Technical notes
Changes to previously published suicide information
An additional 78 suicide deaths are reported here compared with the 2022 report. The breakdown of changes in the number of suicide deaths reported is as follows:
- 69 suicide deaths that occurred in 2021
- 9 additional suicide deaths identified in 2020 (and/or 2019) due to a lag in reporting cause of death
- 7 additional suicide deaths identified in 2007 (1), 2012 (2), 2013 (1), 2015 (3) due to newly identified linkages
- 7 fewer deaths in 2011 (2), 2014 (2), 2016 (2), 2019 (1) due to updates in cause of death information in the NDI
As well as the expansion of the suicide monitoring period and addition of a new year of cause of death data, there are 3 main reasons for changes to previously published suicide results, as described below.
Lag in cause of death information
Analysis in this study is based on year of occurrence of death. The NDI is the source of information on fact of death in this study. Fact of death information from the NDI is supplemented with cause of death information from the National Mortality Database (NMD). Analysis of the NMD for all Australian deaths shows that between 4% and 7% of deaths are not registered until the next year (ABS 2018). These deaths are not captured in cause of death information, until data for the next year become available, and so there is usually a small number of suicides in each report that should have been the year prior’s data but were only confirmed after publication.
Cause of death data revisions (ABS)
Cause of death information for the Serving and ex-serving Australian Defence Force members who have served since 1985: detailed analysis from 1997 to 2021 release is based on final cause of death information for the years 2001 to 2019. Revised data are used for 2020 and preliminary data for 2021. Cause of death for a small number of records linked to the 2019 (revised) and 2020 (preliminary) cause of death data may change where a death is being investigated by a coroner and more up-to-date information becomes available as a result of the ABS revisions process. This may have a small effect on the number of deaths attributed to suicide in these years, as some deaths currently coded as ‘undetermined intent’ could later be identified as ‘intentional self-harm’ (or vice-versa).
Although this method likely captures the vast majority of suicides, there is potential for some to be missed if coronial findings take longer than 4 years and the finding results in an update to the initial coded intent of death.
Care needs to be taken when interpreting data derived from deaths registered in Victoria. Following investigations between the ABS and the Victorian Registry of Births, Deaths and Marriages, 2,812 additional registrations from 2017, 2018 and 2019 were identified that had not previously been provided to the ABS. A time series adjustment has been applied to these deaths to enable a more accurate comparison of mortality over time. Affected deaths are presented in the year in which they were registered (that is, removed from 2020 and added to 2018 or 2019). For detailed information on this issue please refer to Technical note: Victorian additional registrations and time series adjustments in Causes of death, Australia (ABS cat. no. 3303.0) available from the ABS website.
Improvements in information available to the study
Changes to previously published results may also occur as additional information becomes available to the study.
For example, differences in data collection methods and policy around timing of death registration can affect when and how the data is recorded in the ABS collection. Data users should note the potential impact of these changes when making comparisons between reference periods. While such changes will not explain all differences between years, they are a factor that may influence the magnitude of any changes in suicide numbers as revisions are applied (ABS 2018).
Improvements in available information and linkage processes over time have also resulted in additional suicides being identified for periods previously reported on.
Australian Bureau of Statistics (ABS) changes to mortality coding over the study period
The following information on mortality coding is sourced from the ABS. For further information, see the ABS Causes of death, Australia report (ABS 2018).
Substantial changes to ABS cause of death coding were undertaken in 2006, improving data quality by enabling the revision of cause of death for open coroner’s cases over time. Deaths that are referred to a coroner (including deaths due to suicide) can take time to be fully investigated. To account for this, all coroner-certified deaths registered after 1 January 2006 are subject to a revisions process. This allows cause of death for open coroner’s cases to be included at a later stage where the case is closed during the revision period. Cause of death data are deemed preliminary when first published, with revised and final versions of the data being historically published 12 and 24 months after initial processing. Between 2001 and 2005, revisions did not take place and as such it is recognised by the ABS that deaths by suicide may have been understated during this period (ABS 2018).
As well as the above changes, new coding guidelines were applied to deaths registered from 1 January 2007. The new guidelines improve data quality by enabling deaths to be coded as suicide by ABS mortality coders if evidence from police reports, toxicology reports, autopsy reports and coroners’ findings indicates the death was due to suicide. Previously, coding rules required a coroner to determine a death as due to suicide for it to be coded as suicide.
