Priority populations
Some children disproportionately experience more instances of, and impacts from injuries. First Nations people, and those living in rural and remote parts of Australia have higher rates of injury hospitalisation and emergency department (ED) presentation.
Other groups of children and adolescents may also have higher rates of injury, however they cannot be identified using available hospitals data and/or corresponding population data. These groups may include and are not limited to children and adolescents:
- with siblings (Piotrowski & Warda 2021)
- with special needs such as disabilities or mental health issues (CDC 2022)
- who are culturally and linguistically diverse (CALD) (AIHW 2022c)
- that are refugees and humanitarian entrants (AIHW 2023b)
- in areas of greater socioeconomic disadvantage (AIHW 2023c)
- in the youth justice and state and territory child protection systems (Shepherd et al. 2018).
For more information about CALD populations and refugee and humanitarian entrants provided by the Australian Institute of Health and Welfare (AIHW), refer to:
The AIHW uses 'First Nations children' to refer to Aboriginal and Torres Strait Islander children in this report. Injuries are the second leading contributor to the burden of disease for First Nations people of all ages (AIHW 2022b). In 2021–22, among First Nations children:
- there were 52,100 ED presentations (14,600 per 100,000)
- there were 8,100 injury hospitalisations (2,300 per 100,000)
- boys made up the majority of ED presentations (57%) and hospitalisations (59%)
