Adolescence (13–18)
Adolescents aged 13–18 make up the oldest child developmental stage. This age group tends to be in high school or undertaking an apprenticeship, and while they are beginning to physically resemble adults, there are still significant differences in maturity and decision-making capabilities (Arain et al. 2013). Additionally, adolescents may be more likely to engage in risky behaviours, such as experimenting with drugs or alcohol, or driving recklessly, which can increase their risk of injury (CARRS 2021).
Peer pressure and the desire to fit in can also play a role in teenagers' decision-making and may lead them to take risks that they otherwise would not, in addition to increased prevalence of mental health disorders that may lead to intentional self-injury (AIHW 2021a; Tian et al. 2019).
Within this developmental stage, children are split into ages 13–15 and 16–18 for analysis due to differences in injury mechanisms. The exception to this is intentional self-harm, where due to data sensitivities, the age groups are aggregated and presented as one.
Adolescents aged 13–15
Causes
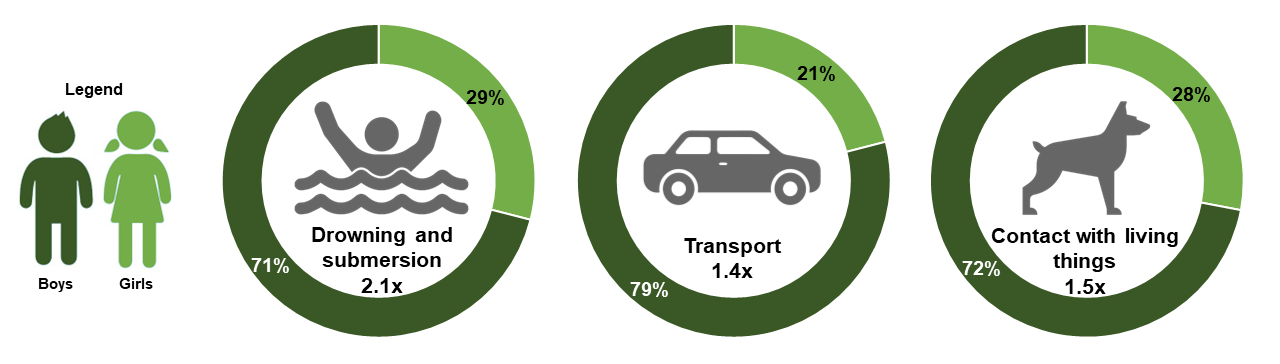
Adolescents aged 13–15 are more likely than adults to be hospitalised for injuries caused by drowning and submersion, transport, and contact with living things. For each of these causes, boys make up the majority of cases (Figure 31).
Figure 31: Injury hospitalisation rate ratios of adolescents aged 13–15 compared to adults, and sex demographic proportions, by selected external cause, Australia, 2021–22