The combined result of both changes has been the more complete capture of deaths by suicide, and a reduced number of deaths coded as ‘undetermined intent’, within Australian mortality data. The National Coronial Information System (NCIS) also continually makes improvements and enhancements to their system which allows for ABS coding to be accessed in a more timely fashion.
Detailed information on coding guidelines for intentional self-harm, and administrative and system changes that can have an impact on the mortality data set, can be found in Explanatory Notes 91-100 of Causes of death, Australia report (ABS 2018).
Suicide incidence rates
This report uses incidence rates to measure how often suicide occurs amongst the 3 ADF service groups, as well as in the Australian population. The incidence rate is the total number of deaths by suicide in a population over a specific period of time, divided by population time at risk during this time. In this study, the sum of the population at 30 June in each year of the relevant period is used as a proxy for population time at risk. Suicide incidence rates are expressed as the number of deaths per 100,000 population per year.
Rates based on small numbers
Rates based on small numbers of events can fluctuate from year to year for reasons other than a true change in the underlying risk of the event.
In this report, rates are not reported when there are fewer than 5 events, as rates produced using small numbers can be sensitive to small changes in counts of deaths over time.
In this report, rates denoted with an asterisk (*) should be interpreted with caution as the number of events is fewer than 20. These rates are considered potentially volatile.
Standardised mortality ratios
Age-adjusted comparisons between the suicide rate in each of the 3 ADF service status groups and the Australian population were calculated using Standardised Mortality Ratios (SMRs). The SMR is a widely recognised measure used to account for differences in age structures when comparing death rates between populations. This method of standardisation can be used when analysing relatively rare events, that is, where number of deaths is less than 25 for the analysed time period. The SMR is used to control for the fact that the ADF service status groups have a younger age profile than the Australian population, and rates of suicide vary by age in both the study populations and the Australian population. The SMRs control for these differences, enabling comparisons of suicide counts between the service status groups and Australia without the confounding effect of differences in age.
The SMR is calculated as the observed number of events (deaths by suicide) in the study population divided by the number of events that would be expected if the study population had the same age and sex specific rates as the comparison population. SMRs greater than 1.0 indicate a greater number of suicides in the ADF population than expected; and SMRs less than 1.0 indicate a lower number of suicides than expected in the ADF population.
Unlike suicide rates, SMRs only provide information about the 2 populations the statistic is based on. Comparing SMRs cannot be used to draw conclusions about the relative adjusted mortality rates of the study populations. This is because each SMR measure provides a comparison that is specific to the 2 populations involved.
Comparisons with the Australian population are not calculated for other breakdowns such as by length of service and rank as only adjusting for age and sex does not account for all the differences in the populations. In addition, it is considered more useful to compare between the different levels of these groups rather than with the Australian population.
Confidence Intervals
This report uses confidence intervals of 95% in the calculation of rates and SMRs. Broadly speaking wider CIs imply less certainty around a calculated value, and narrower CIs imply more certainty. Specifically, a CI at 95% suggests that repeated samples calculating the CI in the same manner would contain the true value 95% of the time.
Using confidence intervals to test for statistical significance
Statistical significance is based on a measure that indicates how likely it is that an observed difference, or a larger one, would occur under the conditions of the null hypothesis.
In this study, 95% confidence intervals (CIs) are provided for each standardised mortality ratio (SMR) and suicide rate to indicate the level of uncertainty around these estimates due to random fluctuations in the number of suicides over time. Estimates produced using low numbers can be sensitive to small changes in numbers of deaths over time and will therefore have wide CIs. CIs at 95% are provided within this report as they may account for the variation in absolute numbers of deaths by suicide over time (related to the small sample size). These assume that the suicide counts used in this analysis can be described by a Poisson distribution.
It is important to note that there are other sources of uncertainty, such as the linkage error, that are not captured by the provided CIs.
Use of CIs is the simplest way to test for significant differences between service groups and Australian comparison groups. For the purpose of this report, differences are deemed to be statistically significant if CIs do not overlap with each other (when comparing suicide rates) or 1.0 (in the case of an SMR). The CIs in this report cannot be used to determine the significance of differences between rates calculated for overlapping 3-year time periods.