- 16–18-year-olds had the highest rate of injury ED presentations (Figure 3) and hospitalisations (Figure 4) among both boys and girls
- falls were the leading cause of injury hospitalisation (crude rate of 600 per 100,000 population).
Figure 3: Number and crude rates (per 100,000) of injury emergency department presentations among First Nations children, by age and sex, Australia, 2021–22
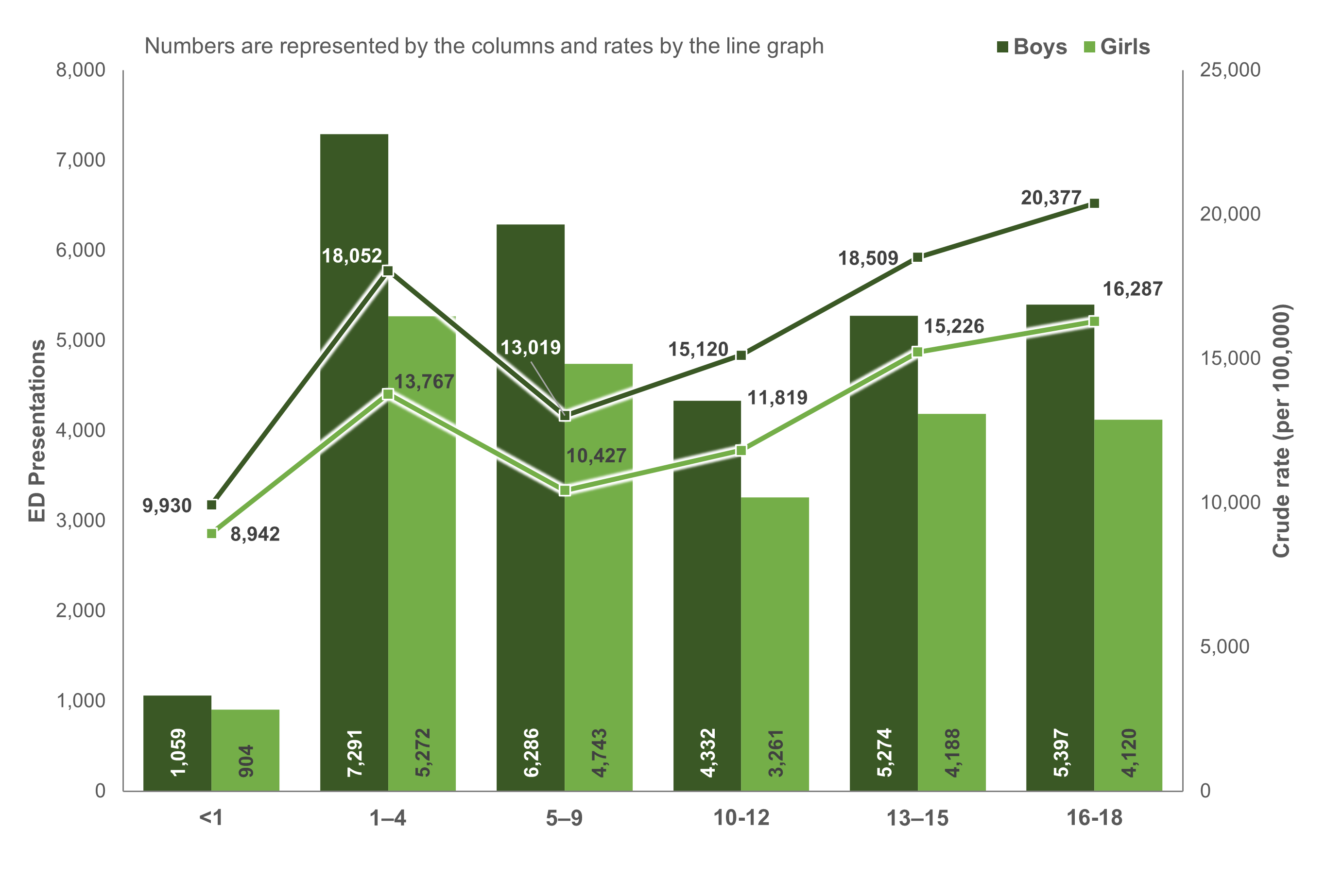
Notes:
- Numbers are represented by the columns and rates by the line graph.
- Rates are crude per 100,000 population.
- Only includes ED presentations where the patient was between 0 and 18 years of age, and where sex was not intersex, indeterminate or missing.
- Records where Indigenous status is missing or not stated are excluded.
Sources: AIHW National Non-Admitted Patient Emergency Department Care (NAAPEDC) Database and ABS Estimates and Projections, Aboriginal and Torres Strait Islander Australians.
Figure 4: Number and crude rates (per 100,000) of injury hospitalisations among First Nations children, by age and sex, Australia, 2021–22
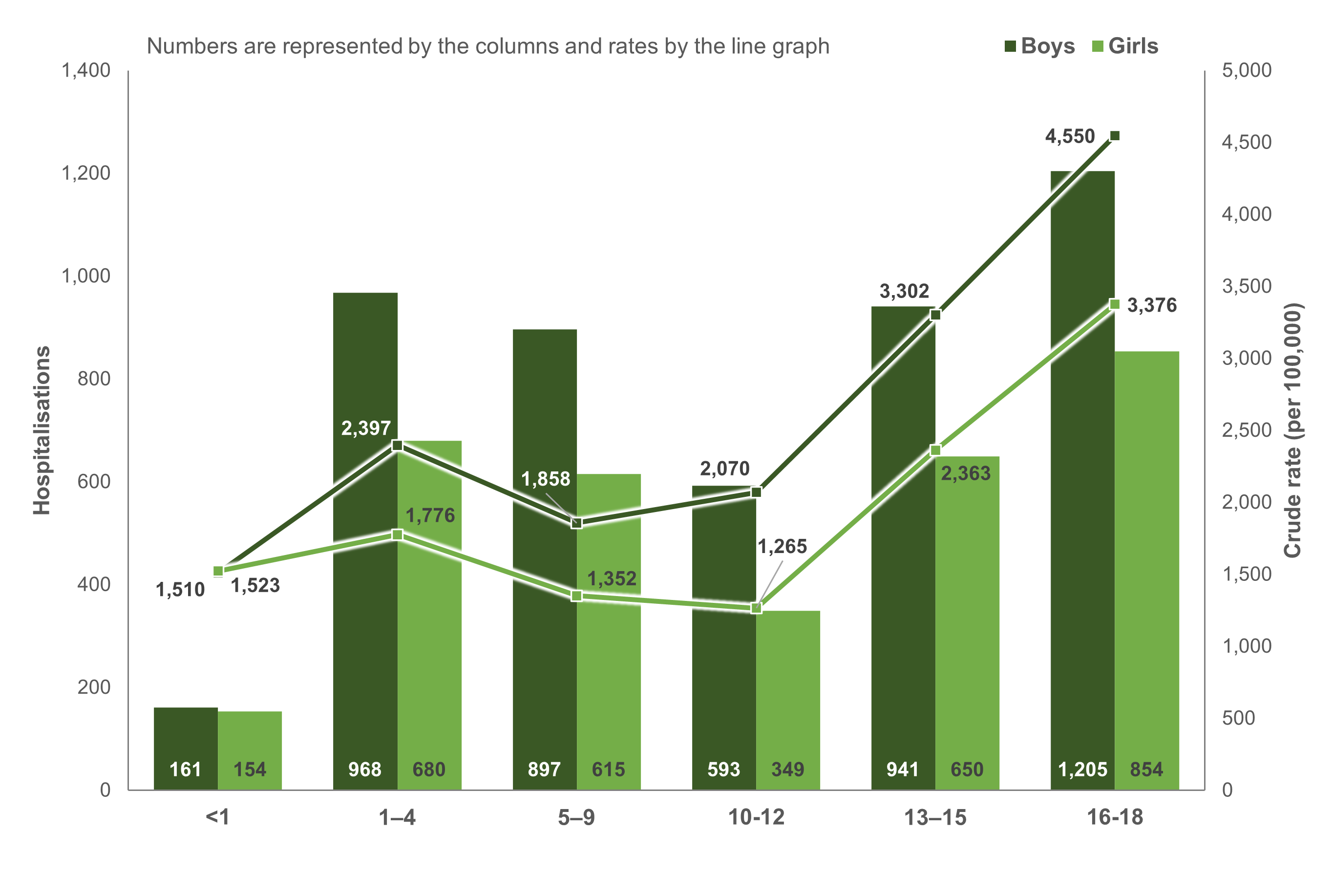
Notes:
- Numbers are represented by the columns and rates by the line graph.
- Rates are crude per 100,000 population.
- Only includes hospitalisations where the patient was between 0 and 18 years of age, and where sex was not intersex, indeterminate or missing.
- Records where Indigenous status is missing or not stated are excluded.
Sources: AIHW National Hospital Morbidity Database (NHMD) and ABS Estimates and Projections, Aboriginal and Torres Strait Islander Australians.
