Department of Veterans’ Affairs clients
This time series line graph shows the yearly proportions of ex-serving males and females who were a DVA client or recent interaction DVA client over time from 2002 to 2021.

The proportion of ex-serving ADF members who had only made claims that had not been accepted by DVA decreased from 2.2% in 2002 to 1.2% in 2021 among males and from 1.7% in 2002 to 1.2% in 2021 among females.
The proportion of ex-serving ADF members who had served at least one day since 1985, who were cardholders has increased since 2002 5:
- Veteran White Card holders rose from 11% to 27% in 2021 for ex-serving males and 4.6% to 25% for ex-serving females
- Veteran Gold Card holders rose from 4.3% to 11% in 2021 for ex-serving males, and from 0.7% to 3.8% for ex-serving females
Among ADF members who were permanent or reserve at 31 December 2021, 67% of females and males had a Veteran White Card, and 1.3% of females and males had a Veteran Gold Card.
The proportion of ex-serving ADF members who were Veteran Orange Card holders is not presented due to small numbers (see Supplementary table S9.1). For more information and definitions of the DVA client cardholder types, see Technical notes.
DVA clients who died by suicide
This section presents suicide rates, numbers and proportions of deaths by suicide between 2002 and 2021 broken down by the DVA client status (DVA client and DVA recent interaction client).
It is important to note that ADF members who are eligible for DVA support – and who access services funded by DVA – are more likely to have physical and mental health needs that would have led them to DVA. In particular, at 31 December 2021, 93% of the involuntary medical separation cohort was a DVA client compared with 39% of the voluntary separation cohort. The key findings of this report show that the involuntary medical separation group have a higher rate of suicide. These data importantly suggest that DVA support is appropriately provided to this group.
The number and proportion of DVA clients who died by suicide can be found in Table 11. While reading these data it should be remembered that, for the purposes of this report, all recent interaction clients are also part of the DVA client group.
DVA client category | Number of males who died by suicide | % of ex-serving ADF males who died by suicide | Number of females who died by suicide | % of ex-serving ADF females who died by suicide |
|---|---|---|---|---|
DVA client(b) | 306 | 29.1% | 25 | 24.8% |
DVA recent interaction client(c) | 197 | 18.7% | 16 | 15.8% |
Non-DVA client | 747 | 70.9% | 76 | 75.2% |
Total suicides | 1,053 | 100% | 101 | 100% |
Notes
a. Note that the Total suicides numbers do not agree with Table 1 because this count runs from 2002-2021 rather than 1997-2021.
b. Includes ex-serving members who met one of the following conditions: had a White or Gold card or received a health service or support service (National Treatment Account or MBS or Hospital separation or ED attendance) or received an income or other payment or had at least one accepted claim. See Technical notes: DVA client definitions for more information.
c. Includes ex-serving members who met one of the following conditions: received a health service or support service through DVA (National Treatment Account or MBS or Hospital separation or Emergency Department (ED) attendance) or received an income payment from DVA in the past 2 years. See Technical notes: DVA client definitions for more information.
Source: AIHW analysis of PMKeyS–NDI–DVA, 1985−2021.
Among permanent and reserve male ADF members who died by suicide, 41% were DVA clients. Among permanent and reserve male ADF members who died by suicide, 16% were recent interaction clients indicating they were in receipt of DVA funded health care or income support in the two years prior to death. DVA clients and recent interaction clients include cases where interactions only occurred after death, for example where compensation has been provided after the death of an ADF member.
Among a small proportion of ADF members who died by suicide, the only interaction recorded with DVA was claims that had not been accepted – 3.9% of permanent and reserve ADF males who died by suicide had only made claims that had not been accepted, and 3.4% of ex-serving ADF males who died by suicide had only made claims that had not been accepted. Non-liability health care and other services such as employment support may still be provided to ADF members without accepted claims.
Of the ADF members who died by suicide between 2003 and 2021 6,
- 65 were males who separated for involuntary medical reasons and were also DVA clients (81% of all suicide deaths among males who separated for involuntary medical reasons)
- 32 were males who separated for other involuntary reasons and were also DVA clients (29% of all suicide deaths among males who separated for other involuntary reasons)
- 25 were males who separated voluntarily and were also DVA clients (30% of all suicide deaths among males who separated voluntarily).
