Disease specific methods - morbidity
This chapter provides information on the methods used to estimate morbidity (non-fatal burden or YLD) for each of the 17 disease groups (below, in alphabetical order). It includes information on the sequela and health states used, prevalence and severity data sources used, and details on the methods used to calculate prevalence estimates for each disease.
It also describes methods for the following conditions, which are sequela to multiple diseases (referred to as envelopes), within these disease group sections:
- anaemia – blood & metabolic disorders
- heart failure – cardiovascular conditions
- infertility – reproductive & maternal conditions
- intellectual disability – mental & substance use disorders
- vision loss – hearing & vision disorders.
Detailed information is provided on the methods used for 2018 national estimates. Where these methods differ for sub-national estimates, 2015, 2011 or 2003 estimates, this is described separately.
Sequelae and health states
Sequelae and health states assigned to blood & metabolic disorders are shown in the table below. Assumptions are outlined in subsections for individual diseases.
Table 4.5: Sequelae and health states for blood & metabolic disorders
|
Disease |
Sequela |
ABDS 2018 health |
|---|---|---|
|
Cystic fibrosis |
Non-respiratory complications due to cystic fibrosis |
207 |
|
Respiratory complications due to cystic fibrosis |
55, 56, 57 |
|
|
Haemophilia |
Haemophilia |
128, 207, 262 |
|
Haemolytic anaemia |
Haemolytic anaemia |
207 |
|
|
Acute, severe event due to haemolytic anaemia |
194, 2 |
|
|
Anaemia due to haemolytic anaemia(b) |
196, 197 |
|
Iron deficiency anaemia |
Anaemia due to iron-deficiency anaemia(b) |
195, 196, 197 |
|
Protein-energy deficiency |
Stunting due to protein-energy deficiency |
211 |
|
Wasting due to protein-energy deficiency |
210, 211 |
|
|
Other blood & metabolic disorders |
Anaemia due to other blood & metabolic disorders(b) |
197 |
|
Non-anaemic deficiency due to other blood & metabolic disorders |
195 |
|
|
|
Immune suppression due to other blood & metabolic disorders |
10 |
|
|
Metabolic dysfunction due to other blood & metabolic disorders |
31 |
(a) See ABDS 2018 health states.
(b) Part of anaemia envelope.
Prevalence estimation
Anaemia envelope
As an envelope in the ABDS 2018, the overall prevalence of anaemia was calculated to ensure the sum of estimates for sequelae do not exceed the total. Diseases that include anaemia as sequelae include iron-deficiency anaemia, haemolytic anaemia, uterine fibroids, chronic kidney disease, gastroduodenal disorders and maternal haemorrhage.
The following section describes the method used to calculate anaemia envelope estimates and anaemia due to iron-deficiency anaemia in the ABDS 2018. Methods for estimating sequelae from the other diseases are found in their respective disease groups.
Prevalence estimation of the anaemia envelope
Prevalence rate of individuals at risk of anaemia in ages 10 and over, by age and sex, were derived from self-reported data from the NHS 2017–18 (ABS 2019). To account for individuals with undiagnosed anaemia, sex-specific ratios of self‑reported: biomedical anaemia were estimated from the AHS 2011–12 (ABS 2013a) and applied to calculated prevalence rates from the NHS 2017–18. The AHS 2011–12 survey was used as biomedical data were not available from the NHS 2017–18. Additionally, the NHS did not report on Very remote areas,
so prevalence was modelled to account for Very remote areas.
Similarly to the ABDS 2015, iron-deficiency anaemia was assumed to be prevalent among 4% of children aged under 1 (Oti-Boateng et al. 1998), 2% of children aged 1–4 (Looker et al. 1997; Mackerras et al. 2004), and 1% for children aged 5–10 (Sadler & Blight 1996).
To avoid double counting, the sum of estimates of anaemia as sequelae due to other disease were subtracted from the anaemia envelope estimates. This included estimates for anaemia due to haemolytic anaemia, uterine fibroids, chronic kidney disease and gastroduodenal disorders. Methods for estimating anaemia due to these conditions are described in their respective disease groups. Once all anaemia sequelae have been subtracted, the remainder results in the prevalence of iron-deficiency anaemia.
Maternal haemorrhage estimates were not included in this subtraction, as this condition is short term. It is also not included in the NHS 2017–18 results.
Cystic fibrosis
Prevalence of cystic fibrosis was derived from the Australian Cystic Fibrosis Data Registry (ACFDR) (Ruseckaite 2020, pers. comm. 18 June). Registrants by age, sex and severity (lung function) was obtained for all ages.
The ACFDR includes numerous markers for severity, but these conflict with other components of the ABDS 2018 (risk factor and comorbidity analyses), or are captured elsewhere (for example, in respiratory infections). Therefore, lung function was used to attribute the proportion and severity of respiratory complications due to cystic fibrosis; however, in the ACFDR, there were a proportion of cystic fibrosis registrants with normal lung function when tested. These registrants had other consequences from cystic fibrosis, so a disability weight similar to mild lung function was applied to registrants with normal lung function to ensure the burden was adequately estimated for this group.
Haemophilia
Haemophilia in the ABDS 2018 included haemophilia A and B. Prevalence estimates and severity distribution were derived from the Australian Bleeding Disorders Registry 2017–18 report (National Blood Authority 2018).
The report provided severity estimates by haemophilia type, in broad age groups. The total male proportions for haemophilia A and B severity were applied to male prevalence estimates, assuming similar proportions across all ages. Based on clinical advice , it was assumed 95% of females with haemophila have mild and 5% have moderate haemophilia (Rowell 2015, pers. comm. 11 September).
Haemolytic anaemia
The same disabling sequelae for heamolytic anaemia as used in the ABDS 2015 were used in this study. The table below lists diagnosis and procedure codes (using the ICD-10-AM or Australian Classification of Health Interventions (ACHI) codes) for sequelae and severity distributions.
Table 4.6: Sequelae, severity and descriptions for haemolytic anaemia
|
Sequelae |
Severity |
Diagnosis/procedure descriptions |
ICD-10-AM/ |
|---|---|---|---|
|
Haemolytic anaemia |
Haemolytic anaemia |
All haemolytic anaemias |
D55–D58 |
|
Acute, severe event due to haemolytic anaemia |
Acute haemolytic crisis |
Sickle cell crisis |
D57.0 |
|
|
Surgical intervention: splenectomy |
Haemolytic anaemias with splenectomy procedure code |
Block: 815 |
|
Anaemia due to haemolytic anaemia |
Moderate anaemia |
Haemolytic anaemias excluding beta-thalassaemia |
D55–D58, excluding D56.1 |
|
|
Severe anaemia |
Beta-thalassaemia |
D56.1 |
Prevalence estimates for haemolytic anaemia were derived from the NHMD. Separations were ranked according to severity, if separations included more than 1 haemolytic anaemia diagnosis.
As a person can have multiple hospital separations in a single year, linked data from the NIHSI AA v0.5 were used to derive persons‑to‑separations ratios by sex and haemolytic anaemia type. These ratios were applied to national separations to estimate the number of people admitted. It is assumed that the hospital presentation ratios for haemolytic anaemia are the same for all states/territories.
Duration of health loss for haemolytic anaemia and anaemia was assumed to be for the entire year. Duration for individuals with splenectomy and acute sickle cell episodes was assumed to be 2 weeks and 7 days, respectively.
Iron deficiency anaemia
Iron deficiency anaemia in this study is inclusive of anaemia caused by iron deficiency and by unspecified causes. Methods to estimate iron-deficiency anaemia were described previously.
Severity was based on haemoglobin level definitions for mild and moderate anemia (WHO 2011). The severity distribution used in the ABDS 2011 (derived from AHS 2011–12 biomedical data) was used for the ABDS 2018.
Protein-energy deficiency
In this study, burden due to protein-energy deficiency was only estimated for elderly individuals and Indigenous children under 5, as these are the population group most likely to be affected in Australia.
Estimates of protein-energy deficiency in elderly Australians are restricted to individuals residing in nursing homes and those receiving at-home care.
Estimates were derived from an Australian community-living based study assessing malnutrition using the gold standard Mini Nutritional Assessment. This study showed that 35% of residents were at risk of malnutrition and 8.1% were malnourished (Rist et al. 2012).
People at risk of malnutrition were considered to have mild malnutrition (based on the Mini Nutritional Assessment score highlighting nutritional decline in the previous 3 months and intervention required), and people who were malnourished were considered to have moderate/severe malnutrition. These proportions were applied to the number of people living in permanent residential aged care facilities or receiving in-home care services, by sex at a state and remoteness level (AIHW 2020).
It is acknowledged that a proportion of malnutrition in the elderly population might include individuals who are in the end stages of life. As it is not possible to distinguish the cause of malnutrition, estimates in this population might be slightly overestimated.
Data from the AATSIHS 2012–13 was used to estimate the prevalence of protein-energy deficiency in Indigenous children in 2011. As advised by experts, underweight status is indicative of mild malnutrition in the Indigenous population. Severity distributions were derived from the AATSIHS underweight class, with levels 2 and 3 identified as wasting (Cole et al. 2007). To align state distributions to remoteness area estimates, the severity distribution for the Northern Territory was used for Outer regional, Remote and Very remote prevalence estimates. National severity distributions were used for Major cities and Inner regional areas. Estimates for 2003, 2015 and 2018 were derived by applying the 2011 Indigenous rate to the Indigenous ERPs for 2003, 2015 and 2018 (from the 2016 Census).
Other blood and metabolic conditions
This group includes deficiency anaemia, acquired haemolytic anaemias, coagulation defects, immune mechanism disorders, nutritional deficiencies and metabolic disorders.
To estimate prevalence, separations based on principal diagnosis in the NHMD were used. The ICD‑10-AM codes were grouped according to the main disabling sequelae, and durations applied to the number of separations to derive prevalence (see Definitions and durations for other blood and metabolic conditions below).
Durations were based on hospital analyses of length of stay, or durations used for conditions considered of similar burden.
Table 4.7: Definitions and durations for other blood and metabolic conditions
|
Sequelae |
ICD-10-AM codes |
Duration |
|---|---|---|
|
Anaemia due to other blood and metabolic disorders |
D51.0–D53.9, D59.0–D65, D68.0–D69.9 |
56 days |
|
Immune suppression due to other blood and metabolic disorders |
D70–D77, D80.0–D84.9, D86.1–D86.3, D86.8, D89.0–D89.9 |
2.4 days |
|
Non-anaemic deficiency due to other blood and metabolic disorders |
E00.0–E02, E50.0–E56.9, E58–E61.9, E63–E65, E67–E68 |
6 months |
|
Metabolic dysfunction due to other blood and metabolic disorders |
E70.0–E80.7, E83.0–E83.9, E85.0–E85.2, E88.0–E89 |
7 days |
Sub-national estimates
State and territory prevalence estimates for blood & metabolic disorders were based directly from the data source for each condition used to derive national prevalence. Prevalence estimates by remoteness and socioeconomic group were derived from hospital separations data in 2018.
2015, 2011 and 2003 estimates
2015, 2011 and 2003 estimates were based on the same method as for 2018.
Hospital separations were derived from the 2015, 2011 and 2003 calendar year.
Registrant data from 2015, 2011 and 2003 were used to estimate haemophilia and cystic fibrosis prevalence in the respective year. Where age and sex or severity distributions were unavailable, these were obtained from reports closest to the reference year that provided this information.
Total iron-deficiency anaemia prevalence estimates for 2011 were derived from the biomedical data from the AHS 2011–2012. Estimates for 2003 and 2015 were derived from self-reported estimates from the NHS 2004–2005 and NHS 2014–15 adjusted for under-reporting. Adjustment factors were based on the difference between self-reported and biomedical measures of anaemia in the AHS 2011–12. Age- and sex-specific severity distributions from 2011 were applied to self-reported estimates to obtain age- and sex-specific prevalence rates and applied to population estimates to attain prevalence for 2003 and 2015.
Estimates for protein-energy deficiency in elderly Australians for 2015, 2011 and 2003 used the same method as in 2018 but was based on the number of people living in permanent residential aged care facilities or receiving in-home care services in the respective years, by sex.
Indigenous specific estimates
Where possible, the same general methods and data sources were used to derive Indigenous estimates for blood & metabolic disorders for 2018, 2011 and 2003.
Indigenous estimates based on hospital separations data were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
Registrant data for cystic fibrosis and haemophilia did not contain reliable Indigenous identifiers, therefore hospital separations data was used to estimate prevalence. Based on expert advice, these conditions are not as prevalent in the Indigenous population.
NHMD separations, biomedical data from the AATSIHS 2012–13 (ABS 2020a) and self-report data from NATSIHS 2018–19 (ABS 2020b) were used to estimate iron-deficiency anaemia in 2018, using the same method as used for the national population. The 2011 estimates were calculated using NHMD anaemia separations applied to sex-specific AATSIHS totals to create the anaemia envelope. The 2003 estimates were created by applying the 2011 envelope rates to the 2003 Indigenous population. For all years, other sequela were removed from the envelope to leave IDA. The national severity splits were applied.
The same data source and method used to estimate protein-energy deficiency in the national population was used for the 2018, 2011 and 2003 Indigenous population.
References
ABS (Australian Bureau of Statistics) 2013. Australian Health Survey: users’ guide, 2011–13, ABS cat. no. 4363.0.55.001. Canberra: ABS.
ABS 2019. National Health Survey: users’ guide, 2017–18, ABS cat. no. 4363.0. Canberra: ABS.
ABS 2020a. Microdata: Australian Aboriginal and Torres Strait Islander Health Survey: biomedical results 2012–13, AIHW analysis of Datalab. Accessed 21 April 2021.
ABS 2020b. Microdata: National Aboriginal and Torres Strait Islander Health Survey, 2018–19. AIHW analysis of Datalab. Accessed 21 April 2021.
AIHW 2020. National Aged Care Data Clearinghouse. Accessed 8 July 2021.
Cole TJ, Bellizzi MC, Flegal KM and Dietz WH 2000. Establishing a standard definition for child overweight and obesity worldwide: international survey. British Medical Journal 320:1240–3.
Looker A, Dallman P, Carroll M, Gunter E and Johnson C 1997. Prevalence of iron-deficiency in the United States. The Journal of the American Medical Association 277(12):973–6.
Mackerras D, Hutton S and Anderson P 2004. Haematocrit levels and anaemia in Australian children aged 1–4 years. Asia Pacific Journal of Clinical Nutrition 13(4):330–5.
National Blood Authority 2018. Australian Bleeding Disorders Registry annual report 2017–2018, National Blood Authority.
Oti-Boateng P, Seshadri R, Petrick S, Gibson RA and Simmer K et al 1998. Iron status and dietary iron intake of 6–24-month-old children in Adelaide. Journal of Paediatric Child Health 34(3):250–3.
Rist, G, Miles G and Karimi L 2012. The presence of malnutrition in community-living older adults receiving home nursing services. Nutrition & Dietetics 69(1):46–50.
Sadler S and Blight G 1996. Iron status and dietary iron intake of young women. Proceedings of the Nutrition Society of Australia 20:216.
WHO 2011. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva: WHO. Accessed 26 August 2014.
Methods for cancer and other neoplasms mostly remained the same between the ABDS 2015 and the ABDS 2018. The most notable changes are in the use of linked data from the NIHSI AA v0.5 instead of linked data from the Western Australian Department of Health.
Sequelae and health states
Sequelae and health states for cancer & other neoplasms are based on the progression through 4 phases from diagnosis through metastases to potential death (see General cancer-related sequelae and health states below). For select cancers, it also includes long‑term sequelae—usually as a result of curative treatment (see Long-term cancer sequelae and health states below).
Table 4.8: General cancer-related sequelae and health states
|
Sequelae |
Health state |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Diagnosis and primary therapy phase of <cancer type> |
Cancer: diagnosis and primary therapy |
18, 208(b) |
|
Controlled phase of <cancer type>(c) |
Generic uncomplicated disease: worry and daily medication |
207 |
|
Metastatic phase of <cancer type>(d) |
Cancer: metastatic |
19 |
|
Terminal phase of <cancer type>(e) |
Terminal phase: with medication |
22 |
(a) See ABDS 2018 health states.
(b) For uncomplicated non-melanoma skin cancer only.
(c) Non-melanoma skin cancer model did not include controlled phase health state.
(d) Benign & uncertain brain tumours and breast ductal carcinoma in situ models did not include metastatic phases.
(e) Breast ductal carcinoma in situ models did not include terminal phases.
Table 4.9: Long-term cancer sequelae and health states
|
Disease |
Sequelae |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Laryngeal cancer |
Laryngectomy due to laryngeal cancer |
212 |
|
Bowel cancer |
Stoma due to bowel cancer |
21 |
|
Breast cancer |
Mastectomy due to breast cancer |
20 |
|
Prostate cancer |
Impotence due to prostate cancer |
49 |
|
|
Urinary incontinence due to prostate cancer |
48 |
|
Bladder cancer |
Stoma due to bladder cancer |
21 |
|
|
Urinary incontinence due to bladder cancer |
48 |
|
Brain and central nervous system cancer |
Brain injury (mild, moderate, severe) due to brain and central nervous system cancer |
181, 182, 183 |
|
Benign brain tumours |
Brain injury (mild, moderate, severe) due to benign brain tumours |
181, 182, 183 |
|
Ductal carcinoma in situ |
Mastectomy due to ductal carcinoma in situ |
20 |
(a) See ABDS 2018 health states.
General sequelae
Average durations for each general sequela for the various cancers were primarily taken from the GBD 2013, though a small number that were developed specifically for the ABDS 2011 based on expert advice were used in the ABDS 2015 and ABDS 2018 (see Supplementary table S4.1). Durations were applied to the relevant epidemiological measure for each sequela to derive point prevalence.
Principal diagnosis and primary therapy
Health loss due to diagnosis and treatment of malignant cancer (except non-melanoma skin cancer—NMSC) and ductal carcinoma in situ (DCIS) was based on incidence data from the 2016 ACD. This assumes that people will undergo primary treatment at the time of diagnosis.
The diagnosis and primary therapy health state for NMSC was divided into 2 severity levels, depending on whether the cancer was treated in community settings (uncomplicated NMSC) or hospital settings (complex NMSC).
Uncomplicated NMSC diagnoses and treatments were sourced from Medicare Benefits Schedule claims for first surgical excision of keratinocyte cancers and adjusted for histological confirmation. Histological confirmation is based on information from the QSkin Study by QIMR Berghofer Medical Research Institute (Thompson et al. 2014).
Complex NMSC diagnoses and treatments were sourced from separations in the NHMD with a principal diagnosis of NMSC in 2018 that underwent a skin-related surgery.
As benign and uncertain tumours of the brain and central nervous system are only reported to cancer registries in Victoria, Queensland and Western Australia, the number of incident cases undergoing diagnosis and primary therapy was not directly obtainable. Instead, the age‑specific ratio of benign or uncertain brain tumours in the ACD to separations in the NHMD for Victoria, Queensland and Western Australia was applied to separations from other jurisdictions, to derive national and sub-national estimates. As no incidence data are available for 2015, incidence data for all jurisdictions was obtained by applying the age-specific ratio of incidence to separations from 2014 to separations for 2015.
Incident cases for other non-malignant neoplasms were sourced from the NHMD (acknowledging that this will be the more severe end of the spectrum) using principal diagnosis, adjusted for repeat admissions.
Controlled phase
Health loss due to controlled phase of cancer was based on those people who were alive at the end of 2018 with a diagnosis of cancer in the previous 5 years—this assumes an effective cure rate of 5 years for all cancers.
Health loss is assumed for the full year for each prevalent case, minus the total person-time spent in diagnosis and primary therapy. As prevalent cases must have been alive on 31 December 2018, there is no overlap with people who died that year. Prevalence data were sourced from the ACD, which includes a linkage to the National Death Index to estimate prevalence.
Metastatic and terminal phases
Health loss due to metastatic cancer and terminal cancer in the reference year was based on people who died from cancer in that year (regardless of when they were diagnosed). This assumes that the number of people with metastatic and terminal phases who die of something other than cancer is small. Health loss experienced by people dying early in the following year is equal to health loss experienced in the preceding year by people dying early in the year.
For consistency, deaths from cancer were sourced from the fatal component of the study.
Long-term sequelae
Long-term sequelae were assumed to apply to all survivors (not just those diagnosed in the previous 10 years) consistent with the GBD 2013 onwards. To enable comparison between all three time points, this life-time prevalence was truncated at 20 years as this is the longest prevalence available for 2003 (as cancer data starts in 1982). Health loss for long-term sequelae is assumed to apply for the full year.
Laryngectomy due to laryngeal cancer
Prevalence was based on the ratio of the number of partial or total laryngectomies with a principal diagnosis of laryngeal cancer (derived from the NHMD) to new cases of laryngeal cancer in 2018 (derived from the ACD). This was applied to the 20-year prevalence of laryngeal cancer derived from the ACD.
Stoma due to bowel cancer
Prevalence was based on the ratio of hospitalisations for permanent colostomies due to bowel cancer (derived from the NHMD) to new cases of bowel cancer in 2018. This ratio was applied to 20-year prevalence of bowel cancer.
As individuals cannot be ascertained in the NHMD it was not possible to determine which stomas were temporary or permanent. Instead, permanent stomas were estimated using the overall colostomy closure rate for any disease derived from the NHMD. The overall colostomy closure rate was obtained from the Western Australian Department of Health using linked hospitals data. This method assumes that the closure rate from Western Australia is consistent across Australia.
Mastectomy due to breast cancer or ductal carcinoma in situ
Prevalence of mastectomies due to breast cancer was based on the ratio of the number of mastectomies with a principal diagnosis of breast cancer (derived from the NHMD) to new cases of breast cancer in 2018 ACD. Age-specific ratios were applied to the 20-year prevalence of breast cancer for females; an overall ratio was applied for males.
As prevalence for ductal carcinoma in situ was not available in the ACD to support using the same method as for breast cancer, data from the NHMD were used directly to derive prevalence of mastectomies due to ductal carcinoma in situ. Hospital separations for mastectomies with a principal diagnosis of ductal carcinoma in situ from 2008–2018 were extracted from the NHMD. To derive prevalence from separations, a 7-year prevalence-to‑separations ratio was derived from NIHSI and applied to the number of national separations.
Impotence and urinary incontinence due to prostate cancer
Prevalence was based on the proportions of men diagnosed with localised prostate cancer experiencing impotence and/or urinary incontinence at 3-year follow-up, according to treatment type (Smith et al. 2009) adjusted for background proportion of urinary incontinence and impotence. These were applied to the 20-year prevalence of prostate cancer derived from the ACD.
As radical treatment is not generally offered to men over the age of 70, the proportion of men likely to have undergone different treatments in the previous 10 years was only applied to men aged under 80 in 2018 (to allow for 10 years since treatment). It was also assumed there was no health loss from impotence in males aged under 15. To ensure consistency across the ABDS, urinary incontinence is assumed not to apply to children aged under 5.
Stoma and urinary incontinence due to bladder cancer
In the ABDS 2018, urinary incontinence due to bladder cancer refers to the long-term effects of primary therapy for bladder cancer—that is, removal of the bladder (radical cystectomy). It does not refer to urinary incontinence experienced as a symptom of bladder cancer, which is assumed to be short term until seeking treatment.
Radical cystectomy usually results in a stoma or a neobladder being fitted in the patient, and long-term effects depend on the diversion type. Hospitalisations for radical cystectomy were used to estimate incidence hazard ratios for stomas and neobladders following bladder cancer. This was applied to the 20-year prevalence of bladder cancer from the ACD to obtain point prevalence estimates of stoma for each diversion type.
Proportions of patients with incontinence by diversion type were obtained from Gilbert and others 2007.
Brain injury due to malignant and benign brain tumours and central nervous system cancer
Due to the scarcity of data sources on the long-term impacts of cancer and other tumours of the brain, the ABDS 2018 assumed the proportion of all brain cancer survivors with long‑term sequelae was the same as the proportion of brain injury survivors with long-term sequelae (that is, 8% mild, 10% moderate, 5% severe), derived by the NZBDS (NZMOH 2013).
For brain cancer, these proportions were applied to the lifetime prevalence of brain cancer derived from the ACD. As prevalence of survivors of benign and uncertain brain tumours was not directly available, rate ratios of age-specific prevalence rates for malignant and non‑malignant tumours from a United States study (Porter et al. 2010) were applied to the lifetime prevalence of malignant tumours from the ACD to derive lifetime non-malignant prevalence.
Sub-national estimates
State and territory incidence and prevalence data were derived directly from the data—summing to create the national incidence and prevalence counts for each year.
Remoteness breakdowns of national estimates were derived by applying 2016 ASGS remoteness areas (for 2018 and 2015) and 2011 ASGS remoteness areas (for 2011 and 2003) to the Statistical Area Level 2 or Statistical Local Area recorded in hospitals and cancer mortality data, and postcode recorded in cancer incidence data. Deaths/cases with missing data (including data that could not be mapped) were proportionally assigned to remoteness groups based on the proportion of the population in each group, by state and sex.
Socioeconomic group breakdowns of national estimates were derived by applying 2016 SEIFA population-based IRSD quintiles (for 2018 and 2015) and 2011 SEIFA population-based IRSD quintiles (for 2011 and 2003) to the Statistical Area Level 2 or Statistical Local Area recorded in hospitals and cancer mortality data, and postcode recorded in cancer incidence data. Deaths/cases with missing data (including data that could not be mapped) were proportionally assigned to socioeconomic groups based on the proportion of the population in each group, by state and sex.
2015, 2011 and 2003 estimates
All estimates for the years 2003, 2011 and 2015 were estimated using cancer incidence and prevalence derived from the ACD and cancer mortality from the NMD, for the reference years in the same way as for 2018.
As Medicare Benefits Schedule item codes might have changed over time, the positive predictive value (PPV) provided from the QSkin Study could not be assumed to apply to estimated incidence of NMSC for the year 2003. Instead, incidence from the 2002 survey by Staples and others (2006) was used for the incidence of simple NMSC, on the assumption that most would have had a simple excision prior to any complex treatment. For 2011 and 2015 estimates are produced by using MBS data with a PPV of 68% and a duration of 2 weeks applied to the MBS services for selected items. As the services are provided in 10–15 year age groups, estimates for 5-year age groups are created by applying the overall 10-year prevalence rate to its constituent 5-year age groups.
Hospital separations data were used for health loss due to complex treatment as for 2018.
Long-term sequelae were derived in the same way using year-specific ratios. Where the NHMD was the primary data source, separations from the respective calendar year was used.
For brain injury due to malignant and benign brain tumours and central nervous system cancer, the same rates were assumed as for 2015 estimates; however, as the ACD only contains data from 1982, the lifetime prevalence for 2003 has a much shorter look-back period, and so will be lower than for 2011, 2015 and 2018.