First Nations and non-Indigenous children
Using age-standardised rates, First Nations children are 1.5 times as likely to present to an ED and 1.6 times as likely to be hospitalised for an injury compared to non-Indigenous children (Table 1).
| Sex | First Nations ED | Non-Indigenous ED | First Nations hospitalisations | Non-Indigenous hospitalisations |
|---|---|---|---|---|
| Males | 16,277 | 11,142 | 2,645 | 1,697 |
| Females | 12,957 | 8,300 | 1,918 | 1,147 |
| Persons | 14,661 | 9,766 | 2,291 | 1,431 |
Notes:
- Rates are age-standardised per 100,000
- Only includes records where the patient was between 0 and 18 years of age
- Records where Indigenous status was missing or not stated were excluded
Sources: AIHW National Non-Admitted Patient Emergency Department Care (NNAPEDC) Database, National Hospital Morbidity Database (NHMD), ABS Estimates and Projections, Aboriginal and Torres Strait Islander Australians and ABS National, state and territory population.
Boys have the highest crude rates of injury across each age group regardless of Indigenous status, aside from infants aged under one, where rates between boys and girls are comparable.
Both population groups follow similar patterns of injury hospitalisation by age group, with the highest rates in adolescents aged 16–18 years. Figure 5 shows that First Nations adolescents aged 16–18 are hospitalised for injuries nearly twice as much as their non-Indigenous counterparts (4,000 and 2,100 per 100,000 respectively).