Where the CIs are wide, for example in the case of the SMR for ex-serving females, sensitivity analysis was conducted. This analysis found that slight changes to the numbers of suicides did not significantly alter the result.
Population and suicide monitoring period
The population used in this report includes all ADF members who have served at least one day since 1 January 1985. As of 31 December 2021, around 385,000 Australians had served at least one day in the ADF between 1 January 1985 and 31 December 2021. Of these, 368,000 were still alive, comprising 60,000 permanent, 38,700 reserve, and 269,000 ex-serving.
Box 2 above gives more information on the ADF population used in this report and how it compares to the Australian population. Last year’s report was based on ADF members with at least one day of service since 1 January 1985 who died by suicide between 1 January 1997 and 31 December 2020. The current report uses the same ADF cohort, plus the 2021 data.
For more information on the demographics of this population, see the report: Serving and ex-serving Australian Defence Force members who have served since 1985: population characteristics 2019
ADF suicide deaths in the period 1 January 1985 to 31 December 1996
This publication reports 1,677 confirmed suicide deaths that occurred between 1 January 1997 to 31 December 2021 among ADF members who have served at least one day since 1 January 1985.
There were also 330 confirmed suicide deaths discovered by analysis of the period 1 January 1985 and 31 December 1996, meaning a total of 2,007 confirmed suicide deaths that occurred between 1 January 1985 to 31 December 2021 among ADF members who have served at least one day since 1 January 1985.
Confirmed suicide deaths prior to 1997 were not included in this analysis as these are under reported compared to the suicides identified post-1997, due to the quality and completeness National Death Index (NDI) dataset, as there are gaps in identifying data in the NDI which limits the ability to link to Defence personnel data. Therefore, while we are confident that all the confirmed suicides included are true ADF member confirmed suicides, there may be more unlinked and unknown. As such any population study analysis of suicide deaths during this period would be misleading.
For completeness, the number of discovered suicides per year 1985–1996 is given below in Table 13.
Year | Permanent and Reserve | Ex-serving | Total in all ADF service groups(a) |
|---|---|---|---|
1985 | n.p. | n.p. | 13 |
1986 | n.p. | n.p. | 7 |
1987 | n.p. | n.p. | 11 |
1988 | n.p. | n.p. | 11 |
1989 | 9 | 15 | 24 |
1990 | 7 | 16 | 23 |
1991 | 11 | 17 | 28 |
1992 | 11 | 22 | 33 |
1993 | 14 | 31 | 45 |
1994 | 8 | 35 | 43 |
1995 | 9 | 39 | 48 |
1996 | 13 | 31 | 44 |
Total(b) | 112 | 218 | 330 |
n.p. Not available for publication but included in totals where applicable, unless otherwise indicated. In this case this is a result of low numbers being potentially identifying.
Notes:
a. Consists of deaths by suicide in males and females for permanent, reserve and ex-serving ADF members.
b. Suicide numbers are likely to be under-reported for this period 1985 to 1996 as there are gaps in identifying data in the National Death Index (NDI) which limits the ability to link to Defence personnel data. Therefore, while we are confident that all the confirmed suicides included are true ADF member confirmed suicides, there may be more unlinked and unknown.
Source: AIHW analysis of linked Defence historical personnel data–PMKeyS–NDI data 1985–2021.
Ex-serving ADF members with permanent service and reserve service
Ex-serving ADF members can have either served in the permanent or reserve forces, or a combination of both over their ADF service career. The level of service duties and obligations vary greatly between the two, with permanent forces expected to render higher levels of service than reserves.
For this note, ex-serving members who were at any time engaged in permanent service will be considered ‘permanent ex-serving’, even if they were engaged in reserve service before fully separating. By contrast, those who joined and served solely in a reserve capacity will be considered ‘reserve ex-serving’.
Between 1997 and 2021 the suicide rates for the ex-serving cohort were:
- 34.9 per 100,000 population per year for permanent ex-serving males
- 25.3 per 100,000 population per year for reserve ex-serving males
- 15.6 per 100,000 population per year for permanent ex-serving females
- 15.2 per 100,000 population per year for reserve ex-serving females.
These values are shows in the Figure 20 below.