Indigenous specific estimates
The same general methods were used to derive 2018, 2011 and 2003 Indigenous estimates with the following exceptions:
The 2011 cancer incidence and prevalence for the Indigenous population were derived from the average cancer incidence recorded in the 2011 ACD for 2009-2011 for NT, WA, Victoria and Queensland, and from 2007–2009 for NSW—these are the states with cancer incidence data considered of sufficient quality for reporting. Rates from these states combined were applied to the ACT, Tasmania and SA populations to determine national Indigenous incidence. The 2011 mortality was derived from the average number of deaths in 2009–2011, adjusted for under-identification using ABS mortality adjustment factors as per fatal estimates (see Years of life lost (YLL)).
2003 cancer incidence and prevalence for the Indigenous population were derived from the average cancer incidence recorded in the 2011 version of the ACD for 2002–2004 for NT, WA, NSW and Queensland. Rates from these states combined were applied to the ACT, Victoria, Tasmania and SA populations to determine national Indigenous incidence. 2003 mortality was derived from the average number of deaths in 2002–2004, adjusted for under-identification using ABS mortality adjustment factors as per fatal estimates (see Years of life lost (YLL)).
Indigenous estimates for complex treatment of NMSC were identified from hospitals data for the relevant years, adjusted for under-identification using AIHW standard hospital adjustment factors described in Chapter 4 (see Years lived with disability (YLD)). As no Indigenous data were available for simple NMSC, the Indigenous:national ratio of complex NMSC was applied to the national simple NMSC estimates to derive Indigenous estimates for both 2011 and 2003.
National hazard:incidence ratios for long-term sequelae were applied to Indigenous prevalence estimates due to insufficient data to derive Indigenous-specific ratios. The exception to this was mastectomy where there were sufficient data to derive female Indigenous-specific (but not age-specific) ratios.
As the proportion of brain injury survivors is not currently available by Indigenous status, it was assumed to be the same as the national proportion.
The number of cases of ductal carcinoma in situ diagnosed in Indigenous women in was estimated by applying the ratio of small (i.e. < 2 cm) breast tumours in national:Indigenous women to the national incidence of ductal carcinoma in situ for both 2011 and 2003
References
Gilbert S, Wood D, Dunn R, Weizer A, Lee C, Montie J et al. 2007. Measuring health-related quality of life outcomes in bladder cancer patients using the bladder cancer index. Michigan: American Cancer Society. 109(9):1756–62.
NZMOH 2013. New Zealand Burden of Diseases, Injuries and Risk Factors Study 2006–2016. Wellington: NZMOH.
Porter KR, McCarthy BJ, Freels S, Kim Y & Davis FG 2010. Prevalence estimates for primary brain tumors in the United States by age, gender, behavior and histology. Neuro‑oncology 12(6):520–7.
Smith DP, King MT, Egger S, Berry MP, Stricker PD, Cozzi P et al. 2009. Quality of life three years after diagnosis of localised prostate cancer: population based cohort study. BMJ 339:b4817.
Staples MP, Elwood M, Burton RC, Williams JL, Marks R & Giles GG 2006. Non-melanoma skin cancer in Australia: the 2002 national survey and trends since 1985. MJA 184(1):6–10.
Thompson B, Olsen C, Subramaniam P, Neale R & Whiteman P 2014. Medicare data for cancer follow-up studies. Paper presented at the Australasian Epidemiological Association Annual Scientific Meeting, Auckland.
Methods for cardiovascular diseases mostly remained the same between the ABDS 2015 and the ABDS 2018. The most notable changes are in the use of linked data from the NIHSI AA v0.5 instead of linked data from the Western Australian Department of Health.
Sequelae and health states
Sequelae and health states assigned to the cardiovascular diseases are divided into acute and chronic. Heart failure is a sequela to a number of the cardiovascular diseases and is treated as an envelope condition. Sequelae, health states and durations are detailed in the next section.
Prevalence estimation
Acute sequelae
The NHMD was the main data source used to estimate prevalence of acute sequelae (see table below). As these events are of short duration, point prevalence was estimated by applying the duration of health loss to incidence.
Table 4.10: ABDS 2018 diseases and sequelae that use the NHMD to estimate point prevalence
|
Disease |
Sequela |
ABDS 2018 health |
Duration |
|
Coronary heart disease |
Acute coronary syndrome |
24, 25 |
2 days (more severe) |
|
|
|
|
26 days (less severe) |
|
Stroke |
Acute stroke |
34, 35, 36, 37, 38 |
28 days |
|
Rheumatic heart disease |
Acute rheumatic fever |
3 |
84 days (3 months) |
|
Inflammatory heart disease |
Acute inflammatory heart disease |
2 |
28 days |
|
Aortic aneurysm |
Symptomatic aortic aneurysm requiring repair |
193, 194 |
28 days (ruptured) |
|
|
|
|
14 days (non-ruptured) |
|
|
|
|
2 days (endovascular stent/other surgery) |
(a) See ABDS 2018 health states.
Acute coronary syndrome
As health loss from acute coronary syndrome is short-term, point prevalence was estimated using incidence (events) multiplied by the duration for each of the 2 severity levels (2 and 26 days, respectively).
As there is no national data source, acute coronary syndrome incidence was estimated using AIHW analyses of linked hospitalisations and deaths data from the NIHSI AA v0.5 to determine the number of non-fatal acute coronary syndrome events in the reference year, using methods previously published by the AIHW (AIHW 2014b). Acute coronary syndrome hospitalisations were defined as separations with a principal diagnosis of ICD-10-AM I20.0 and I21. Transfers and readmissions within 28 days were excluded to avoid double-counting of the same event. State-specific incidence rates were available for New South Wales, Victoria, South Australia and Tasmania, i.e. the States that are available in the NIHSI AA v0.5. Incidence rates combining the 4 jurisdictions were used to estimate the incidence in the remaining States and Territories.
Acute stroke
Hospitalisation data were chosen over data from epidemiological studies due to the currency, national coverage and ability to provide estimates at the sub-national level.
Incidence was calculated by counting the number of non-fatal separations due to stroke (defined as principal diagnosis of ICD-10-AM I60–I64) in the reference year in the NHMD.
Prevalence (incidence times duration) estimates were then split into the 5 severity levels using proportions obtained from the GBD 2013 (Burstein et al. 2015), which were reapportioned to exclude asymptomatic acute stroke since it was not included in the estimates from the NHMD.
Acute rheumatic fever
Incidence was calculated by counting the number of non-fatal separations due to acute rheumatic fever (defined as principal diagnosis of ICD-10-AM I00–I02) in the reference year in the NHMD. A duration of 84 days (or 3 months) was applied to estimate point prevalence. It was assumed that any readmission for acute rheumatic fever within a period of 84 days was likely caused by the same event. Hospitalisation ratios were calculated using linked hospitals and deaths data from the NIHSI AA v0.5 were used to account for potential readmissions within 84 days.
Acute inflammatory heart disease
Incidence was estimated by counting the number of separations due to acute inflammatory heart disease in the NHMD in the reference year. These were defined as separations with a principal diagnosis of ICD-10-AM: I30–I33, I40–I41.
Aortic aneurysm
Aortic aneurysm is an acute condition. Cases of aortic aneurysm are defined as hospitalised patients with a principal diagnosis of aortic aneurysm (ICD-10-AM I71) and having undergone a surgical repair. Point prevalence was estimated by applying the appropriate duration depending on whether it was a ruptured or non-ruptured aortic aneurysm and the kind of surgery (that is, open repair surgery, an endovascular stent or other surgery).
Chronic sequelae
The prevalence of chronic sequelae were estimated using NHMD, linked hospitalisations and deaths data from the NIHSI AA v0.5 and the NZBDS.
The sequelae for which a combination of NHMD and linked hospitals and deaths data from the NIHSI AA v0.5 were used are listed in the table below. Heart failure is discussed separately from the other chronic sequelae as it is an envelope condition.
Table 4.11: ABDS 2018 diseases and sequelae that use a combination of the NHMD and the NIHSI AA v0.5 to estimate prevalence
|
Disease |
Sequela |
ABDS 2018 health |
|---|---|---|
|
Coronary heart disease |
Chronic coronary heart disease |
26, 27, 28, 262 |
|
|
Heart failure due to coronary heart disease(b) |
31, 32, 33 |
|
Stroke |
Chronic stroke |
34, 35, 36, 37, 38, 262 |
|
Rheumatic heart disease |
Valvular diseases due to rheumatic heart disease |
207 |
|
|
Heart failure due to rheumatic heart disease(b) |
31, 32, 33 |
|
Non-rheumatic heart disease |
Valvular diseases due to non-rheumatic heart disease |
207 |
|
|
Heart failure due to non-rheumatic heart disease(b) |
31, 32, 33 |
|
Atrial fibrillation and flutter |
Moderate/severe atrial fibrillation and flutter |
29 |
|
Hypertensive heart disease |
Heart failure due to hypertensive heart disease(b) |
31, 32, 33 |
|
Inflammatory heart disease |
Heart failure due to inflammatory heart disease(b) |
31, 32, 33 |
|
Cardiomyopathy |
Heart failure due to cardiomyopathy(b) |
31, 32, 33 |
|
Cardiovascular defects(c) |
Heart failure due to congenital cardiovascular defects(b) |
31, 32, 33 |
|
Peripheral vascular disease |
Intermittent claudication due to peripheral vascular disease |
30 |
(a) See ABDS 2018 health states.
(b) Part of the heart failure envelope.
(c) Included under infant & congenital conditions.
For sequelae that are considered chronic (this includes chronic coronary heart disease, chronic stroke, rheumatic heart disease, non-rheumatic valvular disease and peripheral vascular disease), it was assumed that people who have these diseases are hospitalised at least once within the 7 years leading up to the reference year. A 7-year look-back period was used as it was the longest time period available for hospitals data in the NIHSI AA v0.5.
Repeat hospitalisations are not discernible in national hospitalisation admission data. To adjust for repeat hospitalisations, the ratio of people alive at the reference date who had at least 1 hospital separation due to the chronic sequela to the number of separations by broad age group and sex was derived from linked hospitalisations and deaths data from the NIHSI AA v0.5.
These ratios were then applied to the count of hospital separations from the NHMD, by age and sex. Admitted hospitals data are available from the NIHSI AA v0.5 for New South Wales, Victoria, South Australia and Tasmania. Where numbers allow, that is, the numbers are not low enough to cause volatility in estimates, state-specific ratios are calculated. Otherwise, data from all 4 jurisdictions are used for the ratios. For States/Territories that do not have hospitals data in the NIHSI AA v0.5, ratios calculated using all 4 jurisdictions combined are used. This assumes that persons-to-separations ratios are similar across all jurisdictions.
The prevalence of chronic coronary heart disease was broken down by severity using severity distributions from the GBD 2013 (Burstein et al. 2015).
The prevalence of chronic stroke was broken down by severity using distributions from the GBD 2013 (Burstein et al. 2015). This distribution was adjusted for age differences using the age gradient of health experienced by stroke survivors 12 months after their first stroke from the Perth Community Stroke Study 1989–1990 (Katzenellenbogen et al. 2010).
Due to a lack of robust population-based Australian data, the NZBDS was used to estimate the overall prevalence of atrial fibrillation and flutter. These rates were considered appropriate for Australia in the absence of local data as they were derived from linked administrative data.
Atrial fibrillation and flutter
The prevalence of all atrial fibrillation & flutter (referred to as atrial fibrillation for the rest of this section) in Australia was estimated using the non-Maori prevalence rates from the NZBDS.
The prevalence of moderate/severe atrial fibrillation was estimated by counting the number of separations with atrial fibrillation listed as the principal diagnosis in the reference year in the NHMD. The number of people were estimated by applying persons-to-separations ratios to the count of separations.
The prevalence of mild atrial fibrillation was estimated by subtracting the prevalence of moderate/severe atrial fibrillation from the overall atrial fibrillation prevalence in Australia.
Heart failure envelope
Similar to the other chronic conditions mentioned previously (such as chronic coronary heart disease and chronic stroke), the prevalence of heart failure was estimated by applying prevalence-to-separations ratios from linked hospitalisations and deaths data from the NIHSI AA v0.5 to the national count of separations from the NHMD.
As one of the envelopes in the ABDS 2018, the overall prevalence of heart failure from all diseases was calculated to ensure the sum of estimates for sequelae do not exceed the total. To avoid double-counting, and adhere to mutual exclusivity for each disease, weights were created for each disease using results from linked data from the NIHSI AA v0.5. Where heart failure was diagnosed with no other accompanying cardiovascular disease diagnosis, these were redistributed to other diseases using proportional allocation.
Heart failure has 3 severity levels: mild, moderate, severe. Severity distributions were obtained from the GBD 2013 (Burstein et al. 2015).
Sub-national estimates
Where prevalence was obtained from the NHMD, sub-national estimates were derived directly by applying 2016 (for 2018 and 2015 estimates) and 2011 SEIFA population-based IRSD quintiles to the Statistical Area Level 2 recorded in hospital separations data.
For atrial fibrillation, prevalence by State or Territory, remoteness area, and socioeconomic group were obtained by applying proportions by sub-national disaggregation from separations in the NHMD.
2015, 2011 and 2003 estimates
For chronic sequelae where prevalence was estimated from a combination of the NHMD and ratios and rates derived from the NIHSI AA v0.5, methods for 2003, 2011 and 2015 were largely similar to those for 2018. However, due to a change in the diagnosis classification and to the absence of available linked data before 1 July 1999, the look-back period from 2003 was limited to 4 years. To achieve comparable estimates, 2003 estimates were derived from 2006 prevalence rates. It was assumed that rates were relatively stable between 2003 and 2006.
For acute coronary syndrome, acute stroke and acute inflammatory heart disease, the methods used for 2003, 2011 and 2015 prevalence estimates were the same as those used for 2018 estimates. For acute rheumatic fever, the hospital ratio used to adjust for readmission for 2011 estimates was used for 2003 prevalence estimates. For atrial fibrillation and flutter, the NZBDS prevalence rates used for 2018 estimates were also used for 2015, 2011 and 2003 estimates.
Indigenous specific estimates
The general approach and method used for national estimates were used for the Indigenous estimates. The severity distribution used for national estimates was also used for Indigenous estimates. For diseases and sequelae (Table 4.10) where the NHMD was used to estimate point prevalence, hospital separations data were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
For diseases and sequelae (Table 4.11) where ratios from the NIHSI AA were used to estimate prevalence, Indigenous-specific ratios from the Western Australian Linked Data Set were obtained from the WA Department of Health.
For atrial fibrillation and flutter, where non-Maori prevalence rates from the NZBDS were used for the national prevalence estimates, the Maori prevalence rates were applied to Indigenous populations for the relevant reference years to derive Indigenous prevalence estimates.
References
AIHW 2014b. Acute coronary syndrome: validation of the method used to monitor incidence in Australia. Cat. no. CVD 68. Canberra: AIHW.
Burstein R, Fleming T, Haagsma J, Salomon JA, Vos T & Murray CJL 2015. Estimating distributions of health state severity for the global burden of disease study. Population Health Metrics 13:31.
Katzenellenbogen JM, Begg S, Somerford P, Anderson CS, Semmens JB, Codde JP et al. 2010. Disability burden due to stroke in Western Australia: new insights from linked data sources. International Journal of Stroke 5:269–77.
Sequelae and health states
Sequelae and health states assigned to endocrine disorders are shown in the table below
Table 4.12: Sequelae and health states for endocrine disorders
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Type 1 diabetes |
Amputation due to type 1 diabetes |
140 |
|
|
Diabetic foot ulcer |
39 |
|
|
Diabetic neuropathy |
40 |
|
|
Diagnosed diabetes |
207 |
|
|
Vision impairment due to type 1 diabetes |
114, 115, 116 |
|
Type 2 diabetes |
Amputation due to type 2 diabetes |
140 |
|
|
Diabetic foot ulcer |
39 |
|
|
Diabetic neuropathy |
40 |
|
|
Diagnosed diabetes |
207 |
|
|
Vision impairment due to type 2 diabetes |
114, 115, 116 |
|
Other diabetes mellitus |
Diagnosed other diabetes |
207 |
|
Other endocrine disorders |
Other endocrine disorders |
. . |
(a) See ABDS 2018 health states.
Prevalence estimation
Type 1 diabetes
Diagnosed type 1 diabetes
The prevalence of type 1 diabetes mellitus was sourced from the National (insulin-treated) Diabetes Register (NDR). Data for the NDR are sourced from the National Diabetes Services Scheme (NDSS) Registrant data, the NDSS Sales data, the Australasian Paediatric Endocrine Group (APEG) state-based registers and the National Death Index (NDI). The prevalence estimates were provided by the Cardiovascular, Diabetes and Kidney Unit of the AIHW. For more information on these data sets, refer to the National (insulin-treated) Diabetes Register 2018 Quality statement.
Diabetic neuropathy and foot ulcer
The overall prevalences of diabetic neuropathy, diabetic foot syndrome and vision loss due to type 1 diabetes were obtained from phase 2 of the Fremantle Diabetes Study (Davis 2018, pers. comm., 8 March; Sämann et al. 2008). Prevalence estimates by sex and age were modelled using the national sex and age group distribution. Prevalence was modelled to start at age 20; this decision was informed by data from the NHMD.
Amputation due to type 1 diabetes
The prevalence of amputation due to type 1 diabetes was estimated using the NHMD and persons‑to‑separations ratios derived from linked hospitalisations and deaths data from the NIHSI AA v0.5. This was used to adjust the count of separations from the NHMD to better estimate prevalence. An amputation was determined as being due to type 1 diabetes if there was a principal or additional diagnosis of type 1 diabetes accompanying a lower limb amputation in the hospitalisation.
Vision impairment due to type 1 diabetes
Similar to diabetic neuropathy and diabetic foot syndrome, the prevalence estimates for vision impairment due to diabetes were calculated using results from phase 2 of the Fremantle Diabetes Study (unpublished data). Breakdowns by sex and age were modelled using data from the NHMD.
This sequela has 3 severity levels: moderate, severe and blindness. The severity distribution used for the prevalence was obtained from the study by Wong et al. (2009).
Type 2 diabetes
Diagnosed type 2 diabetes
The prevalence of type 2 diabetes mellitus was sourced from self-report data from the NHS 2017–18, the NHS 2014–15, the AHS 2011–13 and the NHS 2004–05. Due to high Relative Standard Errors (RSEs) for a number of the younger and older age groups, prevalence rates by sex and 5-year age group were modelled. Since the health surveys do not survey the Very remote areas, weighted counts of type 2 diabetes were inflated to include prevalence in Very remote areas.
Diabetic neuropathy and foot ulcer
The overall prevalence of diabetic neuropathy, diabetic foot syndrome and vision loss due to type 2 diabetes were obtained from phase 2 of the Fremantle Diabetes Study (Baba et al. 2015; WA Davis 2018, pers. comm., 7 March; WA Davis 2020, pers. comm., 16 April). Prevalence estimates by sex and age were modelled using the national sex and age group distribution. Prevalence was modelled to start at age 25; this decision was informed by data from the NHMD.
Amputation due to type 2 diabetes
The prevalence of amputation due to type 2 diabetes was estimated using the same method as amputation due to type 1 diabetes—where a principal or additional diagnosis of type 2 diabetes accompanied a lower limb amputation.
Vision impairment due to type 2 diabetes
The prevalence of vision impairment due to type 2 diabetes was estimated using the same method as for vision impairment due to type 1 diabetes. The same severity distribution was used.
Other diabetes mellitus
The prevalence of other diabetes mellitus is difficult to estimate due to lack of robust national-level data. As such, the prevalence of complications due to other diabetes mellitus was not estimated.
The prevalence of other diabetes mellitus was estimated using the proportion of other diabetes from the Fremantle Diabetes Study (Davis et al. 2018). Sex by age distributions were obtained from the NHMD.
Other endocrine disorders
The prevalence of other endocrine disorders is the prevalence of all other endocrine disorders that are not diabetes. The YLD were estimated by applying a YLD:YLL ratio of diabetes to the YLL of the other endocrine disorders.
Sub-national estimates
Prevalence estimates by state/territory, remoteness area and socioeconomic group were derived from the same data source as the national estimates and modelled similarly.
2015, 2011 and 2003 estimates
Type 1 and other diabetes prevalence estimates for 2015, 2011 and 2003 were derived from the same data sources as the estimates for 2018.
For diagnosed type 2 diabetes, prevalence estimates were derived from the NHS 2014–15, the AHS 2011–12 and the NHS 2004–05 for 2015, 2011 and 2003, respectively. For 2015 and 2011, the prevalences of diabetic neuropathy, diabetic foot syndrome, vision impairment and amputation due to type 2 diabetes was estimated using the same data sources used for 2018 estimates.
For 2003, the overall prevalence for diabetic neuropathy, diabetic foot syndrome and vision impairment due to diabetes were obtained from the AusDiab Study (Tapp et al. 2003a, 2003b). Breakdowns by sex and age were modelled using data from the NHMD. Amputation due to type 2 diabetes was estimated using the same data sources as for the 2018 estimates.
Indigenous specific estimates
Indigenous prevalence for type 1 diabetes was derived from the linked National Diabetes Services Scheme (NDSS) and Australasian Paediatric Endocrine Group (APEG) data set. Indigenous-specific prevalence rates were used in people aged under 30 years, and national rates in people aged 30 and over, due to data quality issues. The prevalence of type 2 diabetes was estimated by subtracting the estimated number of Indigenous Australians with type 1 diabetes from estimated total diabetes prevalence estimated using data from the biomedical component of the AATSIHS 2012–13 and self-reported data from the 2018–19 NATSIHS.
The prevalence for each of the diabetic complications for Indigenous people (with the exception of amputation due to diabetes) were estimated using published (Davis et al. 2012) and unpublished results from the Fremantle Diabetes Study.
Amputations due to diabetes prevalence were estimated using the NHMD. Hospital separations data were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
The residual category of other endocrine disorders was estimated using the same method as used for national estimates (by applying the YLD:YLL ratio for diabetes to the YLL for other endocrine disorders).
References
Baba M, Davis WA, Norman PE & Davis TME 2015. Temporal changes in the prevalence and associates of foot ulceration in type 2 diabetes: the Fremantle Diabetes Study. Journal of Diabetes and its Complications 29:356–61.
Davis TME, Hunt K, McAullay D, Chubb SA, Sillars BA, Bruce DG et al. 2012. Continuing disparities in cardiovascular risk factors and complications between Aboriginal and Anglo-Celt Australians with type 2 diabetes: the Fremantle Diabetes Study. Diabetes Care 35(10):2005–11.
Davis WA, Peters KE, Makepeace A, Griffiths S, Bundell C, Gratn SFA et al. 2018. Prevalence of diabetes in Australia: insights from the Fremantle Diabetes Study Phase II. Internal Medical Journal 48(7):803–9.
Sämann A, Tajiyeva O, Müller N, Tschauner T, Hoyer H, Wolf G et al. 2008. Prevalence of the diabetic foot syndrome at the primary care level in Germany: a cross‑sectional study. Diabetic Medicine 25(5):557–63.
Tapp RJ, Shaw JE, de Courten MP, Dunstan DW, Welborn TA & Zimmet PZ 2003a. Foot complications in type 2 diabetes: an Australian population-based study. Diabetic Medicine 20:105–13.
Tapp RJ, Shaw JE, Harper CA, de Courten MP, Balkau B, McCarty DJ et al. 2003b. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 26:1731–7.
Wong TY, Mwamburi M, Klein R, Larsen M, Flynn H, Hernandez-Medina M et al. 2009. Rates of progression in diabetic retinopathy during different time periods: a systematic review and meta-analysis. Diabetes Care 32(12):2307–13.
Sequelae and health states
The sequela and health states assigned to gastrointestinal disorders are shown in the table below. Durations and assumptions are outlined in subsections for individual diseases.
Table 4.13: Sequelae, health states and durations for gastrointestinal disorders
| Disease | Sequela |
ABDS 2018 health state identifier(a) |
Duration |
|---|---|---|---|
| Gastroduodenal disorders | Anaemia due to gastroduodenal disorder(b) | 195, 196, 197 | 8 weeks |
| Symptomatic episodes of gastroduodenal disorder | 193 |
1 week (inflammation) 3 weeks (ulcers) |
|
| Appendicitis | Symptomatic appendicitis requiring appendectomy | 194 | 2 weeks |
| Abdominal wall hernia | Symptomatic hernia requiring repair | 192 | 12 months |
| Vascular disorders of intestine |
Stoma due to vascular disorder of intestine |
21 |
12 months (temporary stoma) |
| Vascular disorders of the intestine | 194 | 6 weeks | |
| Intestinal obstruction (without hernia) | Intestinal obstruction | 194 |
2 weeks (major surgery) 2 days (minor surgery) |
| Inflammatory bowel disease | Crohn’s disease or ulcerative colitis | 46 | 12 months |
| Diverticulitis | Diverticulitis | 194 |
2 weeks |
| Stoma due to diverticulitis | 21 |
12 months (temporary stoma) |
|
| Chornic liver disease |
Decompensated cirrhosis of the liver End-stage liver disease |
44 22 |
10 months (with end-stage liver disease) 2 months (terminal stage) |
| Liver transplant | 42 | 12 months | |
| Gallbladder and bile duct disease | Gallbladder and bile duct disease | 193 | 6 weeks |
| Pancreatitis | Acute episode of pancreatitis | 194 | 6 weeks |
| Chronic pancreatitis | 193 | 12 months | |
| Gastro-oesophageal reflux disease (GORD) | Mild symptomatic gastro-oesophageal reflux disease | 262 | |
| Moderate/severe symptomatic gastro‑oesophageal reflux disease | 192 | approx. 4 days/ week for 12 months | |
| Functional gastrointestinal disorders (FGID) | Functional heartburn due to functional gastrointestinal disorders | 192, 193 | 12 months |
| Irritable bowel syndrome | 192, 193 | 12 months | |
| Other gastrointestinal disorders | Other gastrointestinal disorders |
(a) See ABDS 2018 health states.
(b) Part of the anaemia envelope.
Prevalence estimation
The NHMD was the major data source to estimate prevalence of gastrointestinal disorders, unless otherwise stated. Separations for acute conditions were derived from the 2018, 2015, 2011 and 2003 calendar years, as applicable. The durations used for each sequela are presented in Table 4.13.
Patients hospitalised due to the specified gastrointestinal disorders experience significant health loss, especially if they undergo surgical intervention. A hospitalisation that requires surgery is considered more severe.
Gastroduodenal disorders
Gastroduodenal disorder includes duodenal and gastric ulcers (also referred to as peptic ulcer disease) as well as gastritis and duodenitis. The term ‘gastritis’ used here refers specifically to abnormal inflammation in the stomach lining, and is a pathological diagnosis, not clinical.
Endoscopic diagnosis of gastroduodenal disease is generally considered an under-count of total disease as it does not account for physician-diagnosed and treated disease. Estimates for uncomplicated gastroduodenal disease (which is generally diagnosed by a physician and successfully treated without hospitalisation) were derived by applying the rate ratio of physician-diagnosed peptic ulcer disease to hospitalised incidence (Sung et al. 2009), to the incidence of complicated gastroduodenal disorders. Complicated gastroduodenal disorders (which generally results in hospitalisation and endoscopic diagnosis) and resultant anaemia, were sourced from hospital separations for gastroduodenal disease. Separate durations were applied to prevalence estimates for gastritis/duodenitis (inflammation) and gastric/duodenal ulcers (Table 4.13).