Among First Nations people, ED presentations mirror injury hospitalisation patterns, with the highest rates among adolescents aged 16–18, while for non-Indigenous children the highest rates are among 1–4-year-olds.
Figure 5: Crude rates (per 100,000) of injury emergency department and hospitalisation presentations among children, by age group and Indigenous status, Australia, 2021–22
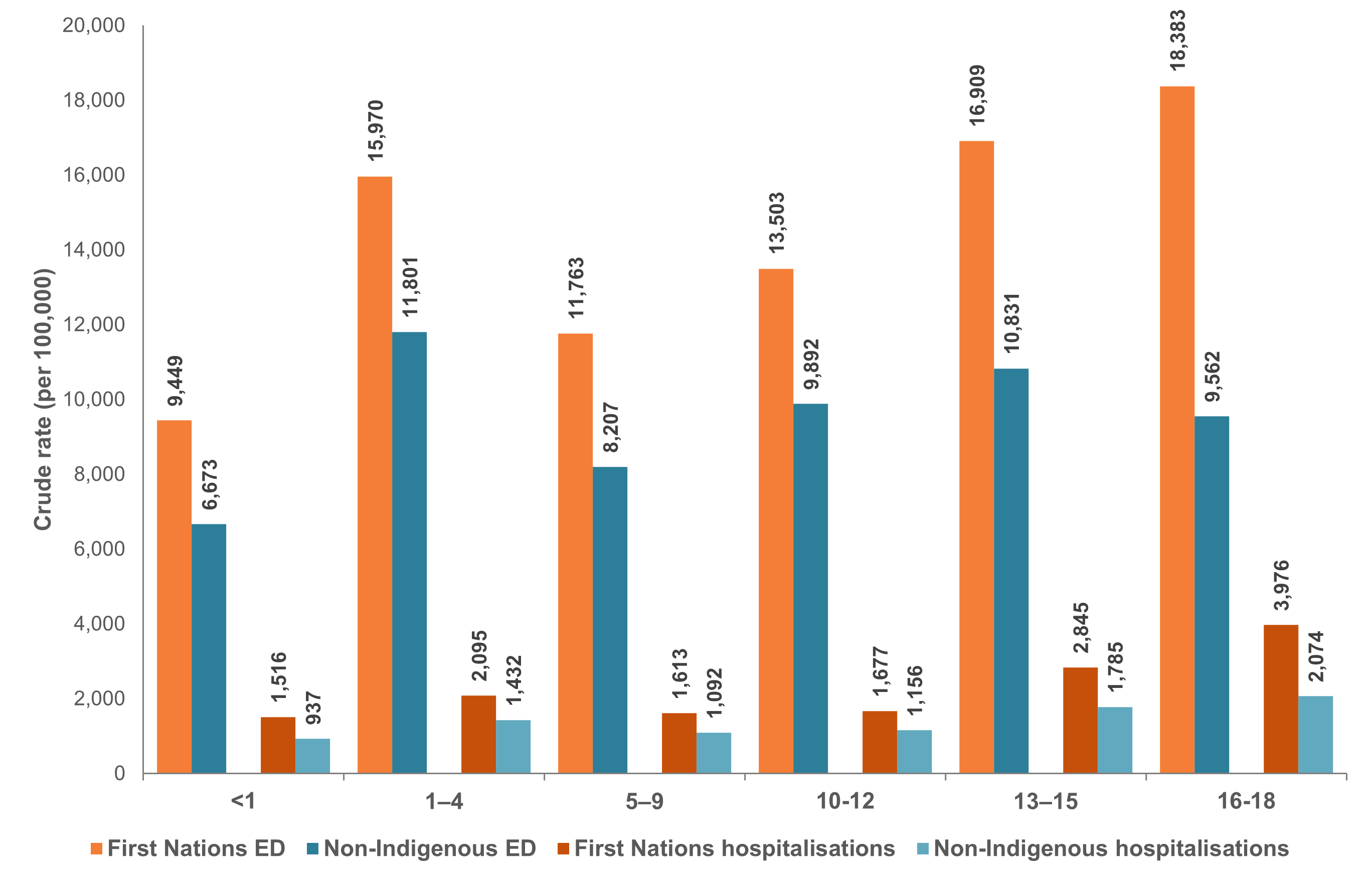
Notes:
- Rates are crude per 100,000.
