 2001.
Mortality identifiers, also known as Mortality IDs, were used to identify ADF members who died by suicide in the NCIS. Records for 1,354 of the 1,359 ADF member deaths by suicide during the period (deaths that occurred between 1 January 2001 and 31 December 2020) were available for coding, as 5 cases did not link to a record in the NCIS. Cases may not have linked to the NCIS for several reasons, including a change in NCIS ID through time. All five cases occurred between 2001 and 2005.
The ABS piloted a project (ABS 2019) analysing information from the National Coronial Information System (NCIS) to capture psychosocial risks for deaths referred to a coroner in 2017 (ABS 2019). The ABS subsequently coded psychosocial risk factors for all Australian suicides 2017–2020 which are available for analysis in the National Mortality Database (NMD) (see also ABS 2021b).
In this report risk factors are presented for Australian male and females who died by suicide where the death was registered in 2018 (sourced from the NMD). The most recent year of data for which the causes of death data are considered ‘final’ and no longer subject to revisions was 2018. Data includes 90 deaths by suicide which were registered in Victoria in 2018 but were not supplied to the ABS until 2019 due to an issue associated with the Victorian Registry's previous processing system. The causes of death information for these cases are considered revised, not final.
Revisions of risk factor coding
As with underlying cause of death information (see above technical note), some coronial cases were open at the time that the ABS initially coded psychosocial risk factors, and further psychosocial risk factors may be identified as the coronial investigation is finalised. In the ADF member cohort there were 51 open cases that could not be coded further at this time.
For Australian deaths by suicide registered since 2017, the ABS revise the coding of causes of death (including psychosocial risk factors) 2 years after a case is opened. The revised coding of causes of death may result in an increase in the proportion of suicides with psychosocial or other risk factors. Data presented for Australian males and females in this report were for deaths registered in 2018 which are considered final and no longer revised.
Limitations in coding of risk factors
The ABS used information sourced from the National Coronial Information System (NCIS) for coding associated causes of death and psychosocial risk factors. The data available in the NCIS for coding reflects the information that was recorded during the coronial investigation of deaths referred to a coroner. The information available for each case of suicide varies depending on the comprehensiveness of the information collected during the investigation. Australian jurisdictions are governed by different Coronial Acts and ‘there will be differences in the processes, type and comprehensiveness of data collection’ between different States and Territories (NCIS n.d.).
To consider a factor as an associated risk to a suicide the information must first be reported as part of the investigative process into death. Secondly for the ABS to include that information as in the ICD-10 coded datasets that information must be made available on the NCIS (ABS 2019; 2021). The coding of risk factors ‘does not necessarily reflect all causes associated with all suicides that have occurred’ (ABS 2021b)
The coded data for ADF members produced by the ABS for the current study will differ from that which is nationally available. Coding of associated causes of death (including psychosocial risk factors) for Australian males and females who died by suicide undergoes a final revision 2 years after the death was registered and is not updated further. For ADF members who died by suicide in the study scope, coding in this study was based on the most updated information recorded in the NCIS regardless of whether the death had been registered more than 2 years previously. The data produced from this project should not be directly compared with other outputs that have used only the National Mortality Database (NMD). Additionally, a specific code was used for the ADF member cohort in the current study (see below).
ADF member specific risk factors
For the purposes of this project, the ABS used a specific code to record ‘defence force related deployment’ as a risk factor in psychosocial coding. The ABS has used the code Z65.9 which is allocated as ‘Problem related to unspecified psychosocial circumstances’ in the ICD-10. The Defence force related deployment code is not used in the coding of psychosocial risk factors for suicides among the Australian population. The code ‘exposure to disaster, war and other hostilities’ in the ICD-10 is used to code risk factors for both the ADF member and the Australian cohorts to capture exposure to military operations. Where both codes are captured for the same ADF member, this indicates the defence related deployment in warlike circumstances. In the report, these codes are captured in the group ‘other problems related to psychosocial circumstances’ (Z655-Z659).