Prevalence of anaemia due to gastroduodenal disorders was sourced from the NHMD. However, as data in the NHMD could not be used to estimate the severity of anaemia due to gastroduodenal disease, the global severity distributions of anaemia from the GBD 2013 were used for gastritis and peptic ulcers.
Appendicitis
Appendicitis is an acute condition. Cases of appendicitis—defined as hospitalised patients with a principal or additional diagnosis of appendicitis having undergone an appendectomy procedure—were assumed to be incident cases. The duration of health loss was assumed to be 2 weeks.
Abdominal wall hernia
Incident cases of abdominal wall hernia were defined as hospitalised patients with a principal or additional diagnosis of hernia having undergone a hernia-related procedure. The duration of health loss for patients with symptomatic hernia until repair was assumed to be 12 months. This was based on the NZBDS’s estimate of duration which accounts for the time between presentation of symptoms, referral and surgery (NZMOH 2012, unpublished documents).
Intestinal obstruction (without hernia)
Incident cases were defined as hospitalised patients with a principal or additional diagnosis of intestinal obstruction with surgical intervention. The duration of health loss for patients with intestinal obstruction (without hernia) varied depending on the type of surgery. Duration was assumed to be 2 weeks for those undergoing major surgery (consistent with the GBD 2017), and 2 days for those undergoing minor intervention based on expert advice.
Experts also advised that minor surgery should account for the majority of procedures to relieve intestinal obstruction; however, investigation of inpatient hospitals data showed that major surgery was performed in 5 times as many separations as minor surgery. This may be due to minor surgery being performed in an outpatient setting, resulting in a potential undercount of minor surgery.
Gallbladder and bile duct disease
Incident cases were defined as hospitalised patients with a principal or additional diagnosis of gallbladder and/or bile duct disease having undergone a cholecystectomy and/or incision of bile ducts. Patients admitted with diagnosis of gallbladder disease and/or cholelithiasis who did not undergo surgery have much milder symptoms which do not result in health loss for burden of disease analysis, and were not included in this analysis. Duration of health loss was assumed to be 6 weeks which is consistent with the GBD 2013.
Pancreatitis
Acute cases of pancreatitis were defined as hospitalised patients with a principal diagnosis of acute pancreatitis (ICD-10-AM K85). Patients with acute pancreatitis are incident cases of short duration. This diagnosis code includes acute episodes within a diagnosis of chronic pancreatitis (NCCH 2010, as described in ICD-10-AM, seventh edition by Australian Coding Standard 0001).
Chronic cases were defined as hospitalised patients with a principal or additional diagnosis of chronic pancreatitis (ICD-10-AM K86.0, K86.1). Patients with chronic pancreatitis are prevalent cases. Since individuals cannot be identified using national hospitalisations data, it was assumed that 1 separation was equal to 1 person. This might have resulted in an overestimation of chronic pancreatitis prevalence, which could be improved using linked hospitals data.
Vascular disorder of the intestine
Incident cases were defined as hospitalised patients with a principal diagnosis of vascular insufficiency with or without surgical intervention. Additional health loss was assigned to cases with a stoma opening procedure in either the small or large intestine.
Duration of health loss varied according to whether a stoma was permanent or temporary. It is not possible to tell from national hospitals data which of these patients’ stomas were subsequently closed. Instead, overall closure rates of stomas regardless of underlying disease derived from national hospitals data were used to estimate the number of permanent stomas, and the duration of temporary stomas.
Chronic liver disease
Chronic liver disease is a progressive disease with different stages and severity (and therefore multiple sequelae). The burden allocated to each individual included their most severe sequela, with the remaining time allocated to less severe sequelae (Sequelae, health states and durations for gastrointestinal disorders.). For example, a person with end-stage liver disease would be allocated 2 months for this sequela. Any remaining time prior to end-stage disease would be allocated as decompensated cirrhosis.
The sex proportions of liver transplants due to chronic liver disease in that state used the same proportions as ABDS 2015, which were derived from Western Australian liver transplant data, which was then applied to the national population, based on the assumption that the prevalence rate is the same across all states and territories.
Data from database linked hospitalisations and deaths data from the NIHSI AA v0.5 were also used to estimate a persons-to-separations ratio for chronic liver disease, by stage of disease progression. These ratios were applied to national hospital separations, by broad age group, to derive national prevalence.
Chronic liver disease patients were identified as those with a principal or additional diagnosis of the condition or from procedures particular to chronic liver disease, based on expert advice. Estimates of the number of individuals that received a liver transplant due to chronic liver disease for the reference year were obtained from the Australian and New Zealand Liver Transplant Registry.
Inflammatory bowel disease
Inflammatory bowel disease is a chronic condition predominantly comprised of 2 diseases: Crohn’s disease and ulcerative colitis, with a small proportion as unclassified inflammatory bowel disease. The health state devised by the GBD 2017, and applied by the ABDS 2018, is inclusive of the remittent and recurring nature of the disease, surgery and any potential long‑term effects such as stoma. The health loss was assumed to apply for the whole year.
Hospitalisations data were not used to estimate the prevalence of inflammatory bowel disease as it only captures patients undergoing procedures related to the condition. Instead, estimates were based on results of the Sydney inflammatory bowel disease cohort study (Selinger et al. 2013), which derived prevalence using hospitals and gastroenterologists’ data. This is the most recently published study that used a similar method to other relevant studies that were done previously (Gearry et al. 2006; Studd 2016). The study draws on a population that is generalisable to the Australian population.
Gastro-oesophageal reflux disease
Gastro-oesophageal reflux disease (GORD) (which includes hiatal hernias) is largely a chronic disease treated in response to symptoms. The major symptoms include heartburn, acid reflux and difficulty swallowing. This condition was first included in the ABDS 2011 due to the reportedly high morbidity.
No health loss is assigned to mild symptomatic GORD as it is of short duration. It is assumed that people with moderate or severe GORD (that is, those experiencing symptoms more than once a week) will seek medical help from a general practitioner (GP).
Total prevalence of moderate or severe GORD was based on published estimates by Harrison et al. (2017), which estimated the national prevalence of GORD as 6.9%. This prevalence rate was applied to the population aged 15 and over. Secondary data sources were required to inform age–sex distributions.
Age and sex distributions for GORD in males and females aged 15 and over were derived from the study by Miller et al. (2015), which estimated age‑specific rates of general practice consultations with a GORD diagnosis in 2012–14.
For GORD in males and females aged under 15, prevalence rates were derived from general practice data for the year 2008–09 (as used in the ABDS 2011 and ABDS 2015) and applied to the 2018 Australian Estimated Residential Population, as more recent data was unavailable at the time of the study.
Functional gastrointestinal disorders
Functional gastrointestinal disorders have not been included in previous Australian or GBD studies until the ABDS 2011 and is also included in the ABDS 2015 and ABDS 2018. Functional gastrointestinal disorders are common disorders characterised by persistent and recurring gastrointestinal symptoms. To avoid bias and over-counting in morbidity estimates, only medically confirmed cases, or cases determined using a validated collection instrument, experiencing health loss were counted. This is best captured through the Rome III criteria (Rome Foundation 2006), which impose strict criteria that must be met for functional symptoms to be classed as pathological.
As there were limited updated data available on the prevalence rates of functional gastrointestinal disorders, the method used in the ABDS 2018 was similar to that used in the ABDS 2011 and in the ABDS 2015 (described below).
There are no robust community-based data on prevalence classified by the Rome III criteria for Australia, and overseas studies based on Rome III have been based on specific populations that cannot be generalised to Australia. As a result, the ABDS 2018 estimates were based on the study by Boyce and others (2006) which provided adult prevalence rates for specific functional gastrointestinal disorders in the Penrith region in New South Wales. This used a validated questionnaire for the Rome II criteria which are very similar to the criteria for the 2 sequelae modelled in the ABDS 2018, as in the ABDS 2011. Estimates for children and adolescents were based on international studies by Chitkara and others (2005) and Helgeland and others (2009).
Distribution of the severity for each sequela were based on the European Disability Weight Study (Haagsma et al. 2015) which estimated disability weights consistent with the GBD 2010 health states and disability weights for functional heartburn, reflux and irritable bowel syndrome for use in European burden of disease studies.
Other gastrointestinal disorders
YLD was derived indirectly by applying the YLD:YLL ratio for all gastrointestinal disorders (except gastro-oesophageal reflux and functional gastrointestinal disorders) combined to the YLL for other gastrointestinal disorders.
Sub-national estimates
Estimates for 2015 and 2018 derived directly from the NHMD were broken down by state/territory, and by remoteness area and socioeconomic group by applying the 2016 ASGS remoteness areas and the 2016 SEIFA population-based IRSD quintiles to the Statistical Area Level 2 recorded in hospital separations data. For 2011 and 2003 estimates, 2011 ASGS remoteness areas and SEIFA population-based quintiles were used.
For estimates based on epidemiological studies (gastro-oesophageal reflux, inflammatory bowel disease, functional gastrointestinal disorders), breakdowns were derived by applying prevalence rates to the relevant population.
2015, 2011 and 2003 estimates
The same methods used for 2018 estimates were used to estimate point prevalence for each of the diseases in the gastrointestinal disorders group for 2015, 2011 and 2003, using 2015, 2011 and 2003 hospitalisations data and populations.
Indigenous specific estimates
Indigenous estimates were derived using the same methods and data sources as described above for national estimates for 2018, 2011 and 2003. Estimates based on hospital separations data were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
Due to lack of evidence on the rates of gastroduodenal disorders in Indigenous Australians compared with non-Indigenous Australians, the same factor to inflate hospitals incidence for physician diagnosed gastroduodenal disorders used for the national population (Sung et al. 2009) was also used for the Indigenous population.
For chronic liver disease, terminal and decompensated estimates were obtained by applying ratios derived from the NIHSI AA v0.5 and Western Australian linked data to national estimates.
Indigenous prevalence for inflammatory bowel disease, gastro-oesophageal reflux and functional gastrointestinal disorders was obtained by applying the national distribution directly to the Indigenous population for 2018, 2011 and 2003. This assumes the underlying rate is the same between the Indigenous and non-Indigenous populations, and between the two time points.
References
Boyce P, Talley N, Burke C & Koloski N 2006. Epidemiology of the functional gastrointestinal disorders diagnosed according to Rome II criteria: an Australian population-based study. Internal Medicine Journal 36:28–36.
Chitkara D, Rawat D & Talley N 2005. The epidemiology of childhood recurrent abdominal pain in western countries: a systematic review. The American Journal of Gastroenterology 100:1868–75.
Gearry RB, Richardson A, Frampton CM, Collett JA, Burt MJ, Chapman BA et al. 2006. High incidence of Crohn’s disease in Canterbury, New Zealand: results of an epidemiologic study. Inflammatory Bowel Disease 12(10):936–43.
Haagsma J, Maertens de Noordhout C, Polinder S, Vos T, Havelaar A, Cassini A et al. 2015. Assessing disability weights based on the responses of 30,660 people from four European countries. Population Health Metrics 13:10.
Harrison C, Henderson J, Miller G & Britt H 2017. The prevalence of diagnosed chronic conditions and multimorbidity in Australia: A method for estimating population prevalence from general practice patient encounter data. PLoS One, 12(3), e0172935.
Helgeland H, Flagstad G, Grøtta J, Vandvik P, Kristensen H & Markestad T 2009. Diagnosing pediatric function abdominal pain in children (4–15 years old) according to the Rome III criteria: results from a Norwegian prospective study. Journal of Pediatric Gastroenterology and Nutrition 49(3):309–15.
Miller G, Wong C, Pollack A. 2015. Gastro-oesophageal reflux disease (GORD) in Australian general practice patients. The Royal Australian College of General Practitioners 44(10):701–4.
NCCH (National Centre for Classification in Health) 2010. The International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM), Australian Classification of Health Interventions (ACHI) and Australian Coding Standards (ACS). 7th Edition. Sydney: NCCH.
NZMOH (New Zealand Ministry of Health) 2012. Ways and means: a report on methodology from the New Zealand Burden of Diseases, Injuries and Risk Factors Study, 2000–2016. Wellington: NZMOH.
Rome Foundation 2006. Rome III diagnostic criteria for FGIDs. Rome: Rome Foundation.
Selinger CP, Andrews J, Dent OF, Norton I, Jones B, McDonald C et al. 2013. Cause-specific mortality and 30-year relative survival of Crohn’s disease and ulcerative colitis. Inflammatory Bowel Diseases 19(9):1880–8.
Studd C, Cameron G, Beswick L, Knight R, Hair C, McNeil J et al. 2016. Never underestimate inflammatory bowel disease: high prevalence rates and confirmation of high incidence rates in Australia. Journal of Gastroenterology and Hepatology 31(1), 81–86.
Sung J, Kuipers E & El-Serag H 2009. Systematic review: the global incidence and prevalence of peptic ulcer disease. Alimentary Pharmacology and Therapeutics 29(9):938–46.
Disease list
For the ABDS 2015 and the ABDS 2018, vision disorders included in the vision loss envelope were reported separately by the type of vision disorder. This is different from previous Australian burden of disease studies (including the ABDS 2011), where vision loss was reported as a single envelope estimate (excluding vision loss due to diabetic retinopathy and trachoma in the ABDS 2011).
Prevalence estimates for vision loss due to diabetic retinopathy and trachoma were calculated separately under endocrine disorders and infections (see methods for these respective disease groups). Vision loss due to injuries is included in other vision disorders.
Sequelae and health states
Sequelae and health states for hearing & vision disorders are listed in the table below. As only permanent hearing & vision disorders are estimated, health loss is assumed to apply for the whole year.
Table 4.14: Sequelae and health states for hearing & vision disorders
|
Disease |
Sequela |
ABDS 2018 health |
|---|---|---|
|
Hearing loss |
Hearing loss |
103, 104, 105, 106, 108, |
|
Other hearing & vestibular disorders |
Ear pain |
15 |
|
Vertiginous symptoms due to other hearing & vestibular disorders |
207 |
|
|
Age-related macular degeneration |
Vision loss |
113, 114, 115, 116 |
|
Cataract & other lens disorders |
Vision loss |
113, 114, 115, 116 |
|
Glaucoma |
Vision loss |
113, 114, 115, 116 |
|
Refractive errors |
Vision loss |
113, 114, 115 |
|
Other vision disorders |
Vision loss |
114, 116, 117 |
(a) See ABDS 2018 health states.
Prevalence estimation
Hearing loss
In the ABDS 2018, hearing loss refers to all clinically confirmed chronic hearing loss, irrespective of the cause. Short-term hearing loss for otitis media is included under infectious diseases.
Data sources
Where possible, the ABDS 2018 gave priority to clinically confirmed data over self-reported surveys. As there is no single source of clinically confirmed hearing loss for all age groups in Australia, the overall national prevalence of hearing loss was estimated using 3 main data sources:
- For ages 0–24, prevalence was derived from the Australian Hearing 2018 demographics report summary tables of people aged 26 and under with a clinically diagnosed hearing impairment who were fitted with a hearing aid (Australian Hearing 2018).
- Prevalence for people aged 25–54 was derived from the NHS 2017–18 (ABS 2019) for the number of people reporting hearing loss, and partial or complete deafness
- For ages 55 and over, prevalence was derived from published estimates of clinically assessed hearing loss in the Blue Mountains Hearing Study (Mitchell et al. 2011) as in the ABDS 2011 and the ABDS 2015 as more recent data were unavailable at the time of the study.
Prevalence estimation by age and sex
Prevalence estimates in 10-year age groups by sex were derived from the Blue Mountains Hearing Study. To derive 5-year age groups, sex-specific proportions of total hearing loss in 5-year age groups from the NHS 2017–18 (ABS 2019) were applied to ages 55 and over.
Prevalence by severity
The same severity distribution as used in the ABDS 2011 and the ABDS 2015 (derived from the GBD 2010 for high‑income regions) was used, as it was the most updated publicly available data at the time of the study.
Due to limited Australian data for tinnitus prevalence by hearing severity, analyses of self‑reported results from a United States National Health Interview Survey were used (Hoffman & Reed 2004). This was favoured as prevalence was obtained specifically from hearing impaired individuals. As this was a self-reported study, hearing levels were not clinically assessed. To determine severity, the Gallaudet Hearing Scale (used in the survey) was mapped to the GBD 2010 lay descriptions for each health state. The severity distribution for tinnitus is in Table 4.15.
The tinnitus estimates were subtracted from the total hearing loss estimates to calculate estimates for hearing impairment without tinnitus.
Table 4.15: Proportion of tinnitus in hearing impaired population, by age, sex and severity level
| Proportion of tinnitus within each severity level of hearing loss (%) | ||||
|
Age group (years) |
Mild |
Moderate |
Severe |
Profound |
|
Males |
|
|
|
|
|
18–24 |
38.9 |
29.2 |
54.1 |
0.0 |
|
25–44 |
21.8 |
35.2 |
35.3 |
37.2 |
|
45–64 |
29.9 |
29.7 |
39.4 |
42.6 |
|
65 and over |
16.5 |
21.9 |
26.7 |
26.4 |
|
Females |
|
|
|
|
|
18–24 |
18.8 |
47.0 |
73.3 |
0.0 |
|
25–44 |
35.6 |
40.4 |
54.8 |
45.3 |
|
45–64 |
29.8 |
34.2 |
47.2 |
32.2 |
|
65 and over |
21.7 |
28.9 |
33.6 |
30.1 |
Other hearing & vestibular disorders
Other hearing disorders were also calculated using self-reported data from the NHS 2017–18 (ABS 2019). It was assumed that conditions classified under Meniere disease would result in vertigo, and those classified as other ear diseases would result in ear pain.
Estimates of Meniere disease by sex were obtained from the NHS 2017–18 (ABS 2019) (age estimates were not available due to high RSEs). To obtain age estimates, the age distribution was obtained using hospitalisations of Meniere disease in 2018 by age and sex from the NHMD, and then applied to the total prevalence derived from the NHS 2017–18 (ABS 2019). As well, the NHS did not report on Very remote areas, so prevalence estimates were adjusted to account for Very remote areas.
To estimate burden from ear pain due to other hearing and vestibular disorders, estimates were obtained from the NHS 2017–18 (ABS 2019) by age and sex. Age groups that had high RSEs (0–19 and 70 and over) were estimated using population sex-specific proportions to obtain 5-year age groups.
Refractive error and cataract & other lens disorders
The prevalence rate of uncorrected refractive error and cataract and other lens disorders, by 10-year age groups from age 40, was obtained from the Melbourne Visual Impairment Project. Estimates were modelled in 5-year age groups using proportions from the ABDS 2003 (Begg et al. 2007).
Prevalence was estimated from age 40 and over for cataract and other lens disorders only due to the nature of this condition. Due to limited information on refractive error prevalence in people aged under 60, prevalence rates from the ABDS 2003 were used. These rates were originally obtained from estimates from Weih et al. (2000). The sex distribution was based on the Australian population, assuming no sex differentiation in these conditions.
Severity distributions for refractive error was obtained from the Melbourne Visual Impairment Project and modelled to account for inconsistencies. It was assumed there was no differentiation by sex, and that refractive error would not be the primary cause of blindness (< 3/60) in individuals with severe visual impairment, based on expert advice.
Severity distributions for vision impairment due to cataract were obtained from published Melbourne Visual Impairment Project data analyses. The average population-weighted prevalence estimates by severity across each age group from the Melbourne Visual Impairment Project estimates were applied to all age groups.
Glaucoma
Prevalence for glaucoma was estimated only from age 40, as primary open angle glaucoma is rare in people aged under 40.
The prevalence rate of vision impairment due to glaucoma for people aged 60–89 in 10-year age groups was obtained from the Melbourne Visual Impairment Project, as in the ABDS 2011 (AIHW 2016), due to limitations in reliable data. Extrapolation based on the exponential curve was used to determine rates in younger age groups. Trend analysis was used to determine prevalence rates in 5-year age groups.
Sex distribution was based on the Australian population, assuming no sex differentiation in glaucoma. The severity distribution of glaucoma, by age, was derived from published Melbourne Visual Impairment Project based estimates (VanNewkirk et al. 2001). Due to sampling artefacts in the study, proportions were considered inconsistent with the disease model of glaucoma severity by age. Instead, estimates by age were pooled, and the pooled severity distribution was used across all age groups.
Age-related macular degeneration
Prevalence of age-related macular degeneration was estimated only from age 50 and over, due to the nature of this condition.
The prevalence rate of age-related macular degeneration for people aged 65–89 was obtained from the Melbourne Visual Impairment Project, as in the ABDS 2011 and ABDS 2015, due to limitations in reliable data. Prevalence rates in younger age groups (that is, 50–64) were obtained through extrapolation and trend analyses. Proportions in 5-year age groups were obtained from estimates in the Access Economics vision loss reports of prevalence of bilateral age-related macular degeneration in the better eye, based on prevalence derived from the Blue Mountains Eye Study (Deloitte Access Economics 2011).
Sex distribution was based on the Australian population, assuming no sex differentiation in age-related macular degeneration. Severity distributions were obtained from published Melbourne Visual Impairment Project data analyses. Based on expert advice, it was assumed that the ratio of clinical age-related macular degeneration-to-vision loss due to age‑related macular degeneration was the same as the ratio of mild vision loss-to-blindness due to age‑related macular degeneration. This also assumed the same progression rate through each severity.
Other vision disorders
As in the ABDS 2011 and the ABDS 2015, vision loss due to other vision disorders was based on the proportions of vision loss caused by residual disorders described in Vision loss in Australia (Taylor et al. 2005). The prevalence of vision loss due to trachoma was subtracted from the estimate to avoid double-counting.
The age and sex distribution from the AHS 2011–12 (ABS 2013) for visual disturbances and blindness was then applied to the overall estimate. Estimates for people aged 0–9 and 90 and over were attained using population proportions.
Estimates for blindness were based on the proportion in Vision loss in Australia, adjusted for trachoma and diabetic retinopathy. Experts advised that most of these are probably due to trauma.
Estimates for moderate and near-sighted vision loss were based on the assumption that the ratio of mild-to-moderate vision loss in Weih et al. (2000) is the same as that for near‑sighted-to-moderate vision loss for other vision disorders.
Sub-national estimates
Sub-national estimates were apportioned from the national estimates based on age- and sex‑specific ratios from the NHS 2017–18 data.
2015, 2011 and 2003 estimates
Due to limitations in reliable data, the same severity distribution and proportions of individuals with hearing loss and vision loss used in 2018 estimates were used for national 2003, 2011 and 2015 estimates.
Indigenous specific estimates
Hearing loss
The overall Indigenous prevalence of hearing loss was estimated using 2 main data sources:
- For ages 0–24, prevalence was derived from the Australian Hearing 2018 report summary tables of Indigenous Australians aged 26 and under with a clinically diagnosed hearing impairment who were fitted with a hearing aid (Australian Hearing 2018).
- Prevalence for Indigenous Australians aged 25 and over was derived from measured hearing loss data from the 2018–19 NATSIHS.
The overall severity distribution for Indigenous estimates was derived from data in the Northern Territory outreach audiology data collection report (AIHW 2020), with the national tinnitus splits then applied.
The Indigenous prevalence rates for 2018 were applied to the 2003 and 2011 Indigenous ERPs to derive prevalence estimates for 2003 and 2011.
Vision loss
Estimates for vision loss in the Indigenous population were estimated from published results from the National Eye Health Survey 2016 for 2018, and the Indigenous Eye Health Survey 2008 for both 2011 and 2003. These estimates provide robust data for vision loss specific to the Indigenous population. Published estimates were reported by state, remoteness category and broad age categories and apportioned into 5 year age groups and sex either using Indigenous population or national age-sex distributions for each cause.
Broad severity distributions were obtained from the National Indigenous Eye Health Survey and applied to the Indigenous prevalence estimates by age and sex. The total number of vision loss by cause was compared to the proportion of total vision loss in the Indigenous population, to ensure the derived prevalence estimates were consistent with that expected in the Indigenous population.
Trachoma
Vision loss caused by trachoma was measured in the Indigenous population only. The proportion of total vision loss due to trachoma by broad severity groups were obtained from the National Indigenous Eye Health Survey 2008 for both 2011 and 2003. The age distribution of trachomatous scarring prevalence was applied to low vision estimates and the prevalence of trichiasis for blindness.
The progression from mild vision loss to blindness occurs quickly in individuals with persistent trachoma infection; therefore expert advice on the appropriate severity distribution was sought on modelled estimates. In absence of other data, the ratio of moderate: severe vision loss by age from the ABDS 2003 (Begg et al. 2007) was applied to the broad severity categories.
References
ABS 2013. Australian Health Survey: users’ guide, 2011–13. ABS cat. no. 4363.0.55.001. Canberra. Viewed 20 March 2016.
ABS 2019. National Health Survey: users’ guide, 2017–18. ABS cat. no. 4363.0. Canberra: ABS. Viewed 19 May 2021.
AIHW 2016. Australian Burden of Disease Study 2011: methods and supplementary material. Australian Burden of Disease Study series no. 5. Cat. no. BOD 6. Canberra: AIHW.
AIHW 2020. Hearing health outreach services for Aboriginal and Torres Strait Islander children in the Northern Territory: July 2012 to December 2019. Cat. no. IHW 228. Canberra: AIHW.
Australian Hearing 2018. Demographic details of young Australians aged less than 26 years with a hearing loss, who have been fitted with a hearing aid or cochlear implant at 31 December 2018. Sydney: Australian Hearing.
Begg S, Vos T, Barker B, Stevenson C, Stanley L & Lopez AD 2007. The burden of disease and injury in Australia 2003. Cat. no. PHE 82. Canberra: AIHW.
Deloitte Access Economics 2011. Eyes on the future: a clear outlook on age-related macular degeneration. Sydney: Macular Degeneration Foundation. Viewed 24 September 2014.
Hoffman H & Reed G 2004. Epidemiology of Tinnitus In: Snow J(ed). Tinnitus: Theory and management. Ontario, Canada: BC Decker 16-41.
Mitchell P, Gopinath B, Wang J, McMahon C, Schneider J, Rochtchin E et al. 2011. Five-year incidence and progression of hearing impairment in an older population. Ear and Hearing 32(2):251–7.
Taylor H, Keeffe J, Vu H, Wang J, Rochtchina E, Pezzullo M et al. 2005. Vision loss in Australia. Medical Journal of Australia 182:565–8.
VanNewkirk, M. R., Weih, L., McCarty, C. A., & Taylor, H. R. (2001). Cause-specific prevalence of bilateral visual impairment in Victoria, Australia: the Visual Impairment Project. Ophthalmology 108(5), 960-967.
Weih LM, VanNewkirk MR, McCarty CA & Taylor HR 2000. Age-specific causes of bilateral visual impairment. Archives of Ophthalmology 118:264–9.
Sequelae and health states
The sequelae and health states assigned to infant and congenital disorders are listed in the table below. The majority of sequelae are chronic, so health loss was assumed to apply for the whole year. Durations for acute sequelae are described in the relevant sections.