- Only includes records where the patient was between 0 and 18 years of age.
- Records where Indigenous status was missing or not stated were excluded.
Sources: AIHW National Non-Admitted Patient Emergency Department Care (NNAPEDC) Database, National Hospital Morbidity Database (NHMD), ABS Estimates and Projections, Aboriginal and Torres Strait Islander Australians and ABS National, state and territory population.
The top 5 leading causes of injury hospitalisations for First Nations children include falls, contact with objects (which includes a falling or moving object, or hard or sharp object), transport, intentional self-harm, contact with living things (Figure 6).
First Nations children have higher rates of injury hospitalisation across most causes with the rate ratio of First Nations people hospitalisation compared with non-Indigenous children ranging between 1.2 and 7.
Figure 6: Age-standardised rates (per 100,000) of injury hospitalisations among children, by cause group and Indigenous status, Australia, 2021–22
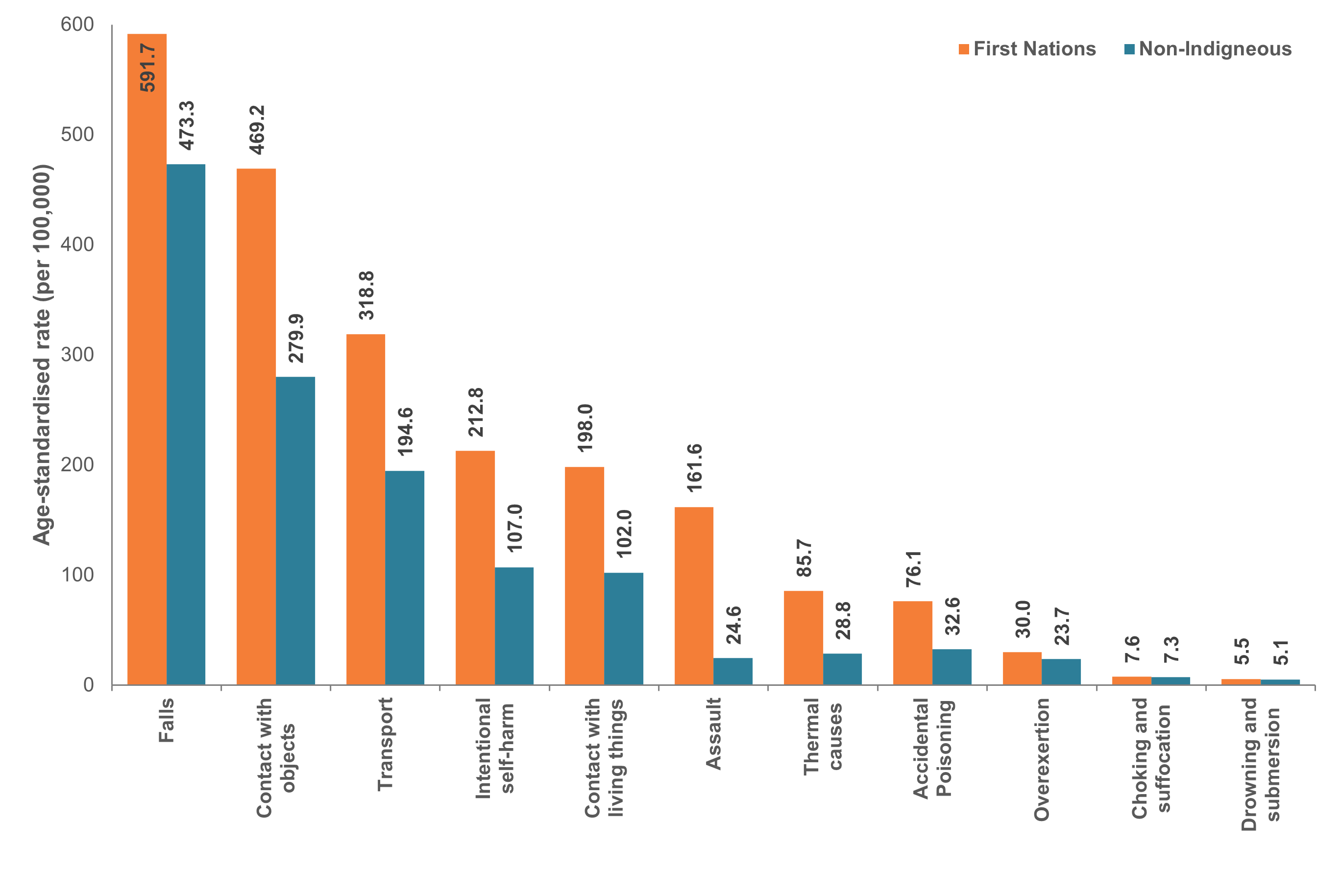
Notes:
- Rates are age-standardised per 100,000 population.