Nature of injuries sustained
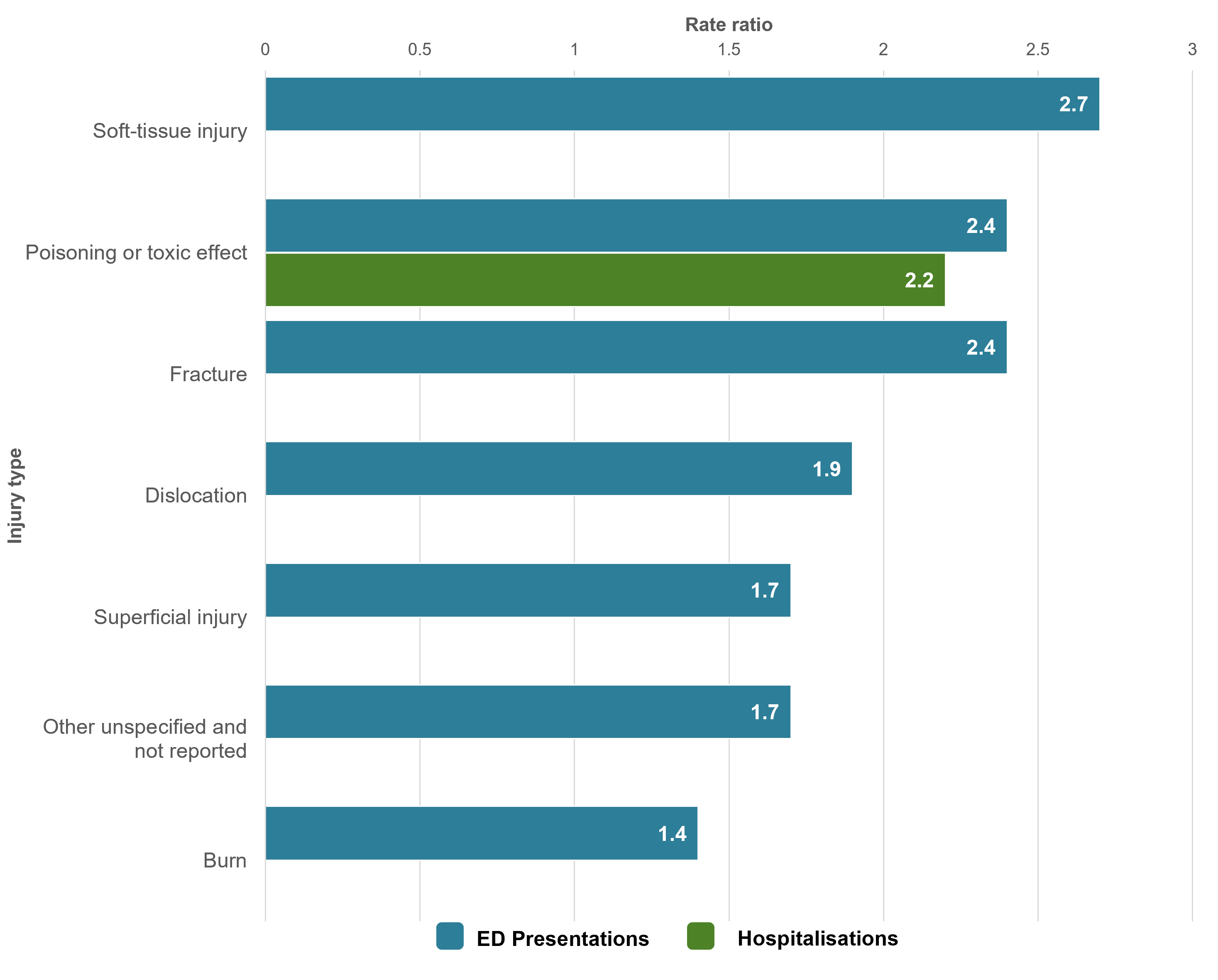
Adolescents aged 13–15 experience higher rates of injury than adults for certain injury types. This age group was 2.4 times more likely to have an ED presentation for poisoning or toxic effect, and 2.2 times more likely to be hospitalised (Figure 32).
Figure 32: Selected rate ratios of injury emergency presentations and hospitalisations among adolescents aged 13–15, by type of injury, 2021–22
Some types of injury are more prevalent in children compared to adults only in one sex. When comparing girls aged 13–15 with women, girls were more likely to have an ED presentation for a:
- foreign object (through orifice) (2.0 times)
- crushing injury (1.5 times).
This age group was also 2.2 times more likely to be hospitalised for an injury involving poisoning or toxic effect. For girls, this increases to 3.5 times (515 and 147 per 100,000 respectively).
For hospitalisations there are also differences in injury mechanism by sex:
- girls are more likely than women to be hospitalised for a crushing injury (1.7 times) or foreign object (through orifice (1.3 times)
- boys are more likely than men to be hospitalised for a fracture (1.4 times).
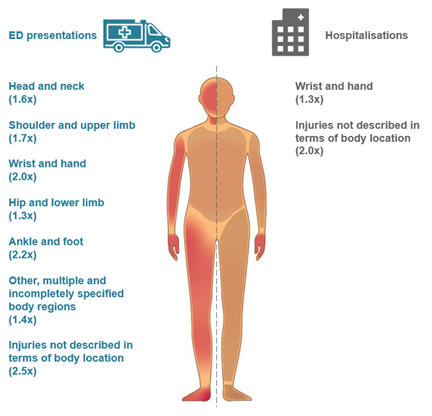
The sites of injury that adolescents aged 13–15 are more likely than adults to have an ED presentation or hospitalisation are shown in Figure 33.