Table 4.16: Sequelae and health states for infant & congenital conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Pre-term birth & low birthweight complications |
Acute complications due to pre-term & low birthweight complications |
54 |
|
|
Neurodevelopment impairment due to pre-term & low birthweight complications(b) |
213, 214, 215, 216, 217, 218 |
|
Birth trauma & asphyxia |
Neurodevelopment impairment due to birth trauma & asphyxia(b) |
216, 217, 218 |
|
Cerebral palsy |
Neurodevelopment impairment due to cerebral palsy |
213, 214, 215 |
|
Neonatal infections |
Acute complications due to neonatal infections |
3 |
|
Other disorders of infancy |
Other disorders of infancy |
54 |
|
Neural tube defects |
Incontinence due to neural tube defects |
48 |
|
|
Motor impairment due to neural tube defects |
213, 214, 215 |
|
|
Neurodevelopment impairment due to neural tube defects(b) |
218 |
|
Brain malformations |
Neurodevelopment impairment due to brain malformations(b) |
216, 217, 218 |
|
Cardiovascular defects |
Congenital cardiovascular defects untreated |
33 |
|
|
Heart failure due to congenital cardiovascular defects(c) |
31, 32, 33 |
|
Cleft lip and/or palate |
Disfigurement due to cleft lip/palate |
201, 202 |
|
|
Speech problems due to cleft lip/palate |
212 |
|
Gastrointestinal malformations |
Acute complications due to gastrointestinal malformations |
194 |
|
|
Incontinence due to anorectal atresia |
48 |
|
Urogenital malformations |
Urogenital malformations |
192, 262 |
|
Down syndrome |
Intellectual disability due to Down syndrome(b) |
99, 100, 101, 102, 243 |
|
Other chromosomal abnormalities |
Intellectual disability due to chromosomal abnormalities(b) |
99, 100, 101, 102, 243 |
|
Other congenital conditions |
Other congenital conditions |
YLL:YLD ratio |
(a) See ABDS 2018 health states.
(b) Part of the intellectual disability envelope.
(c) Part of the heart failure envelope.
Prevalence estimation
The key data sources to estimate prevalence of infant & congenital conditions are listed below.
Table 4.17: Key data sources for infant & congenital conditions
|
Data source |
Related diseases |
|---|---|
|
National Hospital Morbidity Database |
Neonatal infections, other disorders of infancy, pre-term & low birthweight complications (acute) |
|
National Mortality Database |
Cerebral palsy |
|
Western Australian Registry of Developmental Anomalies (WARDA) |
Neural tube defects (acute), cardiovascular defects (acute), gastrointestinal malformations (acute), urogenital malformations (acute) |
|
Cerebral Palsy Register |
Cerebral palsy |
|
Intellectual Disability Exploring Answers (IDEA) database |
Intellectual disability envelope conditions |
|
National Perinatal Data Collection |
Pre-term & low birthweight complications |
|
DisMod II |
Neural tube defects, gastrointestinal malformations |
Western Australian Registry of Developmental Anomalies
For congenital abnormalities, prevalent cases for the acute sequelae were obtained from the Western Australian Registry of Developmental Anomalies (WARDA) for 2015, 2011 and 2003. Linear regression was used to derive the prevalent cases for 2018. The live birth prevalence rate for Western Australia was estimated by dividing the number of cases by Western Australia live births. This rate was then applied to the Australian live births to derive national estimates.
DisMod II
Two groups of congenital abnormalities—neural tube defects and gastrointestinal malformations—used DisMod II to obtain point prevalence for long-term sequelae, the same outputs from DisMod II were used for 2015 and 2018, adjusted for population change. Parameters used as inputs to DisMod II were:
- an incidence rate derived from WARDA for live births
- an assumed remission rate of 0
-
a case fatality rate obtained from previous burden of disease studies or derived from incidence and the NMD.
Intellectual disability in the ABDS 2018
Intellectual disability (also referred to as cognitive impairment) is a sequela of multiple conditions in the infant and congenital disease group, including for:
- pre-term birth and low birthweight complications
- birth trauma and asphyxia
- brain malformations (including FASD)
- neural tube defects
- Down syndrome
- other chromosomal abnormalities.
Details on the methods for prevalence and severity distribution of the intellectual disability envelope are provided in the 'Mental and substance use disorders' section.
Pre-term birth & low birthweight complications
Prevalence of neurodevelopmental impairment due to pre-term birth & low birthweight complications was derived from the intellectual disability envelope. Data on the number of live births by gestational age was obtained from the National Perinatal Data Collection (NPDC) for 2016–2018 combined. This was used to derive the proportion of live births in each preterm category—extremely, very and late pre-term. For each severity, 50% of cases were modelled with motor impairment and 50% of cases with motor and cognitive impairment, based on assumptions by Blencowe et al. (2013).
Estimates for acute complications due to pre-term births & low birthweight were based on incidence of hospital separations in the 2018 calendar year. Any admissions to hospital that included the corresponding ICD-10-AM codes as diagnosis were counted.
The duration of acute complications was derived from the median length of stay for level III neonatal intensive care units for Australian and New Zealand Neonatal Network registrants in 2017, by gestational age (Chow et al. 2019). The durations were:
- extremely pre-term (20–27 weeks): 108 days
- very pre-term (28–31 weeks): 55 days
- late pre-term (32–36 weeks): 20 days.
Birth trauma & asphyxia
Prevalence of neurodevelopmental impairment due to birth trauma & asphyxia was derived from the intellectual disability envelope. The severity distribution for birth trauma & asphyxia was derived from the NHMD 2018–19 using specific severity codes for hypoxic ischaemic encephalopathy of newborn (P91.61–P91.63).
Cerebral palsy
The key data source for cerebral palsy was the Australian Cerebral Palsy Register Report 2018 (Cerebral Palsy Alliance 2018). Incidence and mortality from cerebral palsy in 1913–2018 were estimated from the Australian Cerebral Palsy Register report and the NMD, respectively. Prevalence was adjusted for standard background mortality using the Australian life table 2016–2018 (ABS 2019).
Estimated Australian-specific severity distribution derived from the Gross Motor Function Classification System was applied to the estimates.
Table 4.18: Estimated severity distribution used for cerebral palsy, by Gross Motor Function Classification System (GMFCS) level
|
GMFCS levels |
Description |
GBD health state |
Per cent |
|
Level I |
Walks without limitations |
Motor impairment: mild |
37.0 |
|
Level II |
Walks with limitations, including long distances, balancing, running or jumping; requires use of mobility devices when first learning to walk, and may rely on wheeled mobility equipment when outside of home for travelling long distances |
Motor impairment: moderate |
25.4 |
|
Level III |
Walks with adaptive equipment assistance. Requires mobility assistance to walk indoors, while utilising wheeled mobility outdoors; can sit on own or with limited external support; and has some independence in standing transfers |
Motor impairment: moderate |
11.5 |
|
Level IV |
Self-mobility with use of powered mobility assistance. Is supported when sitting; self-mobility is limited; and likely to be transported in wheelchair |
Motor impairment: severe |
12.2 |
|
Level V |
Severe head and trunk control limitations. Requires extensive use of assisted technology and physical assistance; and to be transported in a wheelchair. |
Motor impairment: severe |
14.0 |
Source: Cerebral Palsy Alliance 2018.
Overlaps with other diseases
Cerebral palsy can be caused by a number of related conditions. Health loss due to infection, traumatic brain injuries and other cerebral accidents caused by cerebral palsy acquired post‑neonatally were captured under other disease groups (for example, injuries, infections).
The total prevalence of cerebral palsy from neonatal conditions was first determined. To ensure the total health loss due to cerebral palsy was neither over- nor under-estimated, the proportion of cerebral palsy caused by other conditions in the infant & congenital disease group (birth trauma & asphyxia and pre-term & low birthweight complications) was excluded after estimation of the YLD. Half (50%) of YLD for neonatally acquired cerebral palsy was distributed to birth trauma & asphyxia (10%) and pre-term & low birthweight complications (40%). The proportional split was determined from the studies by McIntyre et al. (2013), Badawi et al. (2005) and the NZBDS (NZMOH 2012). The remaining 50% of YLD was assigned to cerebral palsy.
Neonatal infections & other disorders of infancy
Health loss from neonatal infections & other disorders of infancy is short term. Prevalence estimates for neonatal infections & other disorders of infancy were based on hospital separations from the NHMD where these diseases were listed as either the principal or additional diagnosis. It was assumed that cases lasted on average 4 weeks.
Neural tube defects
Prevalence of neural tube defects in babies less than 1 year was sourced directly from the live birth prevalence rate derived from WARDA for 2015, 2011 and 2003. Linear regression was used to derive the prevalent cases for 2018. DisMod II was used to model prevalence for those aged over 1 using incidence, remission and case fatality inputs. The same outputs from DisMod II were used for 2015 and 2018, adjusted for population change. Prevalence estimates were then distributed into different health states using proportions from Hunt & Oakeshott (2003) (Table 4.19). The life expectancy for people with moderate or severe neural tube defects was assumed to be about 46 years (Oakeshott et al. 2015).
Table 4.19: Distribution of health states for neural tube defects
|
Health state |
Proportion of neural tube defects cases (%) |
|---|---|
|
Incontinence |
80.0 |
|
Mild motor impairment |
30.0 |
|
Moderate motor impairment |
27.0 |
|
Severe impairment |
|
|
Motor impairment only |
21.5 |
|
Motor plus cognitive impairment |
21.5 |
Source: Hunt & Oakeshott 2003.
Brain malformations
Prevalence of neurodevelopmental impairment due to brain malformations was derived from the intellectual disability envelope (see ‘Mental and substance use disorders’). For moderate and severe brain malformations, prevalence rates were modelled to account for a life expectancy of about 40 years.
Congenital cardiovascular defects
Congenital cardiovascular defects were modelled to include an acute sequela (cardiovascular defects prior to surgery) with a duration of 1 year, and a chronic sequela (heart failure due to congenital cardiovascular defects). Heart failure due to congenital cardiovascular defects was modelled under the heart failure envelope (see Cardiovascular diseases in Disease specific methods - morbidity).
Cleft lip and/or palate
It was assumed that all children born in Australia with cleft lip and/or palate are treated surgically (or at least have commenced a first surgical intervention) within the first year of life (Royal Children’s Hospital Melbourne 2020). As such, it was assumed all cases have disfigurement (level 2) until surgery at about 9 months. Post-surgical treatment, it was estimated that 5% of cases continue to have moderate disfigurement (level 2) and 10% mild disfigurement (level 1). It was assumed that 85% of cases have no residual disability (GBD 2013 Collaborators 2015).
Post-surgery, it was estimated that 19% of cases aged 1–9, and 4% of cases aged 10–14 will experience speech problems, and these are largely resolved by age 15 (Sell et al. 2001).
Live birth prevalence rates of cleft lip and/or palate were derived from published WARDA data for 1980–2015. People born with cleft lip and/or palate were assumed to have the same life expectancy as the general population. Therefore, as an enduring condition, the prevalence rate for a given age in 2018 was obtained from live birth prevalence rate during the relevant birth year. Where WARDA data were unavailable for an age cohort, the prevalence rate from the closest reference year was used.
Gastrointestinal malformations
Gastrointestinal malformations include various congenital anomalies, but anorectal and oesophageal atresia were chosen as the primary sequel for inclusion. An untreated (pre‑surgical) health state in the first year of life was assumed to be equivalent to the GBD 2010 health state: severe abdominopelvic problems.
DisMod II was used to model prevalence for those aged over 1 using incidence, remission and case fatality inputs. The same outputs from DisMod II were used for 2015 and 2018, adjusted for population change. It was assumed 44.6% of people with anorectal malformations experience faecal incontinence (Stenström et al. 2014). The proportion of anorectal malformations was derived from WARDA data published in the annual report of the International Clearinghouse for Birth Defects Surveillance and Research for 2014 (ICBDSR 2014). For the first year of life, it was assumed faecal incontinence only occurred for 6 months after surgical intervention.
Urogenital malformations
The sequelae for urogenital malformations included hypospadias, undescended testicles, and other urogenital malformations.
Children with hypospadias often have surgery at 6–18 months, after which the associated health burden is negligible. As such, hypospadias was assumed to be asymptomatic. For other urogenital malformations, it was proposed the health burden is equivalent to the health state for mild abdominopelvic pain. The proportion of hypospadias and undescended testis was derived from the NHMD 2018–19, and it was assumed 30% of other urogenital malformations were symptomatic (mild abdominopelvic pain).
It was assumed people born with urogenital malformations have the same life expectancy as the general population and zero remission; therefore, the live birth prevalence rate (from WARDA) was held constant and applied to the national population by sex and age groups.
Down syndrome
The major sequela for Down syndrome was intellectual disability, which was modelled as part of the intellectual disability envelope. Due to the reduced life expectancy in people with Down syndrome (Day et al. 2005; Glasson et al. 2003), prevalence rates were modelled to account for a life expectancy of about 70 years.
Other chromosomal abnormalities
The major long-term disabling sequela for other chromosomal abnormalities was intellectual disability, which was modelled as part of the intellectual disability envelope.Other congenital conditions
A YLD:YLL ratio was derived using the combined YLD and YLL from cardiovascular defects, cleft lip and/or palates, gastrointestinal malformations and urogenital malformations. This ensured there was no overlap with the health loss captured for conditions under the intellectual disability envelope. This ratio was applied to the fatal burden of other congenital conditions to derive the corresponding YLD.
Sub-national estimates
National estimates were apportioned into each remoteness area, socioeconomic group and state/territory based on proportions of the respective disease obtained from the NHMD 2018–19 data.
2015, 2011 and 2003 estimates
Estimates for infant & congenital conditions used a similar method, with data sourced for 2015, 2011 and 2003.
Indigenous specific estimates
Where possible, prevalence estimates for the Indigenous population for 2018, 2011 and 2003 were obtained from the same data sources as used for national prevalence estimates, using the same methods. Exceptions to this are described below.
Indigenous estimates based on hospital separations data (that is, neonatal infections, other disorders of infancy, acute preterm low birth weight complications) were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
For congenital abnormalities, Indigenous:total population rate ratios were derived from the WA Registry of Developmental Anomalies (for birth anomalies, e.g. for neural tube defects) or the NHMD (where surgical interventions, e.g. for cleft lip/palate) applied to national prevalence rates.
The Australian Cerebral Palsy Register (Cerebral Palsy Alliance 2018) reported 5.8% of people with cerebral palsy were born from mothers of Aboriginal and/or Torres Strait Islander status. This proportion was 3.5% in 2011 and 2003. These proportions were applied to national estimates to derive the Indigenous prevalence for cerebral palsy.
For conditions included in the intellectual disability envelope (see above), Indigenous prevalence estimates were calculated using Indigenous:non-Indigenous rate ratios (see Indigenous estimates section in ‘Mental and substance use disorders’). Due to lack of data, 2003 and 2018 estimates were calculated using 2011 rates, applied to reference populations.
References
ABS (Australian Bureau of Statistics) 2019. Life tables, 2016–2018. Canberra: ABS. Viewed 1 July 2020.
Badawi N, Felix JF, Kurinczuk JJ, Dixon G, Watson L, Keogh JM et al. 2005. Cerebral palsy following term newborn encephalopathy: a population-based study. Developmental Medicine and Child Neurology 47(5):293–8.
Blencowe H, Lee ACC, Cousens S, Bahalim A, Narwal R, Zhong N et al. 2013. Pre-term birth: associated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatric Research 74:17–34.
Cerebral Palsy Alliance 2018. Report of the Australian Cerebral Palsy Register, birth years 1995–2012. Sydney: Cerebral Palsy Alliance.
Chow SSW, Creighton P, Chambers GM, Lui K 2019. Report of the Australian and New Zealand Neonatal Network 2017. Sydney: ANZNN.
Day SM, Strauss DJ, Shavelle RM & Reynolds RJ 2005. Mortality and causes of death in persons with Down syndrome in California. Developmental Medicine and Child Neurology 47(03):171–6.
Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD & Bittles AH 2003. Comparative survival advantage of males with Down syndrome. American Journal of Human Biology 15(2):192–5.
ICBDSR (International Clearinghouse for Birth Defects Surveillance and Research) 2014. Annual report 2014. Rome: International Centre on Birth Defects–ICBDSR Centre.
GBD (Global Burden of Disease Study) 2013 Collaborators 2015. Supplement to: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 386(10010): S1–1868.
Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD & Bittles AH 2003. Comparative survival advantage of males with Down syndrome. American Journal of Human Biology 15(2):192–5.
Oakeshott P, Reid F, Poulton A, Markus H, Whitaker RH & Hunt GM 2015. Neurological level at birth predicts survival to the mid-40s and urological deaths in open spina bifida: a complete prospective cohort study. Developmental Medicine & Child Neurology 57:634–8.
Hunt GM & Oakeshott P 2003. Outcome in people with spina bifida at age 35: prospective community based cohort study. BMJ 326:1365–6.
McIntyre S, Blair E, Badawi N, Keogh J & Nelson K 2013. Antecedents of cerebral palsy and perinatal death in term and late pre-term singletons. Obstetrics and Gynaecology 122(4):869–77.
NZMOH (New Zealand Ministry of Health) 2012. Ways and means: a report on methodology from the New Zealand Burden of Diseases, Injuries and Risk Factors Study, 2000–2016. Wellington: NZMOH.
Royal Children’s Hospital Melbourne 2020. Cleft lip and palate. Melbourne: Royal Children’s Hospital. Viewed 29 October 2021.
Sell D, Grunwell P, Mildinhall S, Murphy T, Cornish TA, Bearn D et al. 2001. Cleft lip and palate care in the United Kingdom—the Clinical Standards Advisory Group (CSAG) Study. Part 3: speech outcomes. Cleft Palate–Craniofacial Journal 38(1):30–7.
Stenström P, Clementson Kockum C, Emblem R, Arnbjornsson E & Bjornland K 2014. Bowel symptoms in children with anorectal malformation: a follow-up with a gender and age perspective. Journal of Pediatric Surgery 49:1122–30.
Sequelae and health states
A list of sequelae and health states assigned to each infectious disease is included in the table below. As infectious disease data are generally measured in terms of incident cases, prevalence estimates were produced by applying a duration of health loss. These durations were sourced from previous Australian or GBD studies.
Table 4.20: Sequelae and health states for infectious diseases
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
HIV/AIDS |
HIV/AIDS |
10, 11, 12, 208 |
|
Tuberculosis |
Tuberculosis |
16 |
|
Syphilis |
Congenital syphilis |
3 |
|
|
Primary syphilis |
1 |
|
|
Secondary syphilis |
2 |
|
|
Tertiary syphilis |
217 |
|
Chlamydia |
Chlamydial infection |
1 |
|
|
Infertility due to chlamydia(b) |
50, 51 |
|
|
Pelvic inflammatory disease due to chlamydia |
193, 194 |
|
Gonorrhoea |
Gonococcal infection |
1 |
|
|
Infertility due to gonorrhoea(b) |
50, 51 |
|
|
Pelvic inflammatory disease due to gonorrhoea |
193, 194 |
|
Other sexually transmitted infections |
Infertility due to other sexually transmitted infections(b) |
50, 51 |
|
|
Other sexually transmitted infections |
1 |
|
|
Pelvic inflammatory disease due to other sexually transmitted infections |
193, 194 |
|
Hepatitis A |
Acute hepatitis A |
1, 2, 3 |
|
|
Hepatitis A, relapsing |
4 |
|
Hepatitis B (acute) |
Acute hepatitis B |
2, 3 |
|
Hepatitis C (acute) |
Acute hepatitis C |
2, 3 |
|
Upper respiratory infections |
Upper respiratory infections |
1, 2 |
|
Otitis media |
Otitis media: acute |
15 |
|
|
Otitis media: chronic |
103 |
|
Lower respiratory infections |
Lower respiratory infections |
2, 3 |
|
Influenza |
Influenza |
2, 3 |
|
Diphtheria |
Diphtheria |
2, 3 |
|
Pertussis |
Pertussis, acute |
1, 2, 3 |
|
Tetanus |
Tetanus |
3 |
|
Measles |
Measles |
2, 3 |
|
Rubella |
Rubella |
1 |
|
Varicella |
Varicella |
1 |
|
Herpes zoster |
Herpes zoster |
4, 9 |
|
Mumps |
Mumps |
2, 3 |
|
Haemophilus influenzae type b |
Haemophilus influenza type b disease |
3 |
|
Pneumococcal disease |
Invasive pneumococcal disease |
3 |
|
Meningococcal disease |
Meningococcal disease |
3 |
|
Other meningitis and encephalitis |
Other meningitis and encephalitis |
3 |
|
Dengue |
Dengue fever |
1, 2, 3, 4 |
|
Ross River virus |
Ross River virus infection |
131, 4 |
|
Barmah Forest virus |
Barmah Forest virus infection |
131, 26 |
|
Malaria |
Malaria |
2, 3 |
|
Trachoma |
Blindness due to trachoma(c) |
115, 116 |
|
|
Low vision due to trachoma(c) |
113, 114 |
|
Campylobacteriosis |
Gastrointestinal infection |
5, 6, 7 |
|
Salmonellosis |
Gastrointestinal infection |
5, 6, 7 |
|
Rotavirus |
Gastrointestinal infection |
5, 6, 7 |
|
Other gastrointestinal infections |
Gastrointestinal infection |
43, 5, 6, 7 |
|
Urinary tract infections |
Urinary tract infections |
2, 3 |
(a) See ABDS 2018 health states.
(b) Part of infertility envelope.
(c) Part of vision envelope.
Prevalence estimation
The primary data sources used for infectious diseases are listed below. These data sources were often supplemented by a secondary data source (particularly the NHMD) to help estimate either the severity distribution or the age and sex distribution for each disease.
Table 4.21: Key data sources for infectious diseases
|
Data source |
Disease |
|---|---|
|
National Notifiable Diseases Surveillance System (NNDSS) |
Tuberculosis, syphilis, chlamydia, gonorrhoea, hepatitis A, hepatitis B, diphtheria, pertussis, tetanus, measles, mumps, rubella, Haemophilus influenzae type-B (Hib), pneumococcal disease, meningococcal disease, dengue, Ross River virus, Barmah Forest virus, malaria |
|
Bettering the Evaluation and Care of Health survey (BEACH) |
Upper respiratory infections, otitis media (acute), varicella, herpes zoster, lower respiratory infections, influenza, other sexually transmitted infections, urinary tract infections |
|
National Hospital Morbidity Database (NHMD) |
Other meningitis and encephalitis, otitis media (chronic) |
|
Foodborne illness in Australia: annual incidence circa 2010 (Kirk et al. 2014) |
Campylobacteriosis, salmonellosis, rotavirus, other gastrointestinal infections |
|
Modelled prevalence estimates produced by The Kirby Institute (University of New South Wales) |
HIV/AIDS, hepatitis C |
The methods for prevalence estimation are presented here by primary data source, rather than by disease as in other sections, due to the large number of individual diseases being estimated and similarities in approaches.
National Notifiable Diseases Surveillance System
Notifications to the National Notifiable Diseases Surveillance System (NNDSS) were considered to be an accurate estimate of the incidence of tuberculosis, diphtheria, tetanus, measles, mumps, rubella, Haemophilus influenzae type-b (Hib), pneumococcal disease, meningococcal disease, dengue, Ross River virus, Barmah Forest virus and malaria.
For other conditions, disease notifications represent only a proportion of the total incidence (referred to as the ‘notified fraction’). The notified fraction varies by disease, jurisdiction and period due to the influence of several factors: the pathogenicity of the organism; disease severity; changing case definitions; specificity and sensitivity of diagnostic tests; and differences in testing and reporting practices between primary care practices, laboratories and hospitals. As a result, notifications for pertussis, hepatitis A and hepatitis B were inflated in an attempt to estimate the true community incidence. These adjustment factors were based on a variety of evidence, including enhanced surveillance programs, outbreak investigation and expert advice (de Greeff et al. 2009; Kirk et al. 2014).
Enhanced disease surveillance and screening programs in target populations (particularly for sexually transmitted diseases) might result in the notification of asymptomatic infection. For burden of disease purposes, individuals who are asymptomatic are assumed to experience no health loss and are excluded from analysis. Therefore, published data from state annual surveillance reports (SA Health 2012; 2019) and enhanced surveillance studies (Fagan et al. 2013; Ressler et al. 2013) as used in the ABDS 2011 and ABDS 2015 were used to determine sex-specific adjustment factors to correct for asymptomatic notification of chlamydia and gonorrhoea. State annual surveillance reports were similarly used to determine and to distribute national syphilis notifications, by stage of disease.
Bettering the Evaluation and Care of Health
Data from the BEACH survey were used for infectious diseases where no other representative data source was available (including acute otitis media, herpes zoster, influenza, lower respiratory infections, upper respiratory infections, urinary tract infections, varicella and other sexually transmitted infections).
The number of BEACH GP encounters observed by age and sex was compared with the corresponding number of national GP consultations in each of the reference years (based on Medicare Benefits Scheme claims). This factor was then applied to the weighted number of GP consultations with specific International Classification of Primary Care Version 2+ (ICPC–2+) diagnosis codes to estimate an expected number of national GP consultations for a particular disease (using methods described by Britt et al. 2016). The extrapolated number of national consultations was used to estimate disease incidence, based on the assumption that 1 GP episode represents 1 incident case.
Where disease prevalence rates were assumed to remain constant in recent years or no other data sources could be identified to inform prevalence, the disease prevalence rates calculated for 2015 were applied to the 2018 population to attain estimates for the year 2018. This was done for otitis media, varicella, herpes zoster, lower respiratory infections, influenza and upper respiratory infections.
For urinary tract infections, BEACH data for 2015 were not available. Instead, age/sex-specific ratios were calculated between hospitalisations and BEACH data in 2011. Estimated ratios were then applied to separations data in the years 2015 and 2018 to calculate expected disease incidence in the community in those years. This assumes that the proportion of cases identified via notifications or separations data is consistent with those identified in general practices from 2010–2012.
National Hospital Morbidity Database
The NHMD was used to estimate the incidence of other meningitis and encephalitis and chronic otitis media (based on myringotomy with tube insertion procedures).
Across most infectious diseases included in the study, the NHMD was also used to estimate the number of severe cases.
Other published data sources
Published estimates were used for the remaining infectious diseases, namely:
- the incidence of gastrointestinal infectious diseases in 2010 (Kirk et al. 2014)
- the number of individuals living with human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) by age and sex (The Kirby Institute 2020)
- the annual incidence of hepatitis B and C infections (The Kirby Institute 2020)
- age-specific proportion of newly acquired Hepatitis B infection that are symptomatic (Shepard et al. 2006)
- inflation factors for emergency department presentations for pelvic inflammatory disease that do not get admitted to hospital (Goller et al. 2018)
- estimated proportions of pelvic inflammatory disease due to chlamydia, gonorrhoea and other sexually transmitted infections (Reekie et al. 2014).
Additionally, prevalence estimates for infertility were derived as part of the reproductive & maternal conditions disease group. Prevalence estimates for vision loss due to trachoma were estimated as part of the hearing & vision loss disease group.