- Only includes records where the patient was between 0 and 18 years of age.
- Records where Indigenous status was missing or not stated were excluded.
- Excludes causes where rates could not be calculated due to data volatility and small numbers.
Sources: AIHW National Hospital Morbidity Database (NHMD), ABS Estimates and Projections, Aboriginal and Torres Strait Islander Australians and ABS National, state and territory population.
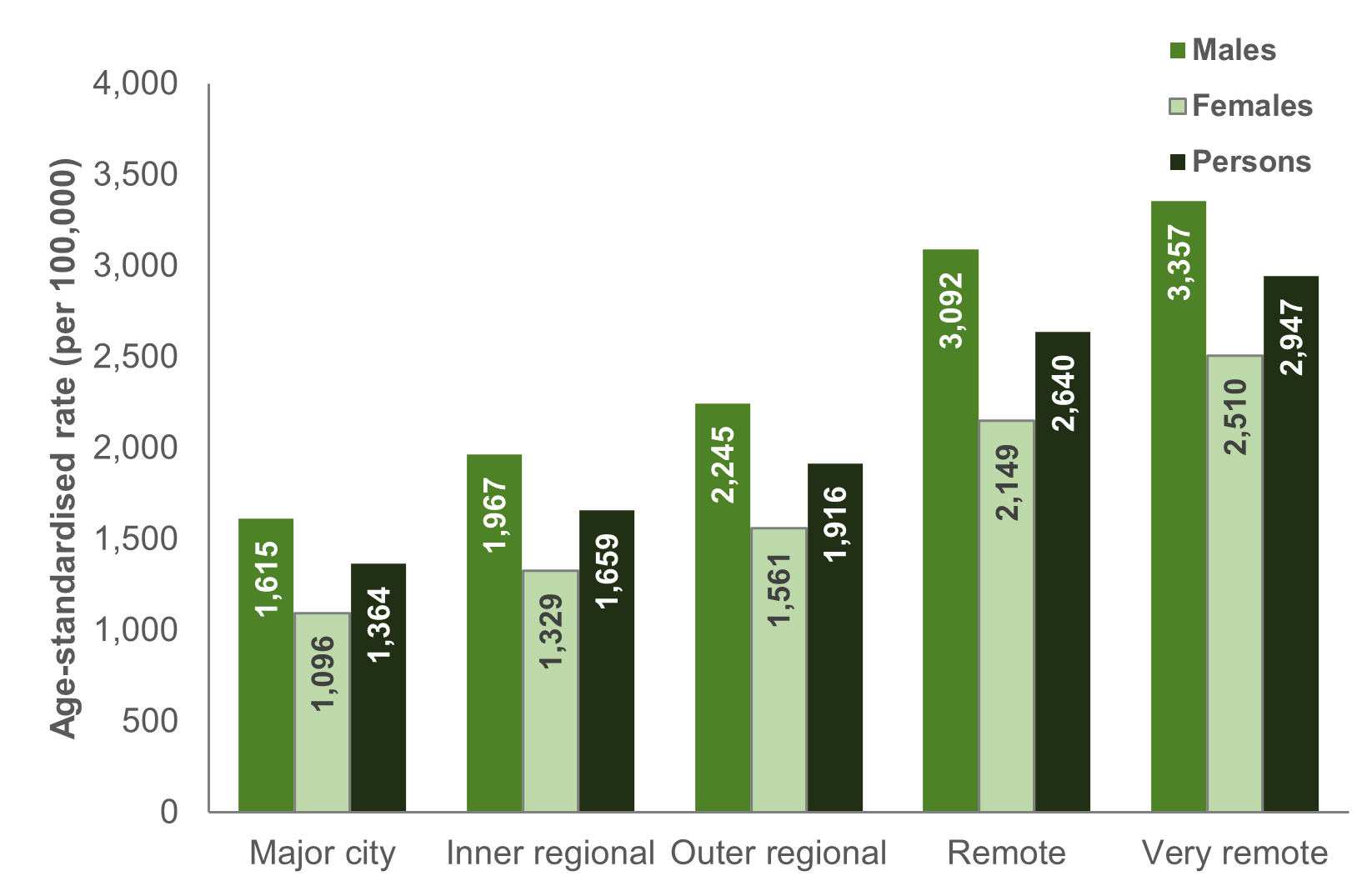
Similar to the pattern of all injuries in the general population, rates of injury hospitalisation among children increase with remoteness. Children and adolescents living in Very remote regions of Australia are over twice as likely to be hospitalised for an injury than their counterparts living in a Major city. For both boys and girls, children in Very remote regions of Australia have the highest age-standardised rates of injury hospitalisation (3,400 and 2,500 per 100,000 respectively) (Figure 7).
Most age groups follow the same pattern, excepting males aged less than 1 or 13–15, where the highest rates were in Remote regions of Australia.
Figure 7: Age-standardised rate of injury hospitalisations among children, by sex and remoteness, 2021–22
Notes:
- Rates are age-standardised per 100,000 population.
- Only includes records where the patient was between 0 and 18 years of age.
- Records where Remoteness status was missing or not stated were excluded.
Sources: AIHW National Hospital Morbidity Database (NHMD), ABS Remoteness populations.
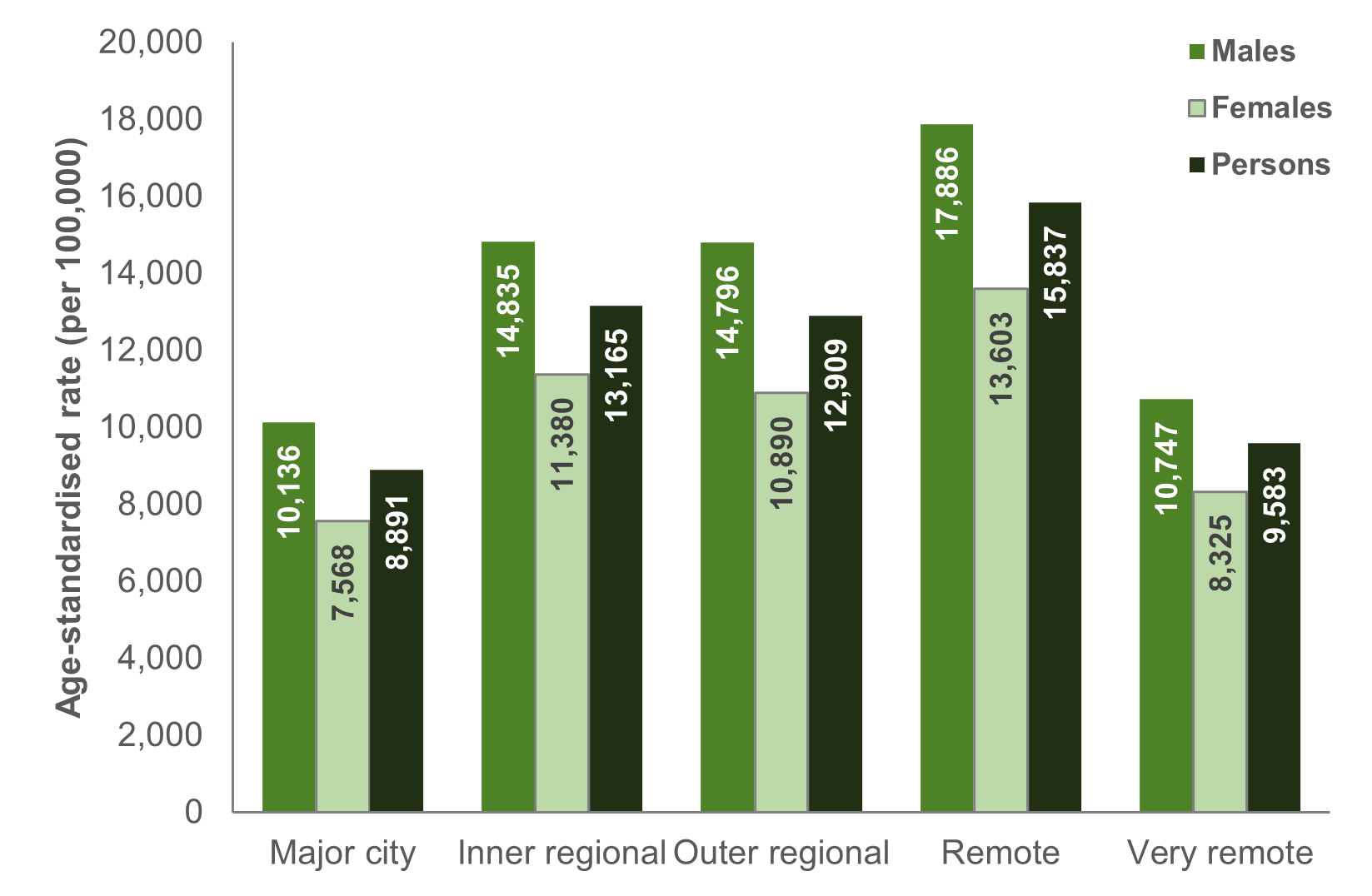
However, ED presentations do not follow this same pattern; the highest age-standardised rates were found in Remote regions of Australia, followed by Inner regional (Figure 8). The data collection only includes public hospital EDs that meet specific criteria. This may exclude smaller EDs, and underrepresent certain regional areas. For more information, see Technical notes.
Figure 8: Age-standardised rate of emergency department presentation among children, by sex and remoteness, 2021–22
Notes:
- Rates are age-standardised per 100,000 population.
- Only includes records where the patient was between 0 and 18 years of age.
- Records where Remoteness status was missing or not stated were excluded.
Sources: AIHW National Non-Admitted Patient Emergency Department Care (NNAPEDC) Database, ABS Remoteness populations.
AIHW (2022b) Australian Burden of Disease Study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018, AIHW, Australian Government, accessed 19 February 2024.
AIHW (2022c) Reporting on the health of culturally and linguistically diverse populations in Australia: An exploratory paper, AIHW, Australian Government, accessed 4 March 2024.
AIHW (2023b) Health of refugees and humanitarian entrants in Australia, AIHW, Australian Government, accessed 4 March 2024.
AIHW (2023c) Injury in Australia, AIHW, Australian Government, accessed 23 January 2024.
Piotrowski C & Warda L (2021) An investigation of risk & protective factors for school-aged child injuries: the influence of siblings, Injury Prevention, 27, doi: 10.1136/injuryprev-2021-SAVIR.71.
Shepherd S, Spivak B, Borschmann R, Kinner S & Hachtel H (2018) Correlates of self-harm and suicide attempts in justice-involved young people, PLOS ONE, 13(2), doi: 10.1371/journal.pone.0193172.