Figure 33: Selected rate ratios for emergency department presentations and hospitalisations among adolescents aged 13–15, by site of injury, Australia, 2021–22
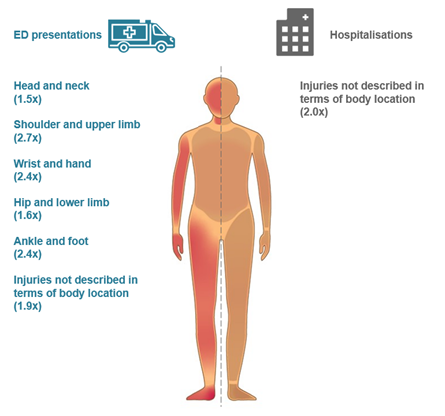
This age group was also more likely to be hospitalised for injuries not described in terms of body location (2.0 times). Boys were more likely than men to be hospitalised for injuries to the shoulder and upper limb (1.7 times).
Adolescents aged 16–18
Causes
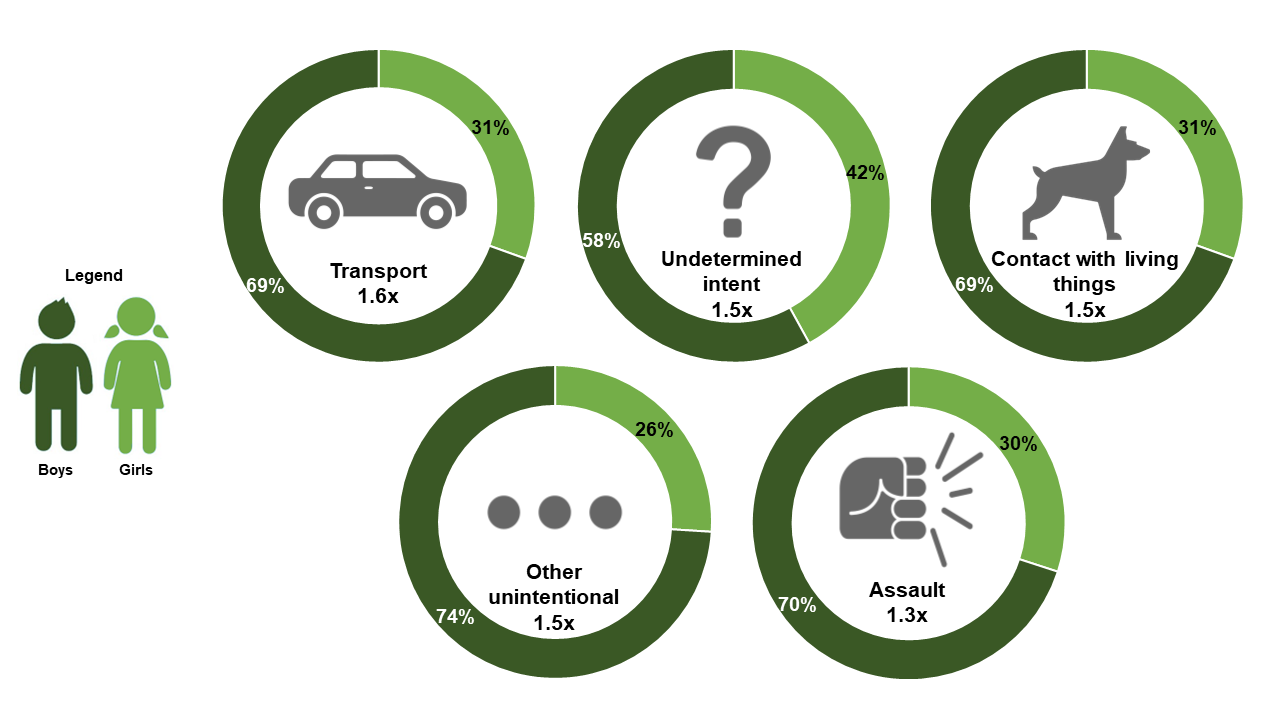
Adolescents aged 16–18 are more likely than adults to be hospitalised for injuries caused by transport, undetermined intent, contact with living things, other unintentional causes, and assault. For each of these causes, boys make up the majority of cases (Figure 34).
Figure 34. Injury hospitalisation rate ratios of adolescents aged 16–18 compared to adults, and sex demographic proportions, by selected external cause, Australia, 2021–22
Some causes of injury are more prevalent in children compared to adults only in one sex. When comparing boys aged 16–18 with men, boys were 2.1 times more likely to be hospitalised for an injury caused by drowning and submersion.
Nature of injuries sustained
Adolescents aged 16–18 experience higher rates of injury than adults for certain injury types. This age group was 3.0 times more likely to have an ED presentation for poisoning or toxic effect, and 2.9 times more likely to be hospitalised (Figure 35).