Other infections
YLD was derived indirectly by applying the YLL-to-YLD ratio for all specified infectious diseases combined to the YLL for other unspecified infectious diseases.
Sub-national estimates
Prevalence estimates by state and territory as well as by remoteness area and socioeconomic group were calculated by applying proportions from the NHMD to national estimates.
2015, 2011 and 2003 estimates
Prevalence estimates for 2003, 2011 and 2015 were calculated from the data sources and method as described for 2018.
Indigenous specific estimates
Where possible, prevalence estimates for the Indigenous population were obtained from the same data source as used for national prevalence estimates. However, for most causes, indirect methods were used by applying rate ratios from the NHMD to the national prevalence estimates to derive Indigenous prevalence.
The same durations were applied for Indigenous estimates as used for national estimates, with the exception of untreated chronic otitis media.
National Hospital Morbidity Database (NHMD)
Indigenous estimates based on hospitalisation data were adjusted for Indigenous under-identification using standard adjustment factors outlined in Chapter 4 (see Years lived with disability (YLD)).
The Kirby Institute reports
Indigenous estimates for HIV/AIDS were based on prevalence estimates by the Kirby Institute (2020).
References
Britt H, Miller GC, Henderson J, Bayram C, Harrison C, Valenti et al. 2016. General practice activity in Australia 2015–16. General practice series no. 40. Sydney: Sydney University Press.
de Greeff S, Lugnér A, van den Heuvel D, Mooi F & de Melker H 2009. Economic analysis of pertussis illness in the Dutch population: implications for current and future vaccination strategies. Vaccine 27:1932–7.
Fagan PS, Downing SG, McCall BJ, Carroll HJ, Howard TM & Palmer CM 2013. Enhanced surveillance for gonorrhoea in two diverse settings in Queensland in the 2000s. Communicable Disease Intelligence 37(3):E253–9.
Goller JL, De Livera AM, Guy RJ, Low N, Donovan B, Law M et al. 2018. Rates of pelvic inflammatory disease and ectopic pregnancy in Australia 2009–2014: ecological analysis of hospital data. Sexually Transmitted Infections 94(7):534–41.
Kirk M, Glass K, Ford L, Brown K & Hall G. 2014. Foodborne illness in Australia: Annual incidence circa 2010. Department of Health: Canberra.
Reekie J, Donovan B, Guy R, Hocking JS, et al. 2014. Hospitalisations for pelvic inflammatory disease temporally related to a diagnosis of chlamydia or gonorrhoea: a retrospective cohort study. PLOS One 9(4):e94361.
Ressler KA, Smedley E, Spokes P, Hockey G, Nurkic A & Ferson MJ 2013. Enhanced surveillance of gonorrhoea in South Eastern Sydney. Sydney: NSW Health.
SA Health 2012. Surveillance of sexually transmitted infections and blood-borne viruses in South Australia 2011. Adelaide: SA Health.
SA Health 2019. Surveillance of STIs and BBVs in South Australia, 2018. Adelaide: SA Health.
Shepard CW, Simarrd EP, FinelliL, Fiore AE & Bell BP 2006. Hepatitis B virus infection: epidemiology and vaccination. Epidemiological Reviews 28(1): 112–125.
The Kirby Institute 2020. National update on HIV, viral hepatitis and sexually transmissible infections in Australia: 2009–2018. Sydney: Kirby Institute, University of New South Wales.
Injury perspectives for burden of disease analysis
Burden of disease studies traditionally report injury burden by external causes. The functional limitations (health states) caused by injury are described by the nature of the injury or the body part injured.
In the ABDS 2018, injury burden was reported using two perspectives—the external cause that led to the injury (for example, a road traffic accident, a fall or an accidental poisoning) and the nature of the injury (for example, a hip fracture, a traumatic brain injury or poisoning). The total burden from injury is the same for each reporting perspective and each perspective is equally comparable with the estimates for other disease groups in this study. To facilitate reporting by both perspectives, the fatal injury burden by external cause was mapped to the nature of injury causes, and the non-fatal burden by nature of injury was mapped to external causes (as described further in the following section).
Injury categories for each perspective are shown in the table below. The ICD-10 codes used to identify injury causes are shown in ABDS 2018 list of diseases, conditions and injuries.
Table 4.22: List of injury categories used in the ABDS 2018 for nature of injury and external cause of injury
|
Injury by nature |
Injury by external cause |
|---|---|
|
Traumatic brain injury |
Road traffic injuries–motorcyclists |
|
Spinal cord injury |
Road traffic injuries–motor vehicle occupants |
|
Internal & crush injury |
Road traffic injuries–pedal cyclists |
|
Poisoning |
Road traffic injuries–pedestrians |
|
Drowning & submersion injuries |
Other land transport injuries |
|
Hip fracture |
Poisoning |
|
Tibia & ankle fracture |
Falls |
|
Humerus fracture |
Fire, burns & scalds |
|
Other fractures |
Drowning |
|
Dislocations |
Other unintentional injuries |
|
Soft tissue injuries |
Suicide & self-inflicted injuries |
|
Burn injuries |
Homicide & violence |
|
Other injuries |
All other external causes of injury |
The overarching methods for estimating non-fatal burden in the ABDS 2018 are the same as for the ABDS 2011 and the ABDS 2015; however, the epidemiological inputs used to estimate injury prevalence have been updated since the ABDS 2015. The overall differences in the inputs and the impact of these on the results are described further below.
In the ABDS 2018, it is assumed that all injuries in Australia are treated. Therefore, the GBD disability weights that relate to untreated injuries were not used for estimating non-fatal burden.
Scope of non-fatal injuries
The scope of injuries is limited to those incurred from trauma. That is, for example, disability associated with surgical amputations due to a disease—or chronic conditions, such as carpal tunnel syndrome and chronic back pain or poisoning due to infections—are out of scope. Similarly, the consequences of some medical injuries are likely captured in other disease groups associated with the underlying reason for the specific intervention.
However, while the burden associated with fractures and dislocations is reported in the injury disease group, there are some known associations between physical trauma and the later development of osteoarthritis and other musculoskeletal conditions. As a result, it is likely that some portion of the post-traumatic burden of injuries is double-counted in the injuries disease group and in the musculoskeletal diseases group.
Non-fatal injuries were identified as all injuries admitted to hospital (admitted) or presented to an emergency department without hospital admission (non-admitted).
Other injuries, such as those presenting only to a GP and those for which no medical care is sought, are not captured. This approach is similar to that used for previous Australian studies, where injuries treated outside the hospital system were assumed to result in insignificant disability to warrant inclusion (Begg et al. 2007). This, however, imposes a limitation on the estimates and may warrant further investigation in future iterations if appropriate data were available.
Due to the nature of identifying injuries in the ABDS, some cases of insignificant injury will be included where they have co-occurred with injuries warranting hospital care.
Sequelae and health states
All injuries (admitted and non-admitted) were assumed to have short-term consequences. Long-term consequences were included according to the GBD 2013 methods (Haagsma et al. 2016).
The model inputs for durations, remission, and excess mortality by admission status (admitted and non-admitted) for each injury sequela were based on the GBD 2013 methods. These inputs are shown in the table below.
Table 4.23a: Model inputs for short–term injuries, health states, and durations by admission status (admitted and non-admitted)
|
Cause sequelae |
Short–term health state identifier(a) |
Short–term admitted duration (years) |
Short–term non–admitted duration (years) |
|---|---|---|---|
|
Burn (non-airway) - minor |
144 |
0.077 |
0.038 |
|
Burn (non-airway) - severe |
146 |
0.164 |
0.164 |
|
Airways burn |
149 |
0.077 |
0.077 |
|
Dislocation - shoulder joint |
153 |
0.170 |
0.148 |
|
Dislocation - shoulder other |
184 |
0.178 |
0.132 |
|
Dislocation - hip |
151 |
0.110 |
0.085 |
|
Dislocation - knee |
152 |
0.110 |
0.112 |
|
Dislocations - other |
154 |
0.178 |
0.132 |
|
Drowning short-term |
155 |
0.011 |
0.005 |
|
Fracture - neck of femur |
162 |
0.216 |
0.197 |
|
Fracture - other than neck of femur |
165 |
0.233 |
0.167 |
|
Crush injury |
150 |
0.167 |
0.030 |
|
Severe chest injury |
187 |
0.148 |
0.115 |
|
Abdominal /pelvic injuries |
187 |
0.058 |
0.058 |
|
Fracture - humerus |
156 |
0.175 |
0.142 |
|
Fracture - patella |
167 |
0.359 |
0.258 |
|
Fracture - clavicle or scapula |
156 |
0.175 |
0.142 |
|
Fracture - face bone |
157 |
0.126 |
0.101 |
|
Fracture - foot bone |
158 |
0.134 |
0.099 |
|
Fracture - hand bone |
160 |
0.099 |
0.110 |
|
Fracture - pelvis |
169 |
0.167 |
0.148 |
|
Fracture - pelvis (coccyx) |
184 |
0.233 |
0.205 |
|
Fracture - radius or ulna |
171 |
0.132 |
0.112 |
|
Fracture - sternum / ribs |
174 |
0.148 |
0.115 |
|
Fracture - vertebral column |
175 |
0.233 |
0.205 |
|
Fracture - other |
176 |
0.167 |
0.148 |
|
Amputation of finger/s excl thumb |
134 |
0.500 |
0.500 |
|
Amputation of thumb |
135 |
0.500 |
0.500 |
|
Amputation of both arms |
137 |
0.500 |
0.500 |
|
Amputation of one arm |
237 |
0.500 |
0.500 |
|
Amputation of toe |
139 |
0.500 |
0.500 |
|
Amputation of one leg |
140 |
0.500 |
0.500 |
|
Amputation of both legs |
142 |
0.500 |
0.500 |
|
Injured nerves |
177 |
0.170 |
0.099 |
|
Injury to eyes |
179 |
0.123 |
0.137 |
|
Superficial injuries |
184 |
0.115 |
0.049 |
|
Open wound |
184 |
0.099 |
0.049 |
|
All other injuries |
184 |
0.008 |
0.005 |
|
Poisoning short-term |
185 |
0.011 |
0.005 |
|
Soft tissue injuries |
154 |
0.178 |
0.132 |
|
SCI at neck - complete severe |
190 |
0.500 |
0.500 |
|
SCI at neck - incomplete severe |
215 |
0.500 |
0.500 |
|
SCI at neck - incomplete moderate |
214 |
0.500 |
0.500 |
|
SCI at neck - mild |
213 |
0.077 |
0.077 |
|
SCI below neck - complete severe |
188 |
0.500 |
0.500 |
|
SCI below neck - incomplete severe |
215 |
0.500 |
0.500 |
|
SCI below neck - incomplete moderate |
214 |
0.500 |
0.500 |
|
SCI below neck - mild |
213 |
0.077 |
0.077 |
|
Fracture - tibia or fibula |
167 |
0.359 |
0.258 |
|
Fracture - ankle |
167 |
0.359 |
0.258 |
|
TBI ST minor |
246 |
0.101 |
0.096 |
|
TBI ST moderate-severe |
180 |
0.110 |
0.074 |
|
TBI skull fracture |
173 |
0.126 |
0.101 |
(a) See ABDS 2018 health states.
Table 4.23b: Model inputs for long–term injuries, proportions and excess mortality by admission status (admitted and non-admitted)
|
Cause sequelae |
Long-term health state identifier(a) |
Long–term admitted proportion |
Long–term non–admitted proportion |
Long-term Mortality risk ratio(b) |
|---|---|---|---|---|
|
Burn (non-airway) - minor |
145 |
1 |
1 |
45+ 2.1 |
|
Burn (non-airway) - severe |
147 |
1 |
1 |
45+ 1.3 |
|
Dislocation - hip |
151 |
1 |
1 |
1 |
|
Dislocation - knee |
152 |
1 |
0 |
1 |
|
Dislocations - other |
154 |
1 |
0 |
1 |
|
Drowning short-term |
155 |
1 |
0 |
1 |
|
Fracture - neck of femur |
163 |
1 |
1 |
Under 50 1.0 |
|
Fracture - other than neck of femur |
176 |
1 |
1 |
1 |
|
Crush injury |
150 |
1 |
1 |
5.23 |
|
Severe chest injury |
187 |
1 |
0 |
1 |
|
Abdominal /pelvic injuries |
187 |
1 |
1 |
1 |
|
Fracture - humerus |
156 |
1 |
1 |
1 |
|
Fracture - patella |
167 |
1 |
1 |
1 |
|
Fracture - clavicle or scapula |
156 |
1 |
0 |
1 |
|
Fracture - face bone |
157 |
1 |
0 |
1 |
|
Fracture - foot bone |
158 |
0 |
1 |
1 |
|
Fracture - hand bone |
160 |
1 |
0 |
1 |
|
Fracture - pelvis |
169 |
1 |
1 |
1 |
|
Fracture - pelvis (coccyx) |
184 |
1 |
1 |
1 |
|
Fracture - radius or ulna |
171 |
1 |
0 |
1 |
|
Fracture - sternum / ribs |
174 |
1 |
1 |
1 |
|
Fracture - vertebral column |
175 |
1 |
1 |
1 |
|
Fracture - other |
169 |
1 |
1 |
1 |
|
Amputation of finger/s excl thumb |
134 |
1 |
1 |
1 |
|
Amputation of thumb |
135 |
1 |
1 |
1 |
|
Amputation of both arms |
137 |
1 |
1 |
1 |
|
Amputation of one arm |
237 |
1 |
1 |
1 |
|
Amputation of toe |
139 |
1 |
1 |
1 |
|
Amputation of one leg |
140 |
1 |
1 |
1 |
|
Amputation of both legs |
142 |
1 |
1 |
1 |
|
Injured nerves |
178 |
1 |
0 |
1 |
|
Poisoning short-term |
216 |
1 |
0 |
1 |
|
SCI at neck - complete severe |
190 |
1 |
1 |
Under 60 5.03 |
|
SCI at neck - incomplete severe |
215 |
1 |
1 |
Under 60 5.03 |
|
SCI at neck - incomplete moderate |
214 |
1 |
1 |
|
|
SCI below neck - complete severe |
188 |
1 |
1 |
Under 60 2.72 |
|
SCI below neck - incomplete severe |
215 |
1 |
1 |
Under 60 2.72 |
|
SCI below neck - incomplete moderate |
214 |
1 |
1 |
Under 60 5.03 |
|
Fracture - tibia or fibula |
167 |
1 |
1 |
1 |
|
Fracture - ankle |
167 |
1 |
1 |
1 |
|
TBI minor |
181 |
1 |
1 |
1 |
|
TBI moderate-severe |
182 |
0.75 |
0.75 |
2.18 |
|
TBI skull fracture |
173 |
1 |
1 |
1 |
(a) See ABDS 2018 health states.
(b) Sourced from Haagsma and others (2015).
Some exceptions were that Australian-specific direct evidence was used to calculate YLD for two injuries:
- spinal cord injury—a severity distribution based on (unpublished) Australian trauma care data
- burns—excess mortality from a study in Western Australia (Duke et al. 2015).
Prevalence estimation
Prevalence estimation is undertaken separately for short- and long-term consequences.
Key data sources to estimate prevalence of injuries were the NHMD and the National Non‑admitted Patient Emergency Department Care Database (NNAPEDC). The prevalence of long-term consequences was modelled for ABDS 2015 using DisMod II, based on incident cases derived from the NHMD and the NNAPEDC. Estimates for 2018 were generated from the 2015 modelled estimates using incidence and mortality for the years 2015 to 2017.
Injury cases were identified in the NHMD based on separations in the 2003, 2011, 2015 and 2018 calendar years. The NNAPEDC for 2013–14 to 2018–19 was used to estimate incidence of non-admitted cases using information about the diagnosis.
Overview of method for estimating non-fatal injury burden
The calculation of non-fatal injury burden requires the estimation of 4 prevalence components: the prevalence of short-term admitted and non-admitted injuries, and of long‑term admitted and non-admitted injuries.
Short-term injury burden is directly associated with the incidence of injury and duration of the health consequences, while long-term burden is directly related to the incidence of injury, the remission of the health consequences and the associated excess mortality.
YLD was estimated for each injury sustained in an incident. That is, where a motor vehicle occupant sustains multiple injuries—for example, a traumatic brain injury, plus a fractured pelvis and traumatic arm amputation from a road traffic accident—the YLD associated with each injury in the ABDS disease list was counted. To maintain consistency for YLD, the total sum of these YLD were attributed to a single external cause (in this case, a road traffic injury to a motor vehicle occupant).
Following on from this example, each injury sustained will have some duration of short-term health loss—based on the duration inputs—followed by long-term health loss—based on remission (or percentage likelihood of sustaining long-term health loss) and the excess mortality associated with the injury.
The YLD is the prevalence weighted by severity (that is, prevalence multiplied by the disability weight) associated with the short- and long-term health states for each injury sequela. The total YLD for any injury is the sum of the YLD for each of the 4 weighted prevalence components.
The YLD is the prevalence weighted by severity (that is, prevalence multiplied by the disability weight) associated with the short- and long-term health states for each injury sequela. The total YLD for any injury is the sum of the YLD for each of the 4 weighted prevalence components.
- short-term admitted prevalence is the product of the short-term admitted incidence and the duration of each injury sequela.
- short-term non-admitted prevalence is obtained by inflating the short-term admitted incidence, using an inflation ratio (to account for cases presenting to the emergency department but which were not admitted) and the duration of short-term non-admitted injury sequela.
- long-term admitted and non-admitted prevalence: The modelling done for ABDS 2015 using DisMod II (modelled on the short-term admitted incidence, the remission and excess mortality of each sequela) has been adapted for the ABDS 2018 study because, of the inputs for DisMod II, only the admitted incidence may have changed. The ratio of long term to short-term prevalence from 2003, 2011 and 2015 is used to calculate ABDS 2018 estimates for long-term prevalence from updated short-term prevalence for those years. Estimates for long-term prevalence in 2018 are calculated by adding the incidence from 2015, 2016 and 2017 (adjusted for all-cause mortality) to the long-term prevalence in 2015. The same methods are used for long-term non-admitted prevalence.
Short-term sequelae
To capture all injuries that presented to a hospital, both admitted cases and non-admitted cases were counted.
Admitted cases
Short-term admitted injury cases were identified as all separations where the primary reason for admission was injury. All diagnoses of injury in that separation were used to calculate the burden as each diagnosis represents an injury that has resulted in health loss. Injuries reported as additional diagnoses in records where the principal diagnosis was not an injury were excluded.
Injury separations were identified from records in the NHMD where the principal diagnosis was in the ICD-10-AM range S00–T75, T79, T80, T81 and T88. Burden was derived from all injuries in this range of codes recorded in these separations, either as the principle diagnosis or the additional diagnoses.
Multiple mentions of the same injury were counted only once per episode of care. Where there were multiple reports of different levels of severity in the same hospital episode of care, the most severe injury was counted over the less severe mentions of injury. For example, if a severe burn and a minor burn were reported in a single episode of care, only the severest injury is counted for estimating YLD.
Burden due to medical injuries in the ICD-10AM range T82–T87 are assumed to be captured in other disease groups by the underlying reason for the transplant or amputation.
Only separations for acute types of care were counted. This excludes injuries presenting to hospitals, for example, for rehabilitation. It is assumed that the burden associated with injuries requiring rehabilitation is sufficiently estimated using the methods described below for long‑term consequences of injuries.
Hospital separations where the person died were excluded as the non-fatal burden from these injuries was assumed to be of short duration, while the fatal burden was captured in YLL. There was no adjustment for repeat admission for the same injury.
Estimating non-admitted injuries
To quantify injury cases presenting to emergency departments but not admitted to hospital, injuries presenting to emergency departments were sourced from the NNAPEDC database for 2013–14 to 2018–19. This data set included a diagnosis variable.
As diagnosis data were provided in a number of classifications, only jurisdictions that had more than 95% of emergency department records coded to an ICD-10 AM classification were included in the analysis. Hence, all records from New South Wales and Western Australian hospitals were excluded. Further exclusions were made for records not coded to an ICD‑10 AM classification. In total, around 48.4% of records were found to be useable for the purposes of the ABDS—that is, after excluding records for New South Wales and Western Australia (as stated earlier), other records not coded to a version of ICD-10 AM, non‑emergency visits and records not identified as admitted or non-admitted. Of the useable records, 27.1% had a principal diagnosis of injury.
An inflation ratio was used to estimate the number of non-admitted injury cases. The ratio of non-admitted to admitted cases for each injury sequela (by age and sex) was calculated using the NNAPEDC. The ratio reflects the excess or absence of non-admitted cases compared with admitted cases. A ratio of less than 1 suggests that there were fewer non‑admitted cases than admitted cases, and a ratio greater than 1 suggests that there were more non-admitted cases than admitted cases. For example, an inflation ratio of 1.2 suggests that for every 10 admitted cases there were 12 non-admitted cases, while a ratio of 0.2 suggests that for every 10 admitted cases there 2 non-admitted cases. The ratio was applied to cases of admitted injuries (from the NHMD).
Diagnosis information is available in the NNAPEDC database starting from 2013–14. As a result, inflation ratios were calculated using the data having diagnosis information (2013–14 to 2018–19) and applied similarly to all data years in the study. A broad assumption in this method is that admission and non-admission rates over the period 2013–14 to 2018–19 were applicable to 2003, 2011, 2015 and 2018.
A limitation of this method is the reliability of the inflation ratios; that is, these data have not been rigorously assessed to understand how well the diagnosis predicts admission. The data were very broadly assessed for limited types of injuries to determine some level of consistency with expectation. For example, the proportion of all hip fractures that resulted in admission was high (above 95%) as would be expected. As well, it should be noted that NNAPEDC data are not necessarily representative of presentations to emergency departments that are not in scope for the collection—for example, in small hospitals or remote areas. In 2014–15, it was estimated that about 88% of emergency occasions were reported in the NNAPEDC (AIHW 2015).
Figure 4.1: ABDS 2018 Short-term injury prevalence – Steps and data sources for calculating prevalence of injury sequelae
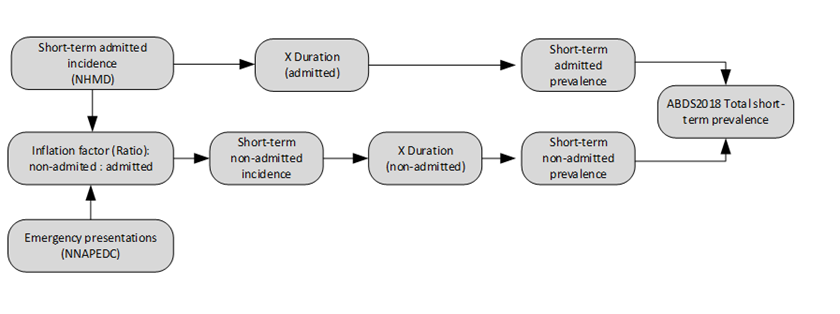
Long-term sequelae
Long-term consequences of injury reflect the functional consequences that persist more than 1 year after the injury. In the ABDS 2015, the respective national all-cause mortality rates and populations were used for DisMod II calculations for each ABDS reference period (2003, 2011 and 2015) for injuries with long-term consequences. The point prevalence was estimated using DisMod II, based on the proportion of admitted and non-admitted incident cases expected to have long-term consequences, the expected extent of health loss (defined as the remission) and expected patterns of mortality (the excess mortality described by rate/risk ratios) for the ABDS 2015. The DisMod II output of prevalent number of cases for each year was used to represent the likely current prevalence of long-term injury sequelae. Note that the amount of extra modelling required in DisMod II was minimal as the availability of unit record level data in Australia, and its use as the single source for injury prevalence, enabled highly accurate data inputs at very fine levels.
The ratio between short and long term prevalence calculated in the ABDS 2015 was applied to the short term injury prevalence calculated in the ABDS 2018 to estimate the long term injury prevalence for the 2003, 2011 and 2015 reference years.
Figure 4.2: ABDS 2018 long-term injury prevalence for 2003, 2011, 2015 – Steps and data sources for calculating prevalence of injury sequelae
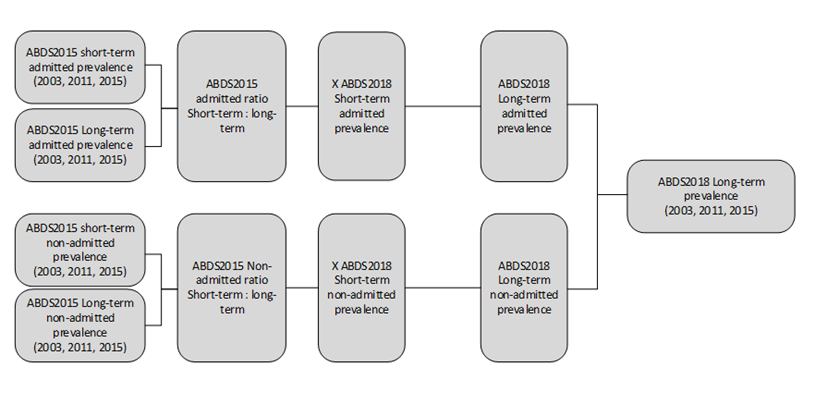
The values for these inputs for each long-term injury sequela were sourced from Haagsma et al. (2015). The inputs estimated from this source are presented in model inputs for durations, remission, and excess mortality by admission status (admitted and non-admitted).
Estimates for long-term prevalence in 2018 are calculated by adding the incidence from 2015, 2016 and 2017 (adjusted for all-cause mortality) to the long-term prevalence in 2015.
Figure 4.3: ABDS 2018 long-term injury prevalence for 2018 – Steps and data sources for calculating prevalence of injury sequelae

The GBD 2013 used a method to avoid double-counting of injury; for example, where post‑trauma effects manifest as other musculoskeletal conditions. This method was not implemented in the ABDS 2015 or the ABDS 2018 (see box below for more detail).
Box 4.1: ABDS diseases associated with previous injury
In the GBD 2013, a method was implemented to avoid double-counting of the burden of diseases associated with previous injury, such as the long-term musculoskeletal conditions resulting from previous trauma. Specifically, the method involved deducting the long-term sequelae of fractures, dislocations, and contusions due to injuries from the disease ‘other musculoskeletal conditions’ (GBD 2013 Collaborators 2015).
There was insufficient detail in the GBD methods paper to implement a similar approach in the ABDS 2018. As a result, the ABDS 2018 estimates may include some double-counting of the musculoskeletal sequelae of injury; that is, the burden of the long-term effects of trauma from injury may be counted in injuries and in musculoskeletal conditions.
With limited available detail on the GBD methodology, the literature was explored to better understand the types and extent of injuries associated with musculoskeletal conditions to help inform a suitable process to avoid this double-counting. The literature review was brief but raised further questions around the relevance of deducting the injury sequelae specifically from other musculoskeletal conditions, as opposed to from specific musculoskeletal conditions.
Given the complexity of the relationships between these causes, further work is required to develop methods to suitably reduce potential double-counting of the burden associated with these causes. This was out of scope for this study.