Figure 20: Suicide rates for permanent ex-serving and reserve ex-serving, males and females, 1997–2021
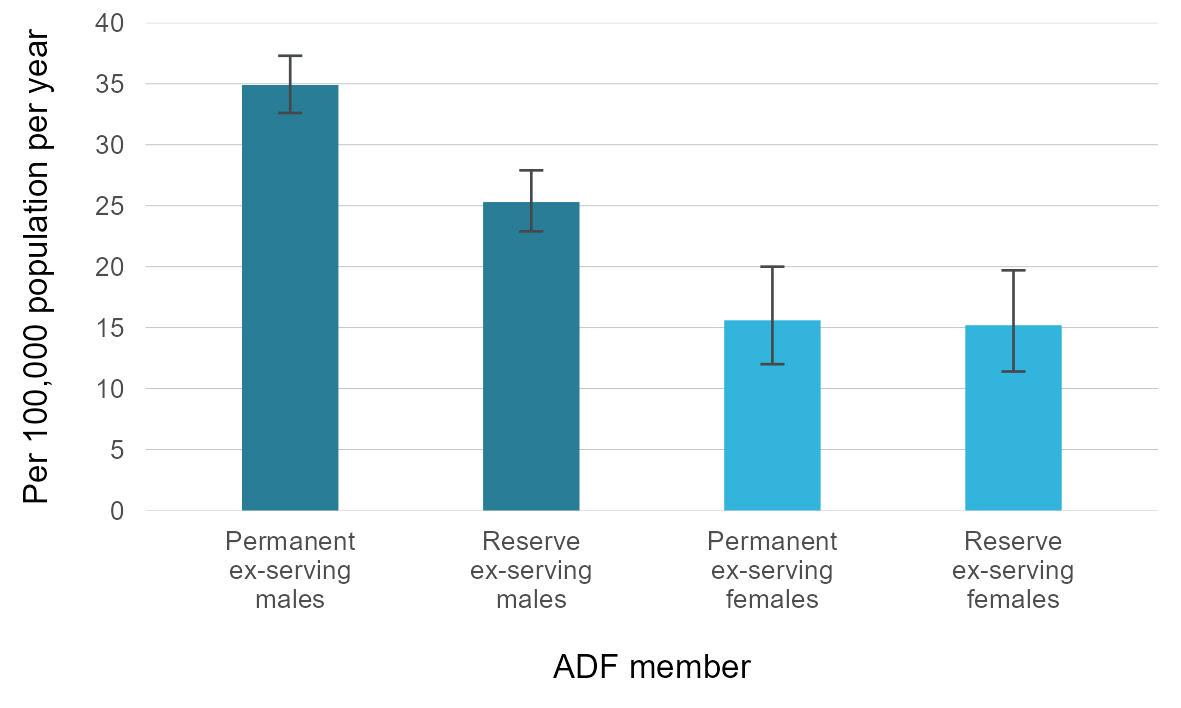
Source: AIHW analysis of linked Defence historical personnel data–PMKeyS–NDI data 1985–2021.
This Figure demonstrates that there is a higher suicide rate among permanent ex-serving males compared with reserve ex-serving males. It should be noted that most involuntary medical separations come from the permanent ex-serving cohort, which may explain this difference in rates (see the Suicides by reason for separation section). There was no corresponding statistically significant difference among the female cohorts.
While suggestive of a difference between permanent and reserve service, the decision to keep these groups aggregated statistically was made to not further limit an already small study population. As such the ex-serving cohort in this report contains all ex-serving members. For further analysis on the permanent ex-serving cohort including comparisons of suicide rates with the general Australian population and suicide rates by service-related characteristics, see Supplementary tables S8.1 to S8.3.
Data underlying this section are available in Supplementary tables S4.1 and S4.2. See Data for a link to the tables.
Other Defence Personnel factors that may be of interest
The Defence Personnel (PMKeyS) data contains other factors beyond those discussed in this report, that may be informative to analysis of ADF member suicide, notably:
- promotions and demotions
- the unit 1 a member worked within in the ADF
- the location a member lived in during their time with the ADF
- the occupation 2 a member preformed within the ADF
Preliminary analyses on these variables revealed that the frequency with which members move around the ADF makes it difficult to disentangle the effects of one specific rank change, unit, location or occupation on the ultimate suicide outcome. A more determined effort with more specialised statistical methods may yield insights into these aspects of ADF service, but for now they remain outside the scope of this analysis.
