Chronic respiratory conditions:
Chronic obstructive pulmonary disease
Web article
Last updated:
Citation
AIHW (Australian Institute of Health and Welfare) (2026) Chronic obstructive pulmonary disease , AIHW, Australian Government, accessed 9 July 2026.
This article is part of Chronic respiratory conditions
Chronic obstructive pulmonary disease
- Chronic obstructive pulmonary disease This page
Bronchiectasis
Allergic rhinitis
-

In 2022, 4.8% (496,000) of people aged 45 and over were estimated to be living with COPD (including chronic bronchitis, emphysema and chronic airflow limitation).
Figure 1: Prevalence of COPD (ages 45 and over), 2001 to 2022
Line chart shows the prevalence of COPD among people aged 45 and over remained stable between 2001 and 2022.

Figure 2: COPD hospitalisations, age and sex (2023–24), trends over time (2014–15 to 2023–24)
Line chart shows a decrease in the crude rate of hospitalisations due to COPD between 2014–15 and 2023–24, from 290 to 255 per 100,000 population.

-

In 2024–25, the rate of ED presentations (principal diagnosis) due to COPD was higher in areas of most socioeconomic disadvantage compared with areas of least socioeconomic disadvantage (400 and 80 per 100,000 population, respectively).
Figure 3: Emergency department presentations due to COPD, age and sex (2024–25), trends over time (2018–19 to 2024–25)
Line chart shows the crude rate of ED presentations due to COPD between 2018–19 and 2024–25 remained relatively stable.

Figure 4: Burden of disease due to COPD, 2003 to 2024
Line chart shows the age-standardised rate of total disease burden due to COPD changed little between 2003 and 2024.

Understanding the contribution of COPD to direct health care expenditure helps to explain its economic impact.
In 2023–24:
- the age distribution of spending on COPD reflects the prevalence distribution, with most spending on people aged 45 and over (98%)
- over one-third (34%) of COPD spending was on those aged 70–79
- spending on COPD was higher for males ($913.0 million), compared with females ($837.7 million) (AIHW 2025b).
Where is the money spent?
Figure 5 shows the breakdown of expenditure due to COPD with the highest category being for admitted patients at public hospitals ($1.0 billion).
In 2023–24, expenditure on COPD was comprised of:
- hospital services, representing 77% ($1.4 billion) of COPD expenditure
- primary health care, representing 19% ($326.3 million) of COPD expenditure
- referred medical services, representing 4.2% ($73.6 million) of COPD expenditure.
Figure 5: COPD spending breakdown, 2023–24

Trends over time
Over the period from 2013–14 to 2023–24:
- total spending on COPD increased from around $1.0 billion to $1.8 billion (in current prices – unadjusted for inflation) (an increase of $711 million)
- after adjusting for the effects of inflation, real expenditure on COPD grew $355.9 million (constant prices) (Figure 6).
Figure 7: Deaths due to COPD, 2013 to 2023
Line chart shows the age-standardised mortality rate due to COPD as the underlying cause of death fluctuated between 19 and 25 per 100,000 population between 2013 and 2023.