Conversion to external cause
Injury YLD were calculated according to the nature of the injury and then converted to external cause using matrices that describe the relationship between the injury and the external cause.
The matrices were derived directly from the NHMD using the principal diagnosis and the first reported external cause. Each matrix was calculated using age- and sex- specific cross‑tabulations of injury diagnosis and external cause, and provides a mapping of the total YLD by nature of injury categories to external cause categories.
As the matrix is derived using admitted cases only (there is no external cause in the NNAPEDC), it is assumed that the external cause of non-admitted injuries follows a similar pattern to that for admitted injuries. It is possible that the relationship between external cause and injury differs, depending on whether or not the injury resulted in admission. This method could be further refined using state-based non-admitted data comprising external cause and injury to develop more accurate matrices for non-admitted injuries.
It was also assumed that patterns of external causes giving rise to particular injuries is the same nationally; that is, the matrices have not been calculated specifically for sub-national populations.
Sub-national estimates
Sub-national estimates were largely derived directly using the same methods as those used for national estimates. This was helped by the availability of unit record data in the NHMD.
For injury cases obtained from the NHMD, sub-national estimates were derived for 2015 and 2018 by applying the 2016 ASGS remoteness areas and 2016 SEIFA population-based IRSD quintiles to the SA2 recorded in hospital separations data. For 2011 and 2003 estimates, 2011 ASGS remoteness areas and SEIFA population-based quintiles were used. The same inflation ratios were applied to sub‑national data.
The long-term national prevalence was apportioned into each state/territory, remoteness area and socioeconomic group based on the age–sex distribution of the short-term admitted incidence of injuries.
For all sub-national estimates, particularly for remoteness areas and socioeconomic groups, if there was insufficient information in the admitted injury records for ascribing a remoteness area or socioeconomic group, the record was excluded for generating models to distribute the remaining prevalence components (non-admitted short-term, and admitted and non‑admitted long-term prevalence).
2015, 2011 and 2003 estimates
The approach used to estimate 2015, 2011 and 2003 prevalence was the same as that used for 2018 estimates. The prevalence of short-term and long-term sequelae was calculated using the same methods.
Indigenous specific estimates
Indigenous estimates of non-fatal injury burden used the same methods as for the national estimates for 2018, 2011 and 2003.
For short-term prevalence, Indigenous cases of short-term injury from the NHMD were adjusted for under-identification using standard adjustment factors from hospital data quality studies undertaken by the AIHW (see Methodological choices specific to Indigenous estimates). The national inflation factors used to adjust for non-admitted injuries were applied to the adjusted Indigenous separations (see Adjusting for non-admitted injuries above).
Long-term injury prevalence was estimated using long-term/short-term ratios derived from the national study and applying them to the indigenous short-term injury estimates.
The conversion of YLD by nature of injury to external cause used indigenous specific age-sex matrices.
References
AIHW 2015. Emergency department care 2014–15: Australian hospital statistics. Health services series no. 65. Cat. no. HSE 168. Canberra: AIHW.
Begg S, Vos T, Barker B, Stevenson C, Stanley L & Lopez AD 2007. The burden of disease and injury in Australia 2003. Cat. no. PHE 82. Canberra: AIHW.
Duke JM, Boyd JH, Rea S, Randall SM & Wood FM 2015. Long-term mortality among older adults with burn injury: a population-based study in Australia. Bulletin of World Health Organization 93:400–6.
GBD (Global Burden of Disease Study) 2013 Collaborators 2015. Supplement to: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013: The Lancet 386(10010): S1–1868.
Haagsma J, Maertens de Noordhout C, Polinder S, Vos T, Havelaar A, Cassini A et al. 2015. Assessing disability weights based on the responses of 30,660 people from four European countries. Population Health Metrics 13:10.
Haagsma JA, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany EC et al. 2016. Annex to: The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Injury Prevention 22:3–18 (online supplementary material). Viewed 17 October 2017.
Sequelae and health states
Sequelae and health states assigned to kidney and urinary conditions are shown in the table below. Asymptomatic chronic kidney disease is defined as chronic kidney disease stages 1–2 and stage 3 (without anaemia). End-stage kidney disease is defined as stage 5 chronic kidney disease.
Table 4.24: Sequelae, health states and duration for kidney & urinary conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
Duration |
|---|---|---|---|
|
Chronic kidney disease |
Asymptomatic chronic kidney disease |
262 |
. . |
|
Anaemia due to stage 3 chronic kidney disease(b) |
195, 196, 197 |
12 months |
|
|
Stage 4 chronic kidney disease |
41 |
12 months |
|
|
Anaemia due to stage 4 chronic kidney disease(b) |
195, 196, 197 |
12 months |
|
|
End-stage kidney disease on dialysis |
43 |
12 months |
|
|
End-stage kidney disease after transplant |
42 |
12 months |
|
|
Untreated end-stage kidney disease |
22 |
5.5 months |
|
|
Enlarged prostate |
Enlarged prostate |
47 |
12 months |
|
Kidney stones |
Kidney stones |
193 |
2 weeks |
|
Interstitial nephritis |
Interstitial nephritis |
2, 3 |
7 days, 14 days |
|
Other kidney and urinary diseases |
Other kidney and urinary diseases |
. . |
. . |
(a) See ABDS 2018 health states.
(b) Part of the anaemia envelope.
Anaemia envelope
Anaemia due to chronic kidney disease is part of the anaemia envelope. As anaemia can result from several conditions, the sum of anaemia from various diseases cannot exceed the total experienced within the population. The definitions for the severity of anaemia in the GBD 2013 used those described in the study by Kassebaum et al. (2014). These were applied to people with chronic kidney disease and anaemia. Specifically, the definitions used were for all those aged 5 and over (excluding pregnant women). See the section on methods for blood & metabolic disorders for more information on the methods used to estimate the anaemia envelope.
Prevalence estimation
Chronic kidney disease
The primary data source used to estimate prevalence of chronic kidney disease (with and without anaemia) was the biomedical data available in the AHS 2011–12, while the primary data source to estimate prevalence of end-stage kidney disease was the Australia and New Zealand Dialysis and Transplant Registry 2018 (ANZDATA). Stages of chronic kidney disease in the AHS 2011–12 were determined by combining the participants’ estimated glomerular filtration rate results with their albumin creatinine ratio results as described in Cardiovascular disease, diabetes and chronic kidney disease, Australian facts: prevalence and incidence (AIHW 2014).
Stages 1 and 2 chronic kidney disease
The prevalence of stages 1 and 2 chronic kidney disease was estimated as described in Cardiovascular disease, diabetes and chronic kidney disease, Australian facts: prevalence and incidence (AIHW 2014). The prevalence for these stages were given an asymptomatic health state with a disability weight of 0.
Stage 3 chronic kidney disease and anaemia due to stage 3 chronic kidney disease
The prevalence of stage 3 chronic kidney disease was estimated from measured data from the AHS 2011–12. To estimate prevalence in the year 2018, the AIHW analysis of trends in stages 3–5 chronic kidney disease prevalence from the 1999–2000 AusDiab compared with the AHS 2011–12 in the broad age groups was used (AIHW 2018). The age and sex distribution was further refined using the age and sex of people who were hospitalised for N18.3 in 2018.
The proportion of people with mild and moderate anaemia was derived from biomedical data available in the AHS 2011–12, with no updated biomedical data available in the NHS 2014–15. Since no severe anaemia due to stage 3 chronic kidney disease was reported in the AHS, the proportion of people with severe anaemia in stage 3 chronic kidney disease from the GBD 2013 (GBD 2013 Collaborators 2015) was used instead. It is important to note that the GBD proportions might not be reflective of high-income countries such as Australia.
Stage 4 chronic kidney disease and anaemia due to stage 4 chronic kidney disease
The prevalence of stage 4 chronic kidney disease was also estimated from measured data from the AHS 2011–12, using the number of people with stages 4 and 5 chronic kidney disease. To estimate prevalence in 2018, similarly to stage 3, the estimate was based on trends for stages 3–5 chronic kidney disease from the 1999–2000 AusDiab compared with the AHS 2011–12. To estimate those with only stage 4 chronic kidney disease, the stages 4 and 5 estimate was used minus the number of people with end-stage kidney disease (stage 5 only) sourced from the ANZDATA.
It was not possible to break down the combined chronic kidney disease stages 4 and 5 data in the AHS 2011–12 by anaemia status, due to small numbers. The severity distribution of mild, moderate and severe anaemia due to stage 4 chronic kidney disease was sourced from the GBD 2013 (GBD 2013 Collaborators 2015).
The age and sex distribution was based on the age and sex of people who were hospitalised for N18.4 in 2018.
End-stage kidney disease treated with dialysis or transplant
Registry data from the Australia and New Zealand Dialysis and Transplant Registry in 2018 was used to determine the prevalence of end-stage kidney disease treated by dialysis or transplant.
Untreated end-stage kidney disease
People with untreated end-stage kidney disease were those not receiving kidney replacement therapy, although they might be receiving palliative treatments. The prevalence of people with untreated end-stage kidney disease was estimated by projecting incidence rates from 1997 to 2013 ANZDATA/NDI linked data to the reference year 2018. The 5-year age group prevalence was estimated using the distribution in 2013 ANZDATA/NDI linked data.
Survival was estimated using an analysis of New South Wales and Western Australian linked hospital and mortality data, by age and sex (AIHW 2014a), which indicated that the mean survival time for people with untreated end-stage kidney disease was approximately 5.5 months.
Enlarged prostate
Enlarged prostate includes cases of benign prostatic hypertrophy and excludes prostate cancer.
Prevalence was estimated using hospitalisations with a diagnosis of enlarged prostate diagnosis (N40) in 2018 from the NHMD. This includes men admitted for surgery or for other reasons, which are both assumed to indicate substantial health loss, due to hospitalisation’s being required. Admissions where there is also a diagnosis of prostate cancer (C61) were excluded.
Ratios of persons-to-separations derived from the National Health Services Information Analysis Asset (NIHSI AA v0.5) were used to adjust national NHMD data for potential readmissions and hospital transfers, to obtain prevalence of the number of men with enlarged prostate in 2018. The ratios were determined using 7 years of data (admitted patient data between 1 July 2010 and 30 June 2017), assuming that the condition is chronic. Health loss was assumed to apply for the entire year. The same ratios were also applied to NHMD data for 2003, 2011 and 2015 prevalence estimates using a 7-year lookback.
Kidney stones
Kidney stones include cases of urolithiasis of the kidney, ureter and lower urinary tract.
Point prevalence was estimated by applying a duration of 2 weeks, based on the NZBDS, to the incident cases of kidney stones—that is, the number of hospitalisations with a diagnosis of kidney stones (N20–N21) in 2018 from the NHMD. As this is an acute condition, each separation was assumed to be a case.
Interstitial nephritis
Interstitial nephritis is a condition that can lead to a variety of non-specific systemic symptoms (including vomiting, fever, rashes and malaise) and can cause discomfort and difficulty with daily activities. Interstitial nephritis can be acute or chronic in nature, with untreated chronic conditions ultimately leading to end-stage kidney disease. For the ABDS 2018, burden due to interstitial nephritis was from acute cases only. Burden from chronic interstitial nephritis is captured under chronic kidney disease.
Burden due to nephritis was estimated using a combination of data from the NHMD and the GBD 2016. Point prevalence of severe cases was estimated by applying a duration of 2 weeks to hospitalised cases, with a principal diagnosis of interstitial nephritis (N10–N12) in 2018. Non‑hospitalised cases was estimated using the ratio of severe:non-severe cases of interstitial nephritis from the GBD 2016. This indicated that nearly three-quarters of all interstitial nephritis cases are severe, which for the ABDS 2018 were assumed to represent hospitalised cases. Point prevalence for non-hospitalised cases was estimated by applying a 7-day duration of health loss to calculated estimates.
Other kidney and urinary diseases
YLD was derived indirectly by applying the YLD:YLL ratio for kidney stones to the YLL for other kidney and urinary diseases.
Sub-national estimates
Prevalence estimates by state and territory, remoteness area and socioeconomic group were derived directly from the same data source as the national estimates.
2015, 2011 and 2003 estimates
Estimates of end-stage kidney disease, kidney stones, interstitial nephritis and enlarged prostate were taken directly from the same data source, using the same method to produce prevalence estimates for 2003, 2011 and 2015.
For stages 3 and 4 chronic kidney disease (without anaemia), prevalence estimates for 2011 were derived from the AHS 2011–12. For 2003, as for 2015 and 2018, the estimate was based on trends for stages 3–5 chronic kidney disease from the 1999–2000 AusDiab compared with the AHS 2011–12. The same severity distributions used in 2018 for stages 3 and 4 chronic kidney disease with anaemia were also applied to the 2015, 2011 and 2003 estimates.
The ratio of the prevalence of end-stage kidney disease treated by dialysis or transplant to the prevalence of stage 3 chronic kidney disease and stage 4 chronic kidney disease in 2011 was used to estimate prevalence in 2003, due to lack of biomedical measurement data consistent with the 2011 method.
As the codes used to estimate the age and sex distributions from hospitalisations data were not in use in 2003, the 2011 age and sex distributions from hospitalisations were applied to the 2003 estimates.
Indigenous specific estimates
The same methods and data sources were used to derive Indigenous estimates for kidney and urinary diseases, except that trend data for chronic kidney disease prevalence were not available for Indigenous Australians. Instead, ratios of treated end-stage kidney disease to stage 4 and stage 3 CKD for 2011 were applied to treated end-stage kidney disease data for 2003 and 2018 to estimate the prevalence of stage 3 and 4 CKD for those reference years. Indigenous data were directly available from the Australia and New Zealand Dialysis and Transplant Registry and the NHMD. Biomedical data for stage 3 CKD and anaemia and stage 4 CKD was sourced from the AATSHIS 2012–13.
Estimates based on hospital separations data (enlarged prostate and kidney stones) were adjusted for under-identification using standard adjustment factors (see Chapter 4 and appendix tables C3 and C4).
The national severity distributions for anaemia were used for 2018, 2011 and 2003 Indigenous estimates.
References
AIHW 2014. Cardiovascular disease, diabetes and chronic kidney disease, Australian facts: prevalence and incidence, Cardiovascular, diabetes and chronic kidney disease series no. 2. Cat. no. CDK 2. Canberra: AIHW.
AIHW 2018. Chronic kidney disease prevalence among Australian adults over time, Cardiovascular, diabetes and chronic kidney disease series no. 6. Cat. no. CDK 6. Canberra: AIHW.
GBD 2013 Collaborators 2015. Supplement to: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 386(10010): S1–1868.
Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R et al. 2014. A systematic analysis of global anemia burden from 1990 to 2010. Blood 123:615–24.
The majority of morbidity estimates were based on methods used for the ABDS 2015, except for eating disorders.
Sequelae and health states
Sequelae and health states assigned to mental and substance use disorders are shown below. Durations (where relevant) and assumptions are outlined in relevant subsections.
Table 4.25: Sequelae and health states for mental and substance use disorders
| Disease | Sequela | ABDS 2018 health state identifier(a) |
|
|---|---|---|---|
|
Depressive disorders |
Dysthymia |
262, 86 |
|
|
Major depressive disorder |
262, 86, 87, 88 |
||
|
Anxiety disorders |
Anxiety disorders |
262, 83, 84, 85 |
|
|
Bipolar affective disorder |
Bipolar disorder |
87, 89, 90 |
|
|
Alcohol use disorders |
Alcohol dependence |
235, 262, 73, 74, 75 |
|
|
Drug use disorders (excluding alcohol) |
Amphetamine dependence |
236, 262, 80 |
|
|
|
Cannabis dependence |
244, 262, 79 |
|
|
|
Cocaine dependence |
245, 262, 81 |
|
|
|
Opioid dependence |
251, 262, 82 |
|
|
Schizophrenia |
Schizophrenia |
91, 92 |
|
|
Depressive disorders |
Dysthymia |
262, 86 |
|
|
Major depressive disorder |
262, 86, 87, 88 |
||
|
Anxiety disorders |
Anxiety disorders |
262, 83, 84, 85 |
|
|
Bipolar affective disorder |
Bipolar disorder |
87, 89, 90 |
|
|
Alcohol use disorders |
Alcohol dependence |
235, 262, 73, 74, 75 |
|
|
Drug use disorders (excluding alcohol) |
Amphetamine dependence |
236, 262, 80 |
|
|
|
Cannabis dependence |
244, 262, 79 |
|
|
|
Cocaine dependence |
245, 262, 81 |
|
|
|
Opioid dependence |
251, 262, 82 |
|
|
Schizophrenia |
Schizophrenia |
91, 92 |
|
|
Eating disorders |
Anorexia nervosa |
93 |
|
|
Bulimia nervosa |
94 |
||
|
Autism spectrum disorders |
Childhood autism |
98 |
|
|
Attention deficit hyperactivity disorder |
Asymptomatic |
262 |
|
|
Attention deficit hyperactivity disorder |
95 |
||
|
Conduct disorder |
Asymptomatic |
262 |
|
|
Conduct disorder |
96 |
||
|
Intellectual disability |
Idiopathic & other intellectual disability(b) |
100, 101, 102, 243, 99 |
|
|
Other mental & substance use disorders |
Other mental & substance use disorders |
83 |
|
(a) See ABDS 2018 health states.
(b) Part of the intellectual disability envelope.
Prevalence estimation
Data sources
Key data sources to estimate mental and substance use disorder prevalence are shown below.
Table 4.26: Key data sources for mental and substance use disorder morbidity estimates
|
Data source |
Related diseases |
|---|---|
|
2007 National Survey of Mental Health and Wellbeing |
Depressive disorders, anxiety disorders, alcohol use disorders, and bipolar disorder |
|
2013–14 Child and Adolescent Survey of Mental Health and Wellbeing (Young Minds Matter survey) |
Depressive disorders, anxiety disorders, attention deficit hyperactivity disorder, conduct disorder |
|
National Psychosis Survey (Survey of High Impact Psychosis) 2010 |
Schizophrenia |
|
Intellectual Disability Exploring Answers (IDEA) database |
Idiopathic intellectual disability and autism |
|
National Drug and Alcohol Research Centre analyses |
Opioid use disorders and amphetamine use disorders |
|
Alcohol and other drug treatment services national minimum data set (AODTS-NMDS) (supplemented with article by McKetin et al. 2017) |
Amphetamine use disorders (for reference year 2015 and 2018) |
|
GBD 2017 |
Anorexia nervosa, bulimia nervosa, cannabis use disorders |
|
GBD 2019 |
Cocaine use disorders |
Estimating point prevalence
Adult estimates obtained from the 2007 National Survey of Mental Health and Wellbeing are for 12-month prevalence. To estimate point prevalence, it was assumed that 30-day prevalence would approximate point prevalence, given the long-term nature of the disorders reflected in diagnostic criteria.
As the 30-day prevalence in this survey did not reflect diagnostic criteria as closely, a 30‑day‑to‑12-month prevalence adjustment factor applied to the 12-month estimates was derived from the 1997 National Survey of Mental Health and Wellbeing, based on expert advice.
For major depressive disorder, this ratio was 0.51, and for anxiety disorders it was 0.67. Experts advised that 12-month prevalence would be similar to 30-day prevalence for drug use disorders and dysthymia, so no ratio was applied. These ratios were also applied to estimates for children obtained from the 2013–14 Child and Adolescent Survey of Mental Health and Wellbeing (Young Minds Matter survey).
Idiopathic intellectual disability and autism were considered chronic conditions, so point prevalence was assumed to be the same as period prevalence. Similarly, eating disorders were estimated to result in health loss, on average, for more than 12 months.
Severity distributions and other health states
Severity distributions for depressive disorders, anxiety disorders and drug use disorders (excluding alcohol) were based on the GBD 2013 distributions published by Burstein and others (2015). Severity for alcohol use disorders was based on the (self-reported) extent that alcohol use interfered across various aspects of life in the 2007 National Survey of Mental Health and Wellbeing.
For bipolar disorder, the health states included mania, depression and residual states. For schizophrenia, these were acute (psychotic) and residual states. The distributions of these health states were based on meta-analyses undertaken for GBD 2010 (Ferrari et al. 2012).
No asymptomatic health state was attributed to eating disorders as the health states themselves reflected the intermittent and ongoing nature of these conditions.
The distribution of symptomatic and asymptomatic health states for attention deficit hyperactivity disorder and conduct disorder were based on findings from the Great Smoky Mountain study (Erskine et al. 2014).
Intellectual disability
As an envelope in the ABDS 2018, the overall prevalence of intellectual disability was calculated to ensure the sum of estimates for sequelae did not exceed the total. To avoid double-counting, and adhere to mutually exclusivity for each disease, the proportion of intellectual disability due to each disease was estimated.
Prevalence and severity distribution of the intellectual disability envelope
The total prevalence rate for intellectual disability due to any cause was based on analysis of the IDEA database. IDEA is a Western Australian database of people with intellectual disability who receive: services from the Disability Services Commission; education support from the state’s Department of Education; or, if they were born between 1983 and 1999, support through the Catholic or independent school systems. The database is also linked to registries of births and deaths. In this database, intellectual disability is defined as an intelligence quotient of less than 70, and an indication of developmental delay before the age of 18. Mild, moderate, and severe intellectual disability are defined as an intelligent quotient of 55–69, 40–54 and less than 40, respectively. Estimates were based on births between 1983 and 2013 and followed through to 2018. IDEA data were available for people up to the age of 35.
The overall severity distribution of intellectual disability was based on an international meta‑analysis (King et al. 2009, as cited by Maulik et al. 2011). Borderline intellectual functioning in children aged 0–14 was based on the borderline intellectual functioning‑to‑intellectual disability ratio (using cognitive scores) observed in the Longitudinal Study of Australian Children (Emerson et al. 2010).
Prevalence of intellectual disability by sequelae
The intellectual disability envelope is made up of several infant & congenital conditions, with the remaining intellectual disability falling under idiopathic/other intellectual disability in the mental and substance use disorders disease group (see table below). Cases of comorbid intellectual disability and autism were not attributed an intellectual disability health state, as it was assumed that the burden of these conditions would be captured under the autism health states.
Table 4.27: Diseases within the intellectual disability envelope, and data source(s) for severity
|
Disease |
Source of severity distribution |
|---|---|
|
Pre-term birth & low birthweight complications |
Mild prevalence was based on the proportion reported in the WA IDEA database. The relationship between mild, moderate and severe was based on the National Perinatal Data Collection. |
|
Birth trauma & asphyxia |
Mild prevalence was based on the proportion reported in the WA IDEA database. Moderate and severe were based on severity distributions shown in NHMD analysis. |
|
Neural tube defects |
Based on severity distribution reported by Hunt & Oakeshott (2003), and modelled in DisMod II. |
|
Brain malformations |
The severity distribution for birth trauma & asphyxia was used for brain malformations. This decision was informed by data from the WA IDEA database, which showed that the severity distribution for brain malformations and brain trauma & asphyxia were similar. |
|
Down syndrome |
All prevalence was based on the proportion reported in the WA IDEA database, adjusted for deaths. |
|
Other chromosomal abnormalities |
All prevalence was based on the proportion reported in the WA IDEA database. |
The proportions of total intellectual disability that could be attributed to diseases specified in the ABDS 2018 were mostly derived from the IDEA database. This was available separately for mild/moderate and severe/profound severity categories. For Down syndrome and other chromosomal abnormalities, prevalence was estimated directly by applying these proportions to the total.
In some cases, the severity distribution was obtained from another source (see table above). For those conditions, IDEA was used to estimate the number of mild cases, and the remaining severity estimates were calculated relative to the mild estimate.
Motor/cognitive impairment due to neural tube defects was modelled in DisMod II.
Idiopathic intellectual disability
Intellectual disability sequelae from other diseases (including motor-cognitive sequelae) were subtracted from the intellectual disability envelope. The remaining estimates were the prevalence of idiopathic intellectual disability (which also includes other underlying conditions resulting in intellectual disability not captured elsewhere). All borderline intellectual disability was attributed to the idiopathic/other category.
Other mental and substance use disorders
This residual group includes delirium, personality disorders, and any remaining child disorders such as specific learning disorders, developmental disorders and sleep disorders.
The prevalence of other mental and substance use disorders was estimated by analysing hospitalisations for the corresponding ICD-10-AM codes (F04–09, F17, F38, F44–49, F51–69, F80–83, F85–89, F93–99).These separations were then compared with those for depression, anxiety, bipolar, schizophrenia, conduct disorder, and attention deficit hyperactivity disorder (that is, conditions with some similar aspects and conceivably similar rates of hospitalisation).
Rate ratios were specific to the reference year (2003, 2011, 2015 or 2018) and age group, but were not created separately for sub-national estimates. Separation rate ratios were then applied to the combined point prevalence estimates, by age and sex (excluding asymptomatic estimates) of the compared conditions to calculate the prevalence of other mental and substance use disorders. This assumes a similar hospitalisation rate for other mental and substance use disorders and the identified conditions.
Sub-national estimates
The 2007 National Survey of Mental Health and Wellbeing was analysed to calculate total prevalence rate ratios for each socioeconomic group, remoteness area (Very remote areas were not sampled), and state/territory. These were then applied to the national prevalence rates for depressive disorders, anxiety disorders, bipolar disorder, alcohol use disorders and drug use disorders. Where these rate ratios were unreliable due to small sample sizes, a proxy rate ratio was used, usually from a nearby state/territory (the rate ratio for Victoria was used for Tasmania, the rate ratio for New South Wales for the Australian Capital Territory, and the rate ratio for South Australia for the Northern Territory).
State and territory rate ratios for opioid use disorders were based on the analysis by Degenhardt and others (2004). The relative rate of hospitalisations for these disorders in Outer regional, Remote and Very remote areas was applied to provide rate ratios for Very remote areas, which was not sampled in the 2007 National Survey of Mental Health and Wellbeing.
The socioeconomic group rate ratios calculated for bipolar disorder were also applied to schizophrenia, due to lack of specific schizophrenia data. Schizophrenia prevalence rates were modelled as consistent across remoteness areas and state/territory.
For attention deficit hyperactivity disorder and conduct disorder, rate ratios were available by remoteness area and socioeconomic group, but not state/territory from the 2013–14 Child and Adolescent Survey of Mental Health and Wellbeing (Young Minds Matter survey). Consistent prevalence rates were assumed across states and territories for these 2 conditions.
For eating disorders, autism and intellectual disability, the same prevalence rates were assumed to be consistent across socioeconomic groups, remoteness areas and states/territories due to lack of data.
2015, 2011 and 2003 estimates
With a few exceptions, all prevalence rates were considered stable between 2003, 2011 and 2015, based on expert advice or lack of available evidence to suggest a significant change. The 2003 opioid prevalence estimates were based on estimates of prevalence in 2002, as reported by Degenhardt et al. (2004). These estimates were then adjusted for change over time, based on data from the National Opioid Pharmacotherapy Statistical Annual Data collection.
The data source for amphetamine disorders (Degenhardt et al. 2016) included estimates for 2003–04 and 2011–12, so each of these was used for the corresponding reference year. The data source for 2015 estimates was the same as the 2018 estimates but for the corresponding reference year.