Figure 35: Selected rate ratios of injury emergency department presentations and hospitalisations among adolescents aged 16–18, by type of injury, 2021–22

Boys aged 16–18 were 1.3 times more likely than men to have an ED presentation for internal organ injuries. They were also 1.3 times more likely to be hospitalised for intracranial injuries, dislocations, and nerve injuries.
Girls aged 16–18 were more likely than women to have an ED presentation for foreign object (through orifice) injuries (2.1 times), and other specified and/or multiple injuries (1.6 times). They were also 1.4 times more likely to be hospitalised for foreign object (through orifice) injuries.
Figure 36 shows the site of injury where adolescents aged 16–18 are more likely than adults to have an injury ED presentation or hospitalisation.
Figure 36: Selected rate ratios for emergency department presentations and hospitalisations among adolescents aged 16–18, by site of injury, Australia, 2021–22
Boys are more likely than men to be hospitalised for injuries to the ankle and foot (1.4 times).
Intentional self-harm
Determining if an injury was intentional is not always straightforward, especially when children are involved. In very young children, confirming that an injury was due to intentional self‑harm can be difficult and may involve a parent or caregiver’s perception of the intent. Ability to form an intention to inflict self‑harm, and to understand the implications of doing so, requires a degree of maturity that is absent in infancy and early childhood. For this reason, statistics about hospitalisations due to intentional self-harm are presented here only for adolescents aged 13 to 18 as aggregated groups.
Note that values for intentional self-harm used in the Causes of injury chapter are for children and adolescents aged 0 to 18 inclusive, to allow for comparison between other cause groups. Consequently, there are variations in the rates presented between chapters.
For more information, see the AIHW’s reports on suicide and self-harm monitoring.
Research indicates that self-harm injuries are on the rise, and are contributing a greater proportion of injuries amongst adolescents and young adults aged 13–24 (Pollock et al. 2024). Adolescents are at a developmental stage where they are experiencing many physical, emotional, and social changes. These changes can be challenging and can contribute to feelings of stress, anxiety, and depression (Jiang et al. 2021). Adolescents may also struggle with issues related to identity, self-esteem, and relationships, which can increase their risk of engaging in self-harm or suicidal behaviours (McEvoy et al. 2023).
Additionally, adolescents may not have fully developed coping skills or support systems to help them deal with these challenges, which can make them more vulnerable to self-harm and suicide. Some population groups are at heightened risk of injury, including:
- adolescents in the youth justice and child welfare systems (Shepherd et al. 2018)
- First Nations adolescents (AIHW 2023e)
- the LGBTIQ+ community (Hill et al. 2023)
- adolescents living in rural and remote areas (Fitzpatrick et al. 2021).
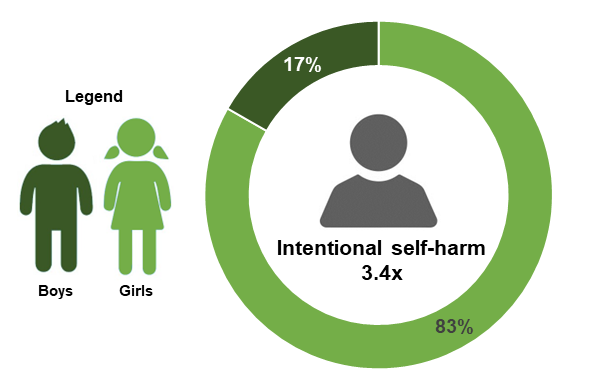
Adolescents aged 13–18 were 3.4 times more likely than adults to be hospitalised for injuries caused by intentional self-harm. Over 4 in 5 of these hospitalisations were for girls (Figure 37).
Figure 37: Injury hospitalisation rate ratios of children aged 13–18 compared to adults, and sex demographic proportions, for hospitalisations caused by intentional self-harm, Australia, 2021–22
Girls are more likely to be hospitalised for intentional self-harm than boys
Girls aged 13–18 were hospitalised for injuries caused by intentional self-harm at a rate of 582 per 100,000 population. Comparatively, boys were hospitalised at a rate of 110 per 100,000.
87% of these hospitalisations for girls involved intentional self-poisoning, compared to 76% for boys. The most common external causes of injury for each sex were:
- girls – intentional self-poisoning by and exposure to nonopioid analgesics, antipyretics and antirheumatics (45%)
- boys – intentional self-poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified (34%).
It is important to note that while females generally have higher rates of hospitalisations caused by intentional self-harm, males have higher rates of death by suicide (AIHW 2023c).