Remoteness and socioeconomic areas
In 2023, after adjusting for age differences, mortality rates for COPD (as the underlying cause) were:
- higher for people living in Remote and Very remote areas compared with people living in Major cities (35 and 17 per 100,000 population, respectively)
- higher for people living in areas of most socioeconomic disadvantage compared with people living in the least disadvantaged areas (30 and 11 per 100,000 population, respectively).
The same patterns were observed for deaths with COPD recorded as either an underlying cause or associated cause of death.
Comorbidities of COPD
People living with COPD often also live with other long-term conditions, known as ‘comorbidity’. Having a comorbid chronic condition can mean that people have complex health needs and poorer overall quality of life (AIHW 2021b).
According to the NHS, in 2022, 88% (438,100) of people aged 45 and over with COPD (including chronic bronchitis, emphysema and chronic airflow limitation) also had one or more other chronic conditions (AIHW analysis of ABS 2023). Of those aged 45 and over with COPD, the top 4 comorbidities were:
- arthritis (54%)
- mental and behavioural conditions (45%)
- back problems (45%)
- asthma (42%).
For more information on chronic conditions and multimorbidity, see Multimorbidity in Australia.
First Nations people
COPD is a major cause of poor health and death for Aboriginal and Torres Strait Islander (First Nations) people.
For more information about First Nations people with respiratory conditions, see Aboriginal and Torres Strait Islander Health Performance Framework Measure 1.04 (AIHW 2025e).
How common is COPD among First Nations people?
An estimated 5.4% (12,400) of First Nations people aged 45 and over were living with COPD in 2022–23, according to self-reported data in the National Aboriginal and Torres Strait Islander Health Survey (NATSIHS) (AIHW analysis of ABS 2024a). The prevalence of COPD was similar among males and females (5.8% and 5.2%, respectively).
Data note: Trends in COPD prevalence among First Nations people
In the NATSIHS, COPD is captured as self-reported current and long-term bronchitis, emphysema or chronic airflow limitation. In the 2022–23 NATSIHS, emphysema was removed from survey prompt cards which may have contributed to a decline in estimated COPD prevalence for 2022–23. COPD prevalence estimates are therefore not directly comparable with previous NATSIHS surveys and unable to be used to report trends in COPD prevalence (ABS 2024b).
Hospitalisations among First Nations people
In 2023–24:
- there were around 6,600 hospitalisations where COPD was the principal diagnosis among First Nations people, a rate of 640 per 100,000 population
- after adjusting for differences in age, the hospitalisation rate among First Nations people was 5.8 times the rate among non-Indigenous Australians.
Emergency department presentations among First Nations people
In 2024–25:
- there were around 7,600 ED presentations where COPD was the principal diagnosis among First Nations people, with a rate of 730 per 100,000 population
- the rate of COPD ED presentations was higher among First Nations women than men (870 and 580 per 100,000 population, respectively)
- after adjusting for age differences, the rate among First Nations people was 7.3 times the rate among non-Indigenous Australians.
Burden of disease among First Nations people
In 2018, COPD was the 6th leading cause of total disease burden among First Nations people (AIHW 2022). COPD accounted for 3.4% of total disease burden (DALY), 2.7% of non-fatal burden (YLD) and 4.2% of fatal burden (YLL) for First Nations people in 2018 (AIHW 2022).
Deaths among First Nations people
In 2023:
- there were 348 deaths where COPD was recorded as the underlying cause of death among First Nations people, with a rate of 34 per 100,000 population
- after adjusting for differences in age, the rate among First Nations people was 3.1 times the rate among non-Indigenous Australians.
COPD mortality and smoking trends, 1980 to 2020
According to the 2018 Australian Burden of Disease Study, tobacco use contributed to 73% of total disability-adjusted life years (DALY) for COPD. The proportion of COPD DALY attributed to tobacco use was higher among females compared with males (79% and 66%, respectively) (AIHW 2021a).
The main risk factor for the development and progression of COPD is smoking, with smokers in the United States being 12 to 13 times more likely to die from COPD than non-smokers (U.S. Department of Health and Human Services 2014).
Improvements in COPD mortality rates tend to follow decreases in smoking rates, with a time-lag in-between due to the long latency period of COPD (smoking early in life is involved in initiating disease processes prior to the disease being diagnosed) (Laniado-Laborín 2009).
In Australia, the smoking rate of adults aged 18 and over decreased from 1980 to 2019 for both men and women, with men having consistently higher smoking rates than women (men: 41% to 14%, women: 30% to 12%) (Greenhalgh et al. 2023) (Figure 8).
For more information on the history of smoking and COPD, see Mortality from asthma and COPD in Australia (AIHW 2014).
Figure 8: COPD death rates of people aged 45 and over, 3-year moving average, and smoking rates, 1980 to 2020
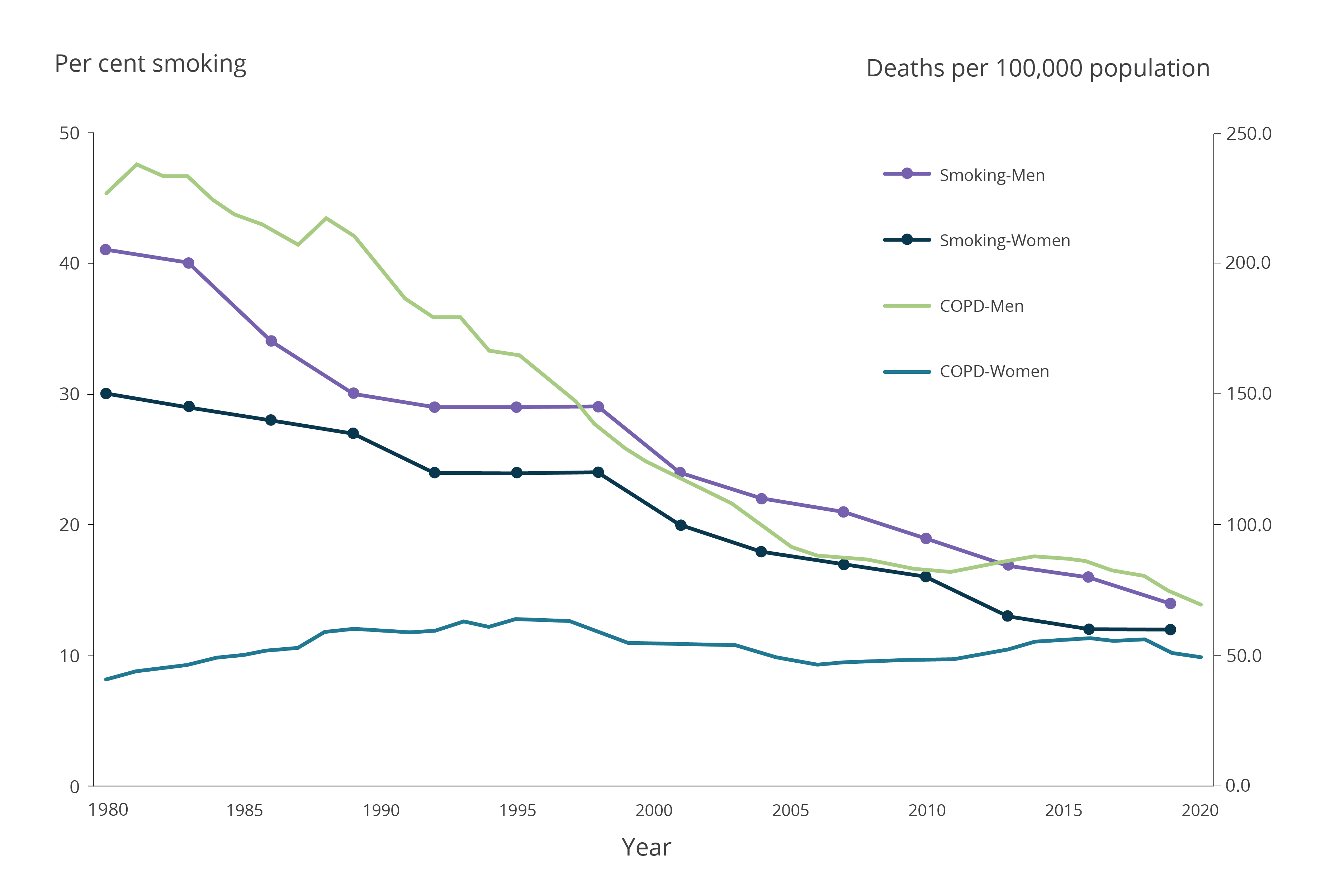
Notes:
- COPD deaths are shown as a 3-year moving average. For example, the 2020 data point represents the average of 2019, 2020 and 2021.
- From 1979 to 1996, COPD classified according to ICD-9 codes 490, 491, 492, 496. From 1997 to 2021, COPD classified according to ICD-10 codes J40–J44.
- Smoking refers to people those reporting that they smoke 'daily' or 'at least weekly', and smoking any combination of combustible cigarettes, cigars, pipes or water pipes. It does not include use of electronic cigarettes/vapes or other personal vaporising devices where users inhale vapour rather than smoke.
- Smoking data were calculated by the Cancer Council of Victoria. Smoking rates for 1980–1992 were sourced from surveys conducted by the Anti-Cancer Council of Victoria. Smoking rates for 1995–2019 were sourced from the National Drug Strategy Household Survey.
- Deaths registered in 2018 and earlier are based on the final version of cause of death data. Deaths registered in 2019 are based on the revised version and deaths registered in 2020 and 2021 are based on the preliminary version. Revised and preliminary versions are subject to further revision by the Australian Bureau of Statistics (ABS).
Source: AIHW analysis of the AIHW National Mortality Database, Greenhalgh et al. 2023.