Prevalence estimates for other drug use disorders and other mental and substance use disorders were based on hospitalisation ratios, so for 2003, 2011 and 2015 these were based on hospitalisations during the 2003, 2011 and 2015 calendar year, respectively.
Some of the specific causes of intellectual disability that contributed to the intellectual disability envelope were adjusted for differences in rates reported by WARDA for 2003, 2011 and 2015.
Indigenous specific estimates
All Indigenous estimates were calculated using indirect methods which involved applying rate ratios from secondary data sources to national prevalence rates. This method was used as no Indigenous-specific data sources were identified that provided adequate information on the prevalence of mental and substance use disorders in the Aboriginal and Torres Strait Islander population.
For depressive disorders, anxiety disorders, bipolar disorder and schizophrenia, Indigenous prevalence estimates were calculated using Indigenous: total population rate ratios from data provided by Queensland Health from their Consumer Integrated Mental Health Application (CIMHA). This is ICD-10-AM coded linked inpatient separation and community mental health services data which provides a measure of the number of persons accessing Queensland public mental health services.
For alcohol use disorders, for which prevalence estimates are required by level of severity, hospitalisation rate ratios were used to derive Indigenous prevalence estimates for asymptomatic/very mild/mild cases of alcohol dependence; and rate ratios from Queensland’s CIMHA data were applied to derive Indigenous prevalence estimates for moderate and severe cases of alcohol dependence.
For drug use disorders, CIMHA modelling rate ratios were used to derive Indigenous prevalence for opioid, cannabis and amphetamine dependence (for all levels of severity). For cocaine dependence, rate ratios from self-reported survey data (AIHW 2019) were used to derive Indigenous prevalence (for all levels of severity).
For attention-deficit/hyperactivity disorder and conduct disorder, Indigenous prevalence estimates were based on the rate ratios from the Longitudinal Survey of Australian Children and CIMHA. An average of these rate ratios was applied to national prevalence estimates.
For eating disorders and autism spectrum disorders total population prevalence rates were applied to the Indigenous population.
For intellectual disability, Indigenous prevalence estimates were calculated using rate ratios derived from the original 2011 ABDS Indigenous estimates and population. The rate ratios were applied to the 2018 ABDS national rate, which was then applied to the 2018 Indigenous population.
Other drug use disorders and other mental and substance use disorders were all based on hospitalisation rate ratios specific to 2018.
References
AIHW (Australian Institute of Health and Welfare) 2019. Data tables: National Drug Strategy Household Survey 2019 – 8 Priority population groups supplementary tables. Accessed 28 April 2021.
Burstein R, Fleming T, Haagsma J, Salomon JA, Vos T & Murray CJL 2015. Estimating distributions of health state severity for the global burden of disease study. Population Health Metrics 13:31.
Degenhardt L, Larney S, Chan G, Dobbins T, Weier M, Roxburgh A et al. 2016. Estimating the number of regular and dependent methamphetamine users in Australia, 2002–2014. Medical Journal of Australia 204(4):1.e2–6.
Degenhardt L, Rendle V, Hall W, Gilmour S & Law M 2004. Estimating the number of current regular heroin users in NSW and Australia 1997–2002. Sydney: National Drug and Alcohol Research Centre.
Emerson E, Einfeld S & Stancliffe RJ 2010. The mental health of young children with intellectual disabilities or borderline intellectual functioning. Social Psychiatry and Psychiatric Epidemiology 45:579.
Erskine HE, Ferrari AJ, Polanczyk GV, Moffitt TE, Murray CJ, Vos T et al. 2014. The global burden of conduct disorder and attention‐deficit/hyperactivity disorder in 2010. Journal of Child Psychology and Psychiatry 55(4):328–36.
Ferrari AJ, Saha S, McGrath JJ, Norman R, Baxter AJ, Vos T et al. 2012. Health states for schizophrenia and bipolar disorder within the Global Burden of Disease 2010 Study. Population Health Metrics 10(1):16.
Global Burden of Disease Collaborative Network 2018. Global Burden of Disease Study 2017 (GBD 2017) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME).
Global Burden of Disease Collaborative Network 2020. Global Burden of Disease Study 2019 (GBD 2019) Results. Seattle: Institute for Health Metrics and Evaluation (IHME).
Hunt GM & Oakeshott P 2003. Outcome in people with spina bifida at age 35: prospective community based cohort study. BMJ 326:1365–6.
Maulik PK, Mascarenhas MN, Mathers CD, Dua T & Saxena S 2011. Prevalence of intellectual disability: a meta-analysis of population-based studies. Research in Developmental Disabilities 32(2):419–36.
McKetin R, Voce A and Burns R (2017). Research into methamphetamine use in the Australian Capital Territory. Perth: National Drug Research Institute, Curtin University.
Sequelae and health states
Sequelae and health states assigned to musculoskeletal conditions are shown in the table below. Durations and assumptions are outlined in subsections for individual diseases.
Table 4.28: Sequelae and health states for musculoskeletal conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Osteoarthritis |
Osteoarthritis of the knee |
262, 126, 127, 128 |
|
|
Osteoarthritis of the hip |
262, 126, 127, 128 |
|
Gout |
Musculoskeletal problems caused by gout |
132, 133 |
|
Rheumatoid arthritis |
Musculoskeletal problems caused by rheumatoid arthritis |
262, 130, 131, 132 |
|
Back pain & problems |
Back pain & problems |
262, 234, 254, 233, 255, 241, 242, 239, 240 |
|
Other musculoskeletal conditions(b) |
Other musculoskeletal problems |
262, 126, 127, 128, 130, 131, 132 |
(a) See ABDS 2018 health states.
(b) Other musculoskeletal conditions excludes symptoms and signs involving musculoskeletal conditions and osteoporosis.
Prevalence estimation
Prevalence estimates for musculoskeletal conditions were derived from self-reported data in the NHS 2017–18, as it covered all the musculoskeletal conditions of interest.
Though self-reported data is generally not considered as good as clinical data, Peeters and others (2015) found that self-reported data is acceptable for osteoarthritis and rheumatoid arthritis. Data derived from the survey was available for 5-year age groups (0–85 and over). For individual diseases and sub-national estimates, these 5-year age groups were combined to deal with sample size issues from the survey. Modelling was required to redistribute the data into 5-year age groups for analysis. As well, the NHS 2017–18 did not report on Very remote areas, so prevalence estimates were adjusted to account for Very remote areas.
The severity distribution for each of the musculoskeletal conditions, except for gout, is based on the distribution across the 6 pain categories (none, very mild, mild, moderate, severe, or very severe) in the preceding 4 weeks, as used in the NHS 2017–18. The pain categories were mapped to the relevant health states, as described in the following individual sections. For each condition, the severity distribution analysis was limited to those who only reported experiencing the condition of interest (that is, not multiple conditions) to ensure that the severity distribution was specific for each condition. This distribution was then applied to all cases of the condition. A key assumption from this method was that the proportion of people who report no pain in the preceding 4 weeks was equivalent to the proportion of people with the condition who are asymptomatic at any point in time.
The GBD study used a method to avoid double counting of disease associated with post‑traumatic effects of injury that lead to long-term musculoskeletal conditions. This method was not implemented in the ABDS 2018, and as a result, there is potential overlap between other musculoskeletal conditions and osteoarthritis with selected injuries such as fractures and dislocations (see ABDS diseases associated with previous injury).
Osteoarthritis
The NHS 2017–18 data for osteoarthritis cannot be broken down into the sequelae osteoarthritis of the hip and osteoarthritis of the knee; this was split (for risk factor analysis) using proportions from the GBD 2017—85% to knee and 15% to hip.
Severity is based on the distribution of the pain experienced in the previous 4 weeks by people reporting osteoarthritis only. Health loss is assumed to last for the entire year.
Table 4.29: ABDS severity distributions (%) for osteoarthritis
|
Reference year (Data source) |
Asymptomatic |
Mild |
Moderate |
Severe |
|---|---|---|---|---|
|
2003 (2011–12 AHS) |
14.5 |
46.9 |
28.0 |
10.6 |
|
2011 (2011–12 NHS) |
14.5 |
46.9 |
28.0 |
10.6 |
|
2015 (2014–15 NHS) |
10.8 |
42.7 |
32.7 |
13.8 |
|
2018 (2017–18 NHS) |
13.6 |
41.9 |
30.9 |
13.5 |
Gout
As a breakdown of chronic or acute gout was not available in the NHS 2017–18 data, the distribution of severity and the average number and duration of gout episodes was based on the GBD 2010 pain method (Hoy et al. 2014). This method assigned 1.4% of cases as chronic (with 12 months duration) and the remaining 98.6% of cases as acute, with an average 3.9 episodes of 6.8 days duration per year.
Note that the AIHW has changed how they report gout prevalence using the 2017–18 NHS data and now counts any person who reported ever having gout (AIHW 2020).
Rheumatoid arthritis
The NHS 2017–18 does not collect information on the affected joints or the severity of rheumatoid arthritis. The distribution of severity for rheumatoid arthritis is based on the distribution of pain reported by people reporting rheumatoid arthritis only in the NHS 2017–18. Health loss is assumed to last for the entire year.
Table 4.30: ABDS severity distributions (%) for rheumatoid arthritis
|
Reference year (Data source) |
Asymptomatic |
Mild |
Moderate |
Severe |
|
2003 (2014–15 NHS) |
16.2 |
32.1 |
35.0 |
16.7 |
|
2011 (2014–15 NHS) |
16.2 |
32.1 |
35.0 |
16.7 |
|
2015 (2014–15 NHS) |
16.2 |
32.1 |
35.0 |
16.7 |
|
2018 (2017–18 NHS) |
13.6 |
38.1 |
30.4 |
18.0 |
Back pain and problems
The NHS 2017–18 data only collected information on back pain as a long-term (chronic) condition. Health loss is assumed to last for the entire year. No estimates are provided for short-term back pain & problems. The distribution of severity for back pain and problems is based on an associated pain data distribution (back pain & problems only) from the NHS 2017–18. Because this variable did not distinguish between those with or without leg pain, the proportion of people experiencing pain at each severity level was divided into with and without leg pain according to proportions from the GBD 2015. The resulting severity distributions are provided below.
Table 4.31: ABDS severity distributions (%) for back pain and problems
| Reference year (Data source) | Asymptomatic | Mild | Moderate | Severe | Very severe |
|---|---|---|---|---|---|
| 2003 and 2011 (2014–15 NHS) | |||||
| Without leg pain (%) | 14.1 | 43.2 | 19.6 | 6.2 | 1.4 |
| With leg pain (%) | . . | 7.6 | 5.2 | 2.1 | 0.5 |
|
Total |
14.1 | 50.8 | 24.8 | 8.3 | 1.9 |
| 2015 (2014–15 NHS) | |||||
| Without leg pain (%) | 14.1 | 43.2 | 19.6 | 6.2 | 1.4 |
| With leg pain (%) | . . | 7.6 | 5.2 | 2.1 | 0.5 |
| Total | 14.1 | 50.8 | 24.8 | 8.3 | 1.9 |
| 2018 (2017–18 NHS) | |||||
| Without leg pain (%) | 13.5 | 39.4 | 23.1 | 6.5 | 1.6 |
| With leg pain (%) | . . | 7.0 | 6.1 | 2.2 | 0.6 |
| Total | 13.5 | 46.3 | 29.2 | 8.6 | 2.2 |
Other musculoskeletal conditions
The prevalence of other musculoskeletal conditions was also derived from the NHS 2017–18. It was estimated by combining the prevalence of specific musculoskeletal conditions (excluding osteoarthritis, rheumatoid arthritis, gout, and back pain/problems) including the following: other arthropathies, other soft tissue disorders, other diseases of the musculoskeletal system and connective tissue, rheumatism and arthritis—other and type unknown.
The distribution of severity for other musculoskeletal conditions is based on associated pain data distribution (other musculoskeletal conditions only) from the NHS 2017–18
Table 4.32: ABDS severity distributions (%) for other musculoskeletal conditions
|
Reference year (Data source) |
Asymptomatic |
Level 1 |
Level 2 |
Level 3 |
Level 4 |
Level 5 |
Level 6 |
|---|---|---|---|---|---|---|---|
|
2003 (2014–15 NHS) |
17.8 |
23.3 |
21.8 |
13.1 |
13.1 |
9.0 |
2.0 |
|
2011 (2014–15 NHS) |
17.8 |
23.3 |
21.8 |
13.1 |
13.1 |
9.0 |
2.0 |
|
2015 (2014–15 NHS) |
17.8 |
23.3 |
21.8 |
13.1 |
13.1 |
9.0 |
2.0 |
|
2018 (2017–18 NHS) |
14.5 |
24.2 |
21.3 |
14.6 |
14.6 |
9.5 |
1.4 |
It is important to note that the NHS 2017–18 does not distinguish cases of other musculoskeletal conditions or osteoarthritis that were due to injuries; therefore, there may be double counting of prevalence in the musculoskeletal and injuries disease groups (see ABDS diseases associated with previous injury).
Sub-national estimates
National prevalence estimates were apportioned based on sex and combined age-specific estimates from the NHS 2017–18 to derive sub-national estimates. Sex and 5-year age‑specific proportions were not used due to a high degree of uncertainty in some 5-year age groups, with RSEs of more than 50% for these estimates. Given that the NHS did not include people living in Very remote areas an adjustment based on population size was performed to inflate prevalence estimates to account for these people.
2015, 2011 and 2003 estimates
Due to some data issues with the coding of musculoskeletal conditions in the 2011–12 NHS (ABS 2015) the 2011–12 survey data for back pain & problems, rheumatoid arthritis, gout and other musculoskeletal conditions were not used. Instead, the prevalence for 2011 for these diseases was estimated using linear spline interpolation using the age/sex prevalence data for the other reference years. For other musculoskeletal conditions, estimates for 2003 and 2011 prevalence rates from 2015 were applied to the 2011 and 2003 populations. The severity distribution from the 2014–15 NHS was used for both 2003 and 2011 estimates for other musculoskeletal conditions, rheumatoid arthritis and back pain & problems.
The same methods used for the 2018, 2015 and 2011 estimates were used for 2003 non-fatal burden musculoskeletal conditions estimates. The primary data source was the NHS 2004–05. Since the data were not specific to 2003, a survey prevalence rate (that is, rates generated from the survey population) was applied to the 2003 Estimated Resident Population to estimate the 2003 population prevalence of each disease. As no equivalent pain variable was available for the NHS 2004–05, the same severity distributions used for 2011 were assumed for each disease.
It is important to note that some of the differences between the reference years will be due to differences in the severity distributions
Indigenous specific estimates
The methods used for estimating non-fatal musculoskeletal conditions burden for the Indigenous population was similar to the method used for national estimates.
The AATSIHS 2012–13 was the primary data source for 2011 estimates. After consultation with ABS regarding a specific data quality issue with published musculoskeletal data from the survey, the ABS provided the AIHW with revised data for back pain and problems and other musculoskeletal conditions for our analysis. The revised data are currently unpublished by the ABS, but available on request. Where the RSE was high for certain 5-year age groups, the national 5-year age distribution was applied to the Indigenous prevalence estimate specific for those age groups.
As the musculoskeletal data items from previous ABS Indigenous health surveys were not comparable to those from the AATSIHS 2012–13, and there was little evidence to suggest a recent change in prevalence of musculoskeletal conditions in the Indigenous population, Indigenous estimates for 2003 were derived from rates from the AATSIHS 2012–13 applied to the 2003 Indigenous population.
The severity distribution for each condition was assumed to be the same as for the national estimates for both 2011 and 2003.
References
ABS 2015. National Health Survey: First Results, 2014–15 Explanatory Notes. 4364.0.55.001. Viewed 3 May 2021.
AIHW 2020. Gout. Cat. no. PHE 259. Canberra: AIHW. Viewed 3 May 2021.
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators 2016. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study. Supplementary appendix. The Lancet 388: 1545–602.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 2018. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Supplementary appendix. The Lancet 392: 1789–858.
Hoy DG, Smith E, Cross M, Sanchez-Riera L, Buchbinder R, Blyth FM et al. 2014. The global burden of musculoskeletal conditions for 2010: an overview of methods. Annals of the Rheumatic Diseases 73(6):982–9.
Peeters GMEE, Alshurafa M, Schaap L, de Vet HCW 2015. Diagnostic accuracy of self-reported arthritis in the general adult population is acceptable. Journal of Clinical Epidemiology 68:452–59.
Sequelae and health states
Sequelae and health states assigned to the neurological conditions are shown below. Durations and assumptions are outlined in subsections for individual diseases.
Table 4.33: Sequelae and health states for neurological conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Epilepsy |
Epilepsy |
207, 248, 249 |
|
Dementia |
Dementia |
58, 59, 60 |
|
Parkinson disease |
Parkinson disease |
70, 71, 72 |
|
Multiple sclerosis |
Multiple sclerosis |
63, 64, 65 |
|
Motor neurone disease |
Motor neurone disease |
65 |
|
Migraine |
Migraine |
61 |
|
Guillain-Barré syndrome |
Guillain-Barré syndrome |
188 |
(a) See ABDS 2018 health states.
Prevalence estimation
Epilepsy
For the ABDS 2018, epilepsy is defined as a chronic disorder of the brain characterised by recurrent seizures, as consistent with the GBD 2017. National sex-specific prevalence estimates of self-reported epilepsy were obtained from the NHS 2017–18. The NHS 2017–18 did not report on Very remote areas, so prevalence estimates were adjusted to account for Very remote areas. Age–sex specific distributions couldn’t be obtained from the NHS 2017–18 as the RSEs for the epilepsy counts in many age groups were too high. Instead, an age distribution by state and sex was calculated using hospitalisation data from the NHMD. Counts of hospital separations from the NHMD were adjusted to account for readmissions using linked hospitalisation and deaths data from the NIHSI AA v0.5. Admitted hospitalisations data were available from the NIHSI AA v0.5 for New South Wales, Victoria, South Australia and Tasmania. Where numbers allowed, that is, the numbers were not low enough to cause volatility in estimates, state-specific ratios were calculated. Otherwise, data from all 4 jurisdictions were used for the ratios. For states and territories that did not have hospitals data in the NIHSI AA v0.5, ratios using all 4 jurisdictions combined were used. This assumes that persons-to-separations ratios were similar across all jurisdictions. The age and state/territory distributions for each sex were then applied to the NHS 2017–18 national sex-specific prevalence estimates to obtain the estimates by age, sex and state/territory. State and territory estimates were summed to obtain final national prevalence estimates. There was no direct Australian data source to estimate the severity of epilepsy as defined in the ABDS 2018, therefore the severity distribution of epilepsy was based on a study conducted in the United Kingdom by Moran et al. (2004).
Dementia
Dementia includes Alzheimer’s disease (the most common form), vascular dementia, dementia with Lewy bodies and frontotemporal dementia (ICD-10-AM: F00–F03, G30–G31). Prevalence estimates for dementia were calculated by applying the prevalence rates used in the Dementia in Australia report (AIHW 2021) to the Australian estimated resident population. The Dementia in Australia report uses rates reported by the 2015 World Alzheimer Report for adults aged 60 and older. For adults under 60 years, the report uses rates published in a community-based study conducted in Sydney, Australia in 2008 (Withall et al. 2014), with sex ratios from an international epidemiological study applied (Harvey et al., 2003). The severity distribution of dementia was estimated using 2 European studies (Barendregt & Bonneux 1998; Lucca et al. 2015), for those aged under 80 and aged over 80 separately.
For more information on the methods used to derive dementia prevalence estimates, see the methods of estimating the number of Australians living with dementia in the AIHW Dementia in Australia report (AIHW 2021).
Parkinson disease
There was a lack of recently published, high quality, population-based Australian studies on Parkinson disease at the time of analysis. Thus, prevalence was estimated using rates from a number of international studies (de Rijk et al. 1995; de Rijk et al. 2000; Willis et al. 2013). Prevalence rates from the de Rijk studies were applied to the Australian estimated resident population for people aged 55 and over. Prevalence rates of Parkinson disease in Australians aged 30–55 were modelled based on findings from the Willis study, assuming there is an increasing linear trend in the rates of Parkinson disease in these age groups. For Australians aged under 30, the prevalence of Parkinson disease was assumed to be zero.
A severity distribution by broad age groups was derived from unpublished data from the Queensland Parkinson Project.
Multiple sclerosis
Prevalence of multiple sclerosis was estimated using prevalence rates from an Australian report prepared by the Menzies Health Economic Research Group, Associate Professor Ingrid van der Mei and Professor Bruce Taylor (Menzies Health Research Group, van der Mei & Taylor 2018). A sex ratio of 3:1 (female: male) was applied to the national prevalence based on data from the Multiple Sclerosis Australia database (Covance Pty Ltd & Palmer 2011). The age distribution of multiple sclerosis was modelled based on the 2018 Survey of Disability, Ageing and Carers (SDAC). The 2018 SDAC is a national survey that collects information on people with disabilities, people aged 65 and over and carers of people with disability, long-term health conditions or older people. When finer age distributions were required, 2018 NHMD separations were used.
The severity distribution was obtained from the joint report by Covance Pty Ltd and Professor Andrew Palmer (Covance Pty Ltd & Palmer 2011).
Motor neurone disease
Motor neurone diseases (MND) are a group of progressive neurological disorders (including amyotrophic lateral sclerosis) that destroy motor neurones. National prevalence of MND was estimated by applying person-to-separation ratios calculated using linked hospitalisations and deaths data from the NIHSI AA v0.5 to hospital separation counts from the NHMD. Admitted hospitalisation data were available from the NIHSI AA v0.5 for New South Wales, Victoria, South Australia and Tasmania, however the numbers were low enough to cause volatility in estimates and therefore the data from all 4 jurisdictions were combined. These combined ratios were applied to all states and territories, assuming that persons-to-separations ratios were similar across all jurisdictions.
Since the GBD 2017 did not have a disability weight specific to motor neurone disease, the disability weight for severe multiple sclerosis was applied.
Migraine
According to Headache Australia, migraine is an episodic condition characterised by quiescent and relapse phases, known as headaches that typically last 4–72 hours. Age-and-sex specific prevalence estimates for migraine were based on the NHS 2017–18 self-reported data. As data was not available from the NHS at the required age group disaggregation, some modelling was undertaken to obtain estimates for the older age groups. The NHS 2017–18 did not report on Very remote areas, so prevalence estimates were adjusted to account for Very remote areas. A duration of 27 days per year was applied to the national estimates to obtain point prevalence. This is the duration used in GBD 2017 which was based on two meta-analyses which reported an average frequency of 43.8 episodes per year and an average duration per episode of 14.87 hours (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 2018).
Guillain-Barré syndrome
Guillain-Barré syndrome (GBS) is a disease of the peripheral nervous system that might develop spontaneously or after a systemic infection or other stress. National age- and sex-specific prevalence of GBS were estimated by applying person-to-separation ratios calculated using linked hospitalisations and deaths data from the NIHSI AA v0.5 to hospital separation counts from the NHMD. Admitted hospitalisation data were available from the NIHSI AA v0.5 for New South Wales, Victoria, South Australia and Tasmania, however the numbers for Tasmania were low enough to cause volatility in estimates and were therefore not used in isolation. For Tasmania, Western Australia, the Australian Capital Territory and the Northern Territory, the data from New South Wales, Victoria, South Australia and Tasmania were combined and these ratios applied, assuming that persons-to-separations ratios were similar across the jurisdictions. Additionally, ratios were only available by sex, therefore the same ratio was applied to each age group within each sex. The person counts were then summed to obtain national estimates. A duration of 6.7 months was based on the GBD 2013 (GBD 2013 Collaborators 2015) and was applied to the national prevalence estimates to obtain national point prevalence estimates.
Other neurological conditions
The prevalence of other neurological conditions is the prevalence of the remaining neurological conditions that are not listed above. The prevalence for other neurological conditions was estimated by applying a YLD:YLL ratio for Parkinson disease, multiple sclerosis and motor neurone disease combined to the YLL for other neurological conditions.
Sub-national estimates
For migraine, sex-specific proportions of people who self-reported this condition were obtained at all the sub-national levels (state and territory, remoteness and socioeconomic group) from the NHS 2017–18. These proportions were applied to the national prevalence estimates to obtain the sub-national estimates.
For epilepsy, the proportions of people who self-reported this condition were obtained from the NHS 2017–18 by socioeconomic group, and by sex and remoteness area. These proportions were applied to the national prevalence estimates to obtain the sub-national estimates. State and territory prevalence estimates were generated during the process of obtaining national estimates, therefore see methods for national epilepsy estimates.
For motor neurone disease (MND) and Guillain-Barré syndrome (GBS), the number of separations at the state and territory level were derived from the NHMD directly and person-to-separation ratios obtained from the NIHSI AA v0.5 were applied to these separation counts, as consistent with the national estimates. For MND, state and territory-specific ratios were not available, therefore ratios calculated using data from the 4 jurisdictions for which hospitalisations data was available in the NIHSI AA v0.5 were applied. For GBS state and territory-specific ratios were available for South Australia, Victoria and New South Wales and for all other jurisdictions combined state and territory ratios were used. For both MND and GBS, remoteness and socioeconomic group estimates were calculated by applying proportions of NHMD separations by age, sex and remoteness/socioeconomic group to the national estimates.
For multiple sclerosis, prevalence rates by state and territory and proportions by remoteness area were available from the 2018 Menzies Health Economic Research Group report (Menzies Health Research Group, van der Mei & Taylor 2018). Prevalence estimates by socioeconomic group were calculated by applying proportions of multiple sclerosis deaths derived from the NMD to the national estimates.
For dementia and Parkinson disease, estimates by state and territory, remoteness area and socioeconomic group were derived by applying proportions of deaths due to the condition from the NMD to the national estimates.
2015, 2011 and 2003 estimates
Where available, the methods and data sources used to estimate prevalence in 2003, 2011 and 2015 were largely similar to those for 2018, however different years of data were used. For motor neurone disease and Guillain-Barré syndrome, prevalence estimates for 2015, 2011 and 2003 were also largely derived from the NHMD using data relevant to each reference year. However, since the NIHSI AA v0.5 only contains hospitalisations data from 2010–17, persons-to-separations ratios calculated for 2011 were also used for estimating prevalence in 2003.
For epilepsy, data were available from the NHS 2004–05, AHS 2011–12 and the NHS 2014–2015 and used for the 2003, 2011 and 2015 estimates respectively. Age, sex and state/territory distributions were calculated using NHMD separations data relevant to each reference year. The same person-to-separation ratios were applied to the count of hospital separations for each reference year.
For migraine, data was available from the NHS 2004–05, AHS 2011–12 and the NHS 2014–2015 and used for the 2003, 2011 and 2015 estimates respectively.
For multiple sclerosis, the same prevalence rates that were used for the 2018 estimates were also used for the 2015 estimates. The 2003 and 2011 estimates were based on the prevalence rates from an earlier study by Andrew Palmer (Palmer et al. 2013). The age distribution for the 2015 estimates were modelled based on 2015 NHMD and SDAC data, whereas the 2011 and 2003 estimates were modelled based on 2009 NHMD and SDAC data. The same sex ratio that was applied to the 2018 estimates was also applied to the 2015, 2011 and 2003 estimates.