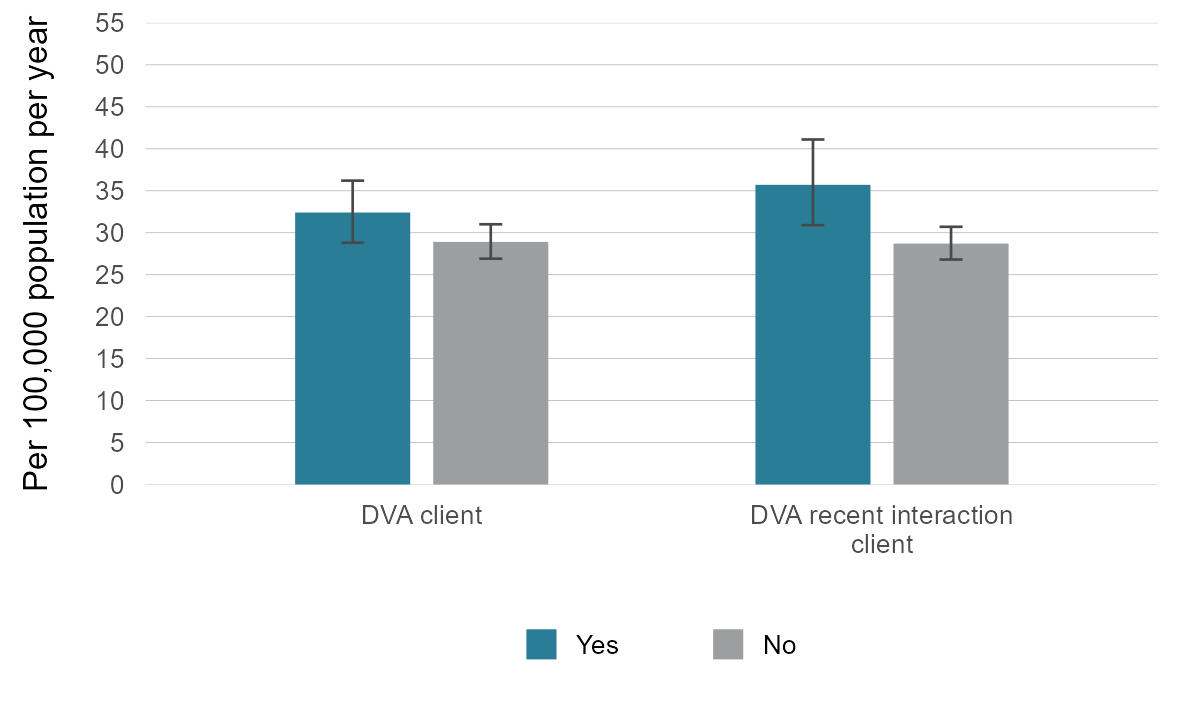
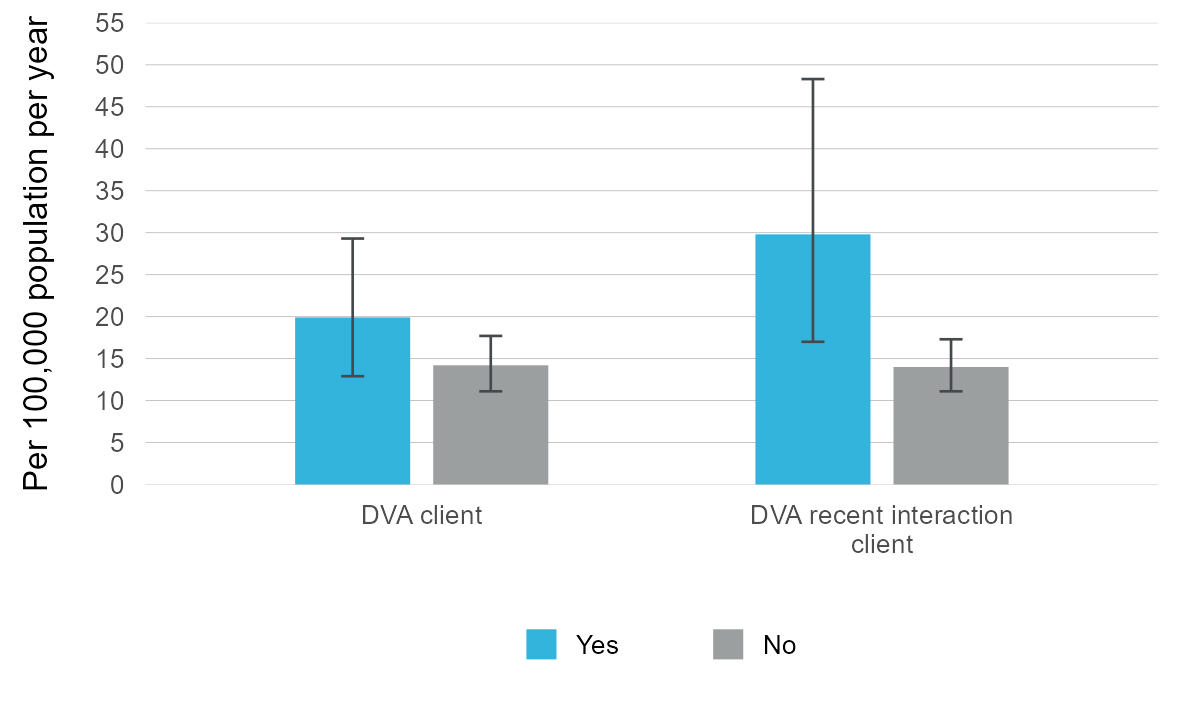
The suicide rates for the DVA client groups and all other ex-serving members are in Table 12 below. As Figures 18 and 19 show, none of these differences are statistically significant, and do not demonstrate a difference between the two groups, largely due to low numbers especially among the female ex-serving cohort.