Operational experience 3 is also captured in the PMKeyS data, but the cohort of members for whom it was reliably recorded is quite small compared with the other variables considered in this report. Operational experience was only recorded with accuracy from 2001 onwards, and since we are interested in a full account of a member’s operational history that means we must confine our analyses to ex-serving members who were hired during or after 2001. This means 24% of the total 1985–2021 study cohort can be considered in these analyses. Of which only 28% have had any operational experience and among those with operational experience, 43 died by suicide. This significantly curtailed cohort of interest is the reason this calculation has proved so difficult. Univariate analysis of the suicide rates of these zero and greater than zero operational experience cohorts is unable to find any statistical differences between them.
Limitations in the study population
The study population does not include ADF members with service prior to 1 January 1985. The analysis is constrained by technical limitations in Department of Defence systems and information infrastructure for records before 1985.
Rehires
In previous years, a complex procedure was used to identify rehires between Defence personnel (PMKeyS) data extracts, and include these individuals in the ex-serving population in the time between re-hires. This was not possible this year, so it may be that the total ex-serving population is slightly underestimated.
Potential disparity due to dates mismatch between study cohort and suicide monitoring
The study population used in this report comprises of all members with ADF service since 1 January 1985, whereas suicide rates are calculated from 1997 to 2021. This gap between the beginning of the study period (1985) and the monitoring period (1997), meaning there are suicides from the period 1985 to 1996 that are not captured in this analysis.
Therefore, for the ex-serving population, there is potentially a slight bias in the suicide rate towards those who live longer (1997 onwards) for those who have served from 1985. However, the inclusion of the post-1985 cohort allows for a more complete picture of the deaths by suicide post-1997 among more of the ex-serving population. Sensitivity analysis demonstrated that the ex-serving suicide rate from 1997 to 2021 were no different when considering those who have served since 1985 compared to considering only those who have served since 1997.
Grouping of reasons for separation
The reason for separation in this report describes the main reason recorded for a person’s separating (discharging) from the ADF. Analysis by reason for separation is presented for the following groups:
- Voluntary separation: includes voluntary redundancies and resignations
- Involuntary separation: includes personnel deemed unsuitable for further duty for disciplinary, medical and operational reasons. Involuntary separation is further divided into separation for medical reasons, and non-medical involuntary separation (which includes being physically unfit for service, training failure and disciplinary reasons).
- Contractual/administration: include contractual change and/or changes in Defence personnel system (for example, transitioning of payroll system to PMKeyS introduced from 2001).
DVA client definitions
This note discusses the specific definitions used in this report for DVA client status groups.
DVA client
A DVA client under the broad definition used in this report is an ADF member who satisfies at least one of the following criteria
- has been issued a White, Orange or Gold card
- had at least one accepted claim for a health or disability condition accepted as being related to service
- has received or is receiving benefits or payments
- has received at least one health service or support service through the DVA National Treatment Account
This definition does not include ADF members who submitted claims to DVA which have not been accepted, and who otherwise did not meet the above criteria.
The definition of DVA client is inclusive of ADF members regardless of the date of contact with DVA, including where the only recorded accepted claim, card issue, benefit, payment or service occurred after death. For example, this definition includes cases where compensation payments are provided to family members after the death of an ADF member. The recent interaction definition of DVA client includes a small number of cases where the only recorded service, or regular income payment, has occurred after death.
Since mid-2018 permanent ADF members transitioning to civilian life are now issued a Veteran Card (White Card), which entitles them to treatment for all mental health conditions under the Non-Liability Health Care program. This policy change means that most ex-serving ADF members who have transitioned since mid-2018 will be included among DVA clients.
DVA recent interaction client
A DVA client under the ‘Recent interaction’ definition used in this report is an ADF member who meets the criteria for being a client per the broad definition above and is currently actively receiving a benefit from the department. A DVA client under recent interaction definition is an ADF member who satisfies the following
- Meets the criteria under the definition of DVA client status given above along with at least one of the following
- received benefits or payment in the form of income support or compensation that are considered to be a primary income source, in the past 2 years
- received at least one health service or support service funded through the DVA National Treatment Account in the past 2 years
An individual eligible for a primary form of income or DVA funded service they had not received in the past 2 years would not be considered a Recent interaction DVA client.
ADF members who are alive are considered a recent interaction client at a point in time if they received one of the designated payments or services in the prior 2 years. ADF members who have died are considered a recent interaction client at death if they had received one of the designated income payments or DVA funded services in the 2 years prior to death, or on or after death.
Income and payments considered a primary form of income for the purposes of the recent interaction client definition include the following:
- Incapacity Payments
- Permanent Impairment Payments
- Special Rate Disability Pension
- Disability Compensation Payment
- Service Pension – Age
- Service Pension – Invalidity
- Social Security Age Pension (where administered by DVA)
Health and support services include any DVA funded public and private hospital admissions, public hospital emergency department presentation, or MBS services, as well as other DVA services (including Allied Health, Community Nursing, Medical, Other TAS, Pharmacy, Private Hospitals Unique Items, Public Hospital Episode, Rehabilitation & Compensation, Rehabilitation Appliance Program, Transport, Veterans Home Care).
Data limitations
DVA record data was obtained from DVA with near complete DVA interactions were captured from 1 January 2000 onwards, noting that records of emergency department episodes are only available from 1 July 2015, and Compensation Scheme payments from 06 July 2004. While interactions before 1 January 2000 are less comprehensive, many interactions spanning from 1 January 1985 were still available and therefore were considered in the analyses.
DVA client cardholders
Veteran cards are provided to identify the eligibility of current and former ADF members, and their dependents for a range of benefits. These can include health care, pharmaceutical benefits and other benefits and concessions. There are several types of cards issued to DVA clients with the White card being the most common card type.
Policy changes over time have affected the types of conditions that qualify for benefit, the entitlements for benefit, and the process for submitting claims to DVA. For example, since July 2017 all current and former ADF personnel have been entitled to non‑liability health care (NHLC) for all mental health conditions. Since July 2018, all personnel separating from the ADF have been automatically issued with a DVA Veteran Card that entitles them to non-liability health care for any mental health. ADF members are considered DVA clients from the date they are issued a card.
Veteran Gold Cards
Holders of a Gold Card are entitled to DVA funding for all clinically necessary health services related to all health conditions, regardless of whether or not they were related to service (DVA, 2023).
Veteran White Cards
White Card holders are entitled to health services related only to conditions accepted as relating to service (DVA, 2023). However, cases of malignant cancer, pulmonary tuberculosis, and any mental-health condition do not have to be due to service-related causes.
From 1 July 2018, eligibility for treatment of any mental health condition expanded to include Reservists who have rendered Reserve Service Days with disaster relief service, border protection service or involvement in a serious service-related training incident. In addition, the White Card on Transition project commenced, with DVA issuing White Cards to transitioning members as they separate from the ADF.
Orange Cards
Orange Card holders are entitled to access prescription medicines, wound care items and nutritional supplements at a concession rate. Orange cards cannot be used for medical or other healthcare treatment. A Veteran Orange Card is issued to Commonwealth and allied veterans and mariners who meet all of the following
- they have qualifying service from the First World War or the Second World War
- they are aged 70 or over
- they have been resident in Australia for 10 years or more
DVA claims
For this paper purposes, a processed claim refers to
- a claim lodged for compensation relating to a health or disability condition related to service; and
- has been assessed by DVA with a decision outcome (accepted or rejected) for the claimed condition under the appropriate legislation
Accepted or Rejected Claims
Accepted processed claims include the following decision outcomes: accepted, aggravated by war service (eligible for treatment), attributable to war service (eligible for treatment), paired organs and limbs policy applied or remitted.
Rejected processed claims include the following decision outcomes: Attributable to war service – not eligible for treatment, deleted, deferred, no incapacity found, no jurisdiction, refused to deal with, rejected or suspended.
Legislative Framework for Compensation and Rehabilitation of Veterans
There are 3 main Acts that determine how DVA provide ADF members with health care and benefits. The applicable Act to cover an ADF member will depend on when they served and the type of military service they performed (DVA 2021b).
- Veterans’ Entitlements Act 1986 (VEA)
- Safety, Rehabilitation and Compensation (Defence-related Claims) Act 1988 (DRCA)
- Military Rehabilitation and Compensation Act 2004 (MRCA)
The Acts have different eligibility requirements and provide different levels of support to veterans through different claims and appeals processes. Veterans with multiple impairments may be covered under different Acts.