For dementia and Parkinson disease the same prevalence rates which were used for the 2018 estimates were also used for the 2003, 2011 and 2015 estimates.
Indigenous specific estimates
Indigenous estimates based on hospital separations data (epilepsy and Guillain-Barré syndrome) were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
Indigenous estimates for motor neurone disease were based on mortality data and were adjusted for under-identification using standard adjustment factors (see Years of life lost (YLL)).
Indigenous prevalence for epilepsy and migraine were derived from the AATSIHS 2012–13 for 2011 estimates and the NATSIHS 2004–05 for 2003 estimates using a similar method as national estimates.
Indigenous dementia prevalence was obtained using three Australian studies (Li et al 2014, Radford et al. 2015, Smith et al. 2008). Severity distribution was obtained from the Koori Growing Old Well Study and the Barendregt & Bonneux (1998) studies. The same prevalence rates and severity distributions were applied for 2003 Indigenous estimates.
Due to the lack of Indigenous-specific data on Parkinson disease and multiple sclerosis, national prevalence rates were applied to the Indigenous population to derive Indigenous prevalence for both 2011 and 2003 estimates. For multiple sclerosis, prevalence rates were also adjusted to reflect the lower rates in Indigenous populations (compared to National populations) as found in a NZ study 2014 (Pearson JF et al 2014) and found in comparisons of Australian hospitalisation and mortality data.
References
AIHW 2021. Dementia in Australia. Cat. no. DEM 2. Canberra: AIHW.
Barendregt JJM & Bonneux LGA 1998. Degenerative disease in an aging population models and conjectures. Rotterdam: Erasmus University.
Covance Pty Ltd & Palmer A 2011. Economic impact of multiple sclerosis in 2010: Australian Multiple Sclerosis Longitudinal Study. North Ryde: Covance Pty Ltd. Viewed 16 July 2014.
De Rijk MC, Breteler MMB, Graveland GA, Ott A, Grobbee DE, van der Meché FGA et al. 1995. Prevalence of Parkinson’s disease in the elderly: The Rotterdam Study. Neurology 45: 2413–6.
de Rijk MC, Launer LJ, Berger K, Breteler MMB, Fartigues JF, Baldereschi M et al. 2000. Prevalence of Parkinson disease in Europe: a collaborative study of population-based cohorts. Neurology 54(Suppl 5):S21–3.
GBD (Global Burden of Disease Study) 2013 Collaborators 2015. Supplement to: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 386(10010): S1–1868.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 2018. Supplementary appendix 1 to: Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392: 1789–858.
Harvey RJ, Skelton-Robinson M & Rossor MN 2003. The prevalence and causes of dementia in people under the age of 65 years. Journal of Neurology, Neurosurgery & Psychiatry 74(9):1206–9.
Li SQ, Guthridge SL, Eswara Aratchige P, Lowe MP, Wang Z, Zhao Y et al. 2014. Dementia prevalence and incidence among the Indigenous and non-Indigenous populations of the Northern Territory. Medical Journal of Australia 200: 465–69
Lucca U, Tettamanti M, Logroscino G, Tiraboschi P, Landi C, Sacco L et al. 2015. Prevalence of dementia in the oldest old: The Monzino 80-plus population based study. Alzheimer’s and Dementia 11:258–70.
Menzies Health Economics Research Group, Ahmad H, Palmer AJ, Campbell JA, van der Mei I & Taylor B 2018. Health economic impact of multiple sclerosis in Australia in 2017: an analysis of MS Research Australia’s platform—the Australian MS Longitudinal Study (AMSLS). North Sydney: Menzies Institute for Medical Research, University of Tasmania. Viewed 23 August 2018.
Moran NF, Poole K, Bell G, Solomon J, Kendall S, McCarthy M et al. 2004. Epilepsy in the United Kingdom: seizure frequency and severity, anti-epileptic drug utilization and impact on life in 1652 people with epilepsy. Seizure 13(6):425–33.
Palmer AJ, Hitchens PL, Simpson Jr. S, O’Leary B, Colman S & Taylor BV 2013. A novel method for calculating prevalence of multiple sclerosis in Australia. Multiple Sclerosis Journal 19(13):1704–11.
Pearson JF, Alla S, Clarke G, Taylor BV, Miller DH, Richardson A et al. 2014. Multiple sclerosis in New Zealand Māori. Multiple Sclerosis Journal 20(14):1892–5.
Radford K, Mack HA, Draper B, Chalkley S, Daylight G, Cumming R et al. 2015. Prevalence of dementia in urban and regional Aboriginal Australians. Alzheimer's & Dementia 11(3):271–9.
Smith K, Flicker L, Lautenschlager NT, Almeida OP, Atkinson D, Dwyer A et al. 2008. High prevalence of dementia and cognitive impairment in Indigenous Australians. Neurology 71(19):1470–3.
Willis AW, Schootman M, Kung N & Racette BA 2013. Epidemiology and neuropsychiatric manifestations of young onset Parkinson disease in the United States. Parkinsonism and Related Disorders 19(2):202–6.
Withall A, Draper B, Seeher K, Brodaty H 2014. The prevalence and causes of younger onset dementia in Eastern Sydney, Australia. International Psychogeriatrics 26(12):1955-65.
Sequelae and health states
Sequelae and health states assigned to oral disorders are shown below. Durations and assumptions are outlined in subsections for individual diseases.
Table 4.34: Sequelae and health states for oral disorders
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Dental caries |
Untreated dental caries (including failed restorations) |
199, 262 |
|
Periodontal disease |
Chronic periodontal disease |
198, 262 |
|
Severe tooth loss |
Severe tooth loss |
200, 262 |
|
Other oral disorders |
Other oral disorders |
200 |
(a) See ABDS 2018 health states.
Prevalence estimation
The prevalence of dental caries, periodontal disease and severe tooth loss in adults was based on analysis of the National Survey of Adult Oral Health 2017–18 (ARCPOH 2019). This survey reported on dental caries apparent during a dental examination, which were measured as part of the DMFT (decayed, missing and filled teeth) index. For this index, DT (decayed teeth) scores indicate the number of dental caries, MT (missing teeth scores): the number of missing teeth, and FT (filled teeth) scores: the number of fillings. The number of adults with complete tooth loss was based on a self-report component of this survey.
Periodontal disease and severe tooth loss was not estimated in children aged under 15 as it is relatively uncommon. Estimates of dental caries in children were modelled with inputs from the National Child Oral Health Study 2012–14 (Do & Spencer 2016), and also past trends from the Child Dental Health Survey 2009 using the DMFT measure (caries in deciduous and adult teeth were both counted)(ARCPOH 2015, Ha et al. 2013).
Dental caries
Prevalence of dental caries was based on the proportion of people with a DT score greater than 1. This was then inflated to account for failed restorations (failed fillings) based on findings reported by Brennan & Spencer (2004).
Periodontal disease
Periodontal disease prevalence was based on cases of moderate–severe periodontal disease according to definitions developed by the Centers for Disease Control and Prevention/American Academy of Periodontology.
No periodontal disease was estimated in children aged under 15, as chronic periodontal disease in children aged under 15 years is relatively rare (Conway et al. 2014), and developmental changes reduce the accuracy of assessment of the disease in children (Jenkins & Papapanou 2001). A review of periodontal disease in children concluded that the prevalence and severity was very low in deciduous teeth (Jenkins & Papapanou 2001). Therefore, the prevalence of chronic periodontal disease in children aged under 15 was assumed to be 0.
All cases of periodontal disease were considered symptomatic. The health state reflects the intermittent nature of the symptoms.
Severe tooth loss
Severe tooth loss was based MT scores on the DMFT measure indicating fewer than 10 teeth remaining, or self-report for people with complete tooth loss (edentulism).
Prevalence for severe tooth loss originated from NSAOH dental examinations. The NSAOH 2017–18 no longer capture severe tooth loss, where only people with less than 21 teeth were captured. Hence transformations were made to deduce the dentate counts of severe tooth loss in ABDS 2018. Using NSAOH 2004–06 data for severe tooth loss, together with data published in NSAOH 2017–18 for people with edentulism and less than
21 teeth, severe tooth loss was estimated to be about 30% of those in these categories.
Other oral disorders
Estimates for other oral disorders were based on incidence of hospital separations in the 2018 calendar year. Any admissions to hospital that included the corresponding ICD-10-AM codes as principal diagnosis were counted. It was assumed that cases lasted an average of 4 weeks.
Sub-national estimates
Prevalence estimates by state/territory, remoteness and socioeconomic group were calculated from results of the National Survey of Adult Oral Health. For dental caries in children under 15, sub-national results from the Child Dental Health Survey 2009 were used. The National Child Oral Health Study 2012–14 reported caries in deciduous and adult teeth separately and the results were compared with the Child Dental Health Survey 2009, but it did not report by remoteness and socioeconomic group.
Proportions were applied to national age and sex distributions for dental caries, periodontal disease and severe tooth loss. New South Wales and Victoria were not sampled in the Child Dental Health Survey 2009, so the national rates were applied to estimate the prevalence of children with dental caries in these states.
The prevalence of other oral disorders for sub-national estimates used the same approach as for national but disaggregated directly according to remoteness area, socioeconomic group and state/territory.
2015, 2011 and 2003 estimates
As the National Survey of Adult Oral Health data were collected in 2017–18 and 2004–06, the 2003 prevalence rates were from NSAOH 2004–06, and the 2018 prevalence rates were from NSAOH 2017–18. Between these time points, linear regression was used to derive the prevalence rates for 2011 and 2015. Prevalence rates were applied to the 2015, 2011 and 2003 population structures to calculate prevalence of dental caries, periodontal disease and severe tooth loss in 2015, 2011 and 2003, respectively.
Prevalence of dental caries in children from the Child Dental Health Survey 2009 were incorporated into the 2015 and 2011 estimates. Differences in the prevalence of dental caries in children between the 2003–04 and 2009 Child Dental Health Surveys were incorporated into the 2003 estimates.
The prevalence of other oral disorders for 2015, 2011 and 2003 used the same approach as 2018, but drawn from data in the 2015, 2011 and 2003 calendar years, respectively.
Indigenous specific estimates
Due to the small sample size, age and sex-specific prevalence estimates for the Indigenous population were not directly available from the data sources used for national prevalence.
For 2018, 2011 and 2003, estimates for adult dental caries and periodontal disease were based on rate ratios of Indigenous:national rates from the National Survey of Adult Oral Health 2004–06 (Slade et al. 2007) applied to national age and sex distributions.
For 2018, 2011 and 2003 estimates for dental caries in Indigenous children were based on rate ratios of Indigenous:national rates from the Child Dental Health Survey 2009 applied to national age and sex distributions.
For severe tooth loss, Indigenous prevalence for 2018, 2011 and 2003 was based on data from AATSIHS 2012–13.
The 2018, 2011 and 2003 prevalence of other oral disorders among Indigenous Australians was based on analysis of NHMD adjusted for Indigenous under-identification using the standard adjustment factors (see Years lived with disability (YLD)).
References
ARCPOH (Australian Research Centre for Population Oral Health) 2015. Data request: Child Dental Health Survey, 2009. Accessed 6 August 2020.
ARCPOH 2019. Australia’s oral health: National Study of Adult Oral Health 2017–18. Adelaide: The University of Adelaide.
Brennan DS & Spencer AJ 2004. Disability weights for the burden of oral disease in South Australia. Pop Health Metrics 2:7.
Conway DI, McMahon AD, Robertson D & Macpherson LMD 2014. Epidemiology of dental diseases. In Ahrens W & Pigeot I (eds), Handbook of epidemiology, 2nd edition. New York: Springer.
Do LG & Spencer AJ (Eds) 2016. Oral health of Australian children: the National Child Oral Health Study 2012–14. Adelaide: University of Adelaide Press.
Ha DH, Amarasena N & Crocombe L 2013. The dental health of Australia’s children by remoteness: Child Dental Health Survey Australia 2009. Dental statistics and research series no. 63. Cat. no. DEN 225. Canberra: AIHW.
Jenkins, WMM & Papapanou, PN. 2001. Epidemiology of periodontal disease in children and adolescents, Periodontology 2000, 26, 16-32.
Slade GD, Spencer AJ & Roberts-Thomson KF 2007. Australia’s dental generations: the National Survey of Adult Oral Health 2004–06. Canberra: AIHW. Accessed 6 August 2020.
Sequelae and health states
Sequelae, health states and durations for sequelae assigned to reproductive and maternal conditions are shown below.
Table 4.35: Sequelae, health states and durations for reproductive & maternal conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
Duration for acute sequelae |
|---|---|---|---|
|
Maternal conditions |
|
|
|
|
Maternal haemorrhage |
Anaemia due to maternal haemorrhage(b) |
195, 196 |
1–3 months |
|
Surgical intervention: caesarean section |
194 |
2 weeks |
|
|
Maternal infections |
Maternal sepsis |
194 |
2 weeks |
|
Other maternal infections |
2 |
1 week |
|
|
Hypertensive disorders of pregnancy |
Hypertensive disorder |
194, 207 |
2 weeks–2 months |
|
Obstructed labour |
Surgical intervention: caesarean section |
194 |
2 weeks |
|
Early pregnancy loss |
Early pregnancy loss due to ectopic pregnancy |
194 |
2 weeks |
|
Early pregnancy loss due to other causes |
193 |
1 week |
|
|
Gestational diabetes |
Diagnosed gestational diabetes |
207 |
4 months |
|
Other maternal conditions |
Surgical intervention: caesarean section |
193 |
2 weeks |
|
Reproductive conditions |
|
|
|
|
Endometriosis |
Endometriosis |
193, 194 |
3 days per month |
|
Infertility due to endometriosis(c) |
50, 51 |
. . |
|
|
Uterine fibroids |
Anaemia due to uterine fibroids(b) |
195, 196 |
6 months |
|
|
Infertility due to uterine fibroids(c) |
50, 51 |
. . |
|
|
Symptomatic uterine fibroids |
192 |
2–6 weeks |
|
Genital prolapse |
Faecal incontinence |
48 |
. . |
|
|
Genital prolapse |
192 |
. . |
|
|
Stress incontinence |
260 |
. . |
|
Polycystic ovarian syndrome |
Infertility due to polycystic ovarian syndrome(c) |
50, 51 |
. . |
|
Polycystic ovarian syndrome |
207 |
. . |
|
|
Infertility |
Infertility(c) |
50, 51 |
. . |
|
Other reproductive conditions |
Anaemia due to other reproductive conditions(b) |
195, 196 |
. . |
|
Pain due to reproductive conditions |
192 |
2 weeks |
(a) See ABDS 2018 health states.
(b) Part of anaemia envelope.
(c) Part of infertility envelope.
Infertility envelope
Infertility was estimated for men and women aged 20–49 seeking to have a child. As infertility is a sequela of multiple conditions across the ABDS, the overall prevalence of infertility was calculated to ensure the sum of estimates for sequelae did not exceed the total—referred to as the ‘infertility envelope’. To avoid double-counting, and adhere to mutual exclusivity for each disease, the total prevalence of infertility was estimated first, then the envelope was used to estimate prevalence of infertility sequelae by other diseases.
Diseases with infertility as sequelae include endometriosis, polycystic ovarian syndrome, uterine fibroids and sexually transmitted diseases (excluding human immunodeficiency virus, or HIV). The methods used to estimate infertility due to these conditions are outlined in subsections for individual reproductive conditions.
Infertility sequelae estimates from other diseases were subtracted from this envelope. The remaining estimates were the prevalence of infertility as a disease.
Prevalence of infertility envelope, by sex
The number of women who underwent autologous cycles in 2018 was derived from the Australian and New Zealand Assisted Reproductive Database (Newman et al. 2019). Estimates were inflated to account for varying types of assisted reproductive technology.
The number of men and women seeking assistance for infertility in 2018 was adjusted to account for individual people (rather than couples) using proportions of infertility due to the female, male or both partners published in the annual report.
As an estimated 19.6% of people who experience difficulty becoming pregnant seek assisted reproductive technology (Marino et al. 2011), the prevalence from the Australian and New Zealand Assisted Reproductive Database was inflated to estimate the overall prevalence of infertility in 2018.
Age by sex distributions were the same as used in the ABDS 2011 and ABDS 2015, originally derived from GP encounters for infertility between April 2000 and March 2011 from the BEACH survey.
Prevalence of infertility envelope by subtype
Infertility was separated into primary and secondary infertility. These are definitions used by the GBD for health states and not clinical definitions of infertility (see table below).
Table 4.36: GBD health states and lay descriptions for infertility
|
GBD health state |
Lay description |
|---|---|
|
Infertility: primary |
Wants to have a child and has a fertile partner, but the couple cannot conceive |
|
Infertility: secondary |
Has at least 1 child, and wants to have more children. The person has a fertile partner, but the couple cannot conceive |
Population-based data of women who gave birth in 2018 and whether they had previously given birth (at least 20 weeks gestation or 400 grams birthweight) was applied (see table below). It is acknowledged that the distribution might slightly overestimate secondary infertility. As there is limited information on men with infertility, the same proportion as women was applied.
Table 4.37: Women who gave birth in 2018, by maternal age and parity (%)
| Maternal age | Primipara (no previous births) | Multipara (one or more previous births) |
|---|---|---|
| 20–24 years | 56.7 | 43.3 |
| 25–29 years | 49.6 | 50.3 |
| 30–34 years | 39.6 | 60.3 |
| 35–39 years | 28.4 | 71.6 |
| 40–44 years | 27.1 | 72.8 |
| 45 years and over | 40.3 | 59.5 |
Source: National Perinatal Data Collection.
Infertility due to sexually transmitted infections (excluding HIV)
Due to the limited information on male infertility, infertility due to sexually transmitted infections was estimated in females only.
Based on clinical advice, it was assumed that 90% of tubal factor infertility is caused by sexually transmitted infections. Current literature reports 7.0%–9.8% of female infertility attributable to tubal disease (Hafner & Pelzer 2011). This estimate (average 8.4%) was proportioned from the total infertility envelope to be due to other sexually transmitted infections (excluding HIV).
This disease was further proportioned based on GBD estimates into chlamydia (30%), gonorrhoea (20%) and other sexually transmitted infections (50%) based on GBD estimates.
Prevalence estimation
Maternal conditions
Incidence of maternal conditions in 2018 were obtained from the NHMD (unless otherwise stated), with definitions based on ICD-10-AM or ACHI codes or from the Medicare Benefits Schedule. Early pregnancy loss was defined as losses (both spontaneous and medically or surgically induced) before a gestational age of 20 weeks. Medical abortions performed via use of pharmaceuticals were included for 2018 and 2015 using PBS data, but not for 2003 or 2011, due to the introduction of ‘MS-2 step’ pharmaceuticals in 2013.
As maternal conditions are generally measured in terms of incident cases, prevalence estimates were produced by applying a duration of health loss (see Sequelae, health states and durations for reproductive & maternal conditions). Durations to derive prevalence from incidence data were the same as those used in the ABDS 2011, unless otherwise stated.
Maternal haemorrhage
Incidence of maternal haemorrhage was assumed to result in acute anaemia. Moderate anaemia was defined as cases of maternal haemorrhage including post-haemorrhagic anaemia (ICD-10-AM: D62), whereas mild cases did not indicate post-haemorrhagic anaemia.
It was assumed it would take 3 months to return to full health from mild anaemia. Severe cases would be treated with blood transfusion, with resulting anaemia lasting at most 1 month. Cases resulting in a caesarean section were given 2-week duration, consistent with surgical interventions with the same health state.
Maternal infections
Cases of maternal sepsis (defined as separations with a diagnosis of O41.1 and O85) were assumed to have health loss of 2 weeks. Other maternal infections—urinary tract infections, vaginitis and wound infections post-delivery—were assumed to have 1 week’s health loss.
Hypertensive disorders of pregnancy
Moderate/severe hypertensive disorders (eclampsia and pre-eclampsia) were assumed to have 2 weeks health loss. Remaining hypertensive disorder estimates were given a duration of 2 months. If multiple hospitalisations occurred for this condition, this could have overestimated hypertensive disorders incidence.
Early pregnancy loss
Cases of early pregnancy loss due to ectopic pregnancy were derived from the NHMD. As evidence suggests 23.3% of ectopic pregnancies are treated in emergency departments and do not go on to be admitted to hospital (Goller et al. 2018), estimates derived from admitted patient data were inflated to account for those that experienced ectopic pregnancy but were not admitted.
Cases of surgically induced early pregnancy loss were derived from public patient hospital admissions for medical abortions, as well as Medicare claims data, where relevant (AIHW National Perinatal Statistics Unit 2005). Queensland provided estimates derived from linked data.
Adjustments for unclaimed procedures in New South Wales, Victoria, Tasmania, Western Australia and the Australian Capital Territory were applied to Medicare Benefits Schedule data (method from AIHW NPSU 2005). Non-hospital claims for these jurisdictions were inflated by 7.5% to account for unclaimed procedures (Shankar et al. 2017). Public patient admissions were added to adjusted Medicare data and PBS data to derive incidence of abortion in 2018.
Medically induced abortions were included for 2018 and 2015 only using PBS data for MS-2 Step pharmaceuticals.
It was assumed abortion was performed at 20 weeks or less, but as some state regulations allow this to be performed after 20 weeks, this might have resulted in a slight overestimate. Due to data limitations, cases of spontaneous early pregnancy loss were restricted to hospitalised instances. This might result in an underestimate of health loss due to this sequela.
Gestational diabetes
The incidence of gestational diabetes was estimated using the number of hospital separations where gestational diabetes (O24.4) was a diagnosis alongside a delivery (O80–O84, Z37). Gestational diabetes is identified using the AIHW’s matrix for assigning diabetes in pregnancy status (AIHW 2019b).
Other maternal conditions
Remaining maternal conditions included placental disorders, labour complications and maternal care. An average duration of 2 weeks was applied to derive prevalence.
Reproductive conditions
Hospital data, longitudinal studies, GP visits and epidemiological studies were used to derive prevalence. These sources require a diagnosis; therefore, undiagnosed conditions were not included.
Endometriosis
The prevalence of endometriosis in women aged 40–44 was derived from the Australian Longitudinal Study on Women’s Health (ALSWH), a longitudinal cohort study, linked with MBS, PBS and/or admitted patient hospital data (AIHW 2019a). This prevalence was previously derived from ALSWH data that had not been linked. The cohort used for prevalence estimates was born between 1973 and 1978. Age distributions derived from the NHMD were applied to these estimates, to derive prevalence by age. Age distribution has been derived from GP visits previously.
Endometriosis severity was based on surgical intervention. Hospitalised cases of endometriosis in 2018 with a relevant procedure were derived from the NHMD. Duration of health loss was assumed to be 36 days (based on the average duration of secondary dysmenorrhea of 3 days per month). Surgical cases were subtracted from the total prevalence to derive non-surgical cases.
Infertility estimates were derived from the ALSWH, with an estimated 11.7% of women with endometriosis reporting infertility issues. These estimates were subtracted from the infertility envelope. This is further discussed in the infertility section.
Polycystic ovarian syndrome
Polycystic ovarian syndrome in women aged 34–39 was derived from the ALSWH. The cohort used for prevalence estimates were born between 1973 and 1978. Age distributions were derived from BEACH data and applied to these estimates, to determine prevalence by age.
Infertility estimates were derived from the ALSWH, with 14.5% of women with polycystic ovarian syndrome reporting infertility issues. These estimates were subtracted from the infertility envelope (see Infertility section).
Uterine fibroids
It was assumed people with burdensome uterine fibroids in 2018 would be hospitalised to remove fibroids. Therefore, incidence was derived from the NHMD based on ICD-10-AM codes with a relevant procedure.
Durations were based on surgical procedures. Abdominal hysterectomies received a duration of 6 weeks—due to more extensive recovery—while all other procedures received a duration of 2 weeks.
An estimated 2.5% of infertility was assumed to be due to uterine fibroids (Buttram & Reiter 1981), and this was subtracted from the infertility envelope as previously described. More recent studies suggest the impact of fibroids on fertility is unknown (for example, Purohit & Vigneswaran 2016) and do not report a proportion. However, it was decided to use the 1981 estimate.
The proportion of women with uterine fibroids who had anaemia was based on the Uterine Bleeding and Pain Women’s Research Study (Zimmerman et al. 2012). The average of the proportion of women with prolonged or heavy bleeding symptoms was used to apportion women with uterine fibroids experiencing anaemia. This proportion was applied to the burdensome uterine fibroids estimate, to derive the prevalence of anaemia due to uterine fibroids. The same severity distribution used for iron-deficiency anaemia was used to apportion mild anaemia and moderate anaemia.
Genital prolapse
Symptomatic genital prolapse: The prevalence of genital prolapse in Australia was based on prevalence rates obtained from the NZBDS (NZMOH 2012) applied to the 2018 Australian Estimated Residential Population. Due to limited data, male estimates were calculated using the male-to-female genital prolapse hospitalisations ratio in the year 2018, with procedure codes related to genital prolapse.
Stress incontinence due to genital prolapse: Stress incontinence in males was not included as this was assumed to be prostate related. The age-specific proportion of females with genital prolapse who experience stress incontinence was obtained from Lawrence and others (2008) and applied directly to females symptomatic prolapse estimates.
Faecal incontinence due to genital prolapse: Estimates of faecal incontinence from Harvie et al. (2018) were applied to total female and male symptomatic prolapse estimates. The age-distribution was obtained from Lawrence et al. (2008) and applied to the total proportion with faecal incontinence due to genital prolapse.
Other reproductive conditions
Remaining ICD-10 codes were categorised into whether they resulted in anaemia, pain, or both anaemia and pain, were captured elsewhere, or did not cause burden. Conditions identified as resulting in pain, anaemia or both were included in estimations.
The prevalence rate of ‘other reproductive conditions’ by age, sex and sequela as estimated in the ABDS 2011, was applied to the 2018 Australian Estimated Residential Population to derive estimates in year 2018. The original estimates from ABDS 2011 were derived from the BEACH survey using the proportion of general practice visits for these conditions between March 2000 and April 2011. Estimates for people aged under 15 were based on population distributions, and estimates for people aged 75 and over were modelled on trend analyses. The severity distribution of iron-deficiency anaemia was applied to anaemia (see anaemia envelope discussion in the blood & metabolic disease group).
Sub-national estimates
Sub-national estimates for most reproductive and maternal conditions were derived directly from the NHMD in 2018, or from age and sex ratios in the NHMD where direct derivation was not possible. State and territory estimates for abortions performed in non-hospital settings were derived from Medicare claims data and adjusted to account for legislative differences.
2015, 2011 and 2003 estimates
Estimates using hospital separations data used the same method as for 2018, but with 2015, 2011 and 2003 NHMD data.
Estimates using ALSWH, BEACH and epidemiological studies used the same rates or proportions as for 2018, applied to the 2011 or 2003 population, unless otherwise stated. This is because using earlier Australian Longitudinal Study on Women’s Health surveys and BEACH data gave implausible estimates