DVA client category | Ex-serving males: Suicide rate per 100,000 population per year | Ex-serving females: Suicide rate per 100,000 population per year |
|---|---|---|
DVA client |
|
|
Yes | 32.4 | 19.9 |
No(a) | 28.9 | 14.2 |
DVA recent-interaction client |
|
|
Yes | 35.7 | 29.8* |
No(b) | 28.7 | 14.0 |
a. This group is composed of every member of the ex-serving cohort that is not a DVA client.
b. This group is composed of every member of the ex-serving cohort that is not a DVA recent interaction client. DVA clients with no recent interaction are a part of this group.
* Suicide rates in this Table denoted with a '*' should be interpreted with caution as the number of suicides is fewer than 20. These rates are considered potentially volatile.
Source: AIHW analysis of PMKeyS–NDI–DVA, 1985−2021.
Figure 18: Rate of suicide among ex-serving males who were DVA clients and non-DVA clients, 2002 to 2021
Notes:
a. DVA recent interaction clients are a subset of DVA clients. Therefore, comparisons for statistical significance of the suicide rate between DVA clients and DVA recent interaction clients should not be made.
b. Ex-serving members who are non-DVA recent interaction clients include those who are not DVA clients and DVA clients who are not DVA recent interaction clients.
c. This Figure shows that the differences in the rate of suicide between DVA clients and non DVA clients, and between DVA recent interaction clients and non DVA recent interaction clients, were not statistically significant.
Source: AIHW analysis of PMKeyS–NDI–DVA, 1985−2021.
Figure 19: Rate of suicide among ex-serving females who were DVA clients and non-DVA clients, 2002 to 2021
Notes:
a. DVA recent interaction clients are a subset of DVA clients. Therefore, comparisons for statistical significance of the suicide rate between DVA clients and DVA recent interaction clients should not be made.
b. Ex-serving members who are non-DVA recent interaction clients include those who are not DVA clients and DVA clients who are not DVA recent interaction clients.
c. This Figure shows that the differences in the rate of suicide between DVA clients and non DVA clients, and between DVA recent interaction clients and non DVA recent interaction clients, were not statistically significant.
Source: AIHW analysis of PMKeyS–NDI–DVA, 1985−2021.
Data underlying this section are available in Supplementary tables S9.8 and S9.9. These Tables include suicide rates among ex-serving ADF members by DVA client status and service-related characteristics including separation reason.
Continued research into the 2 DVA client groups, incorporating additional factors such as health conditions related to claims made to DVA, may provide further insight into the health and wellbeing outcomes for ex-serving ADF members.
Help or support
If you need help or support, please contact:
- Open Arms – Veterans and Families Counselling – Phone: 1800 011 046
- Open Arms Suicide Intervention
- Defence All-hours Support Line (ASL) – Phone: 1800 628 036
- Defence Member and Family Helpline – Phone: 1800 624 608
- Defence Chaplaincy Support
- ADF Mental Health Services
- Lifeline – Phone: 13 11 14
- Suicide Call Back Service – Phone: 1300 659 467
- Beyond Blue Support Service – Phone: 1300 22 4636
For information on support provided by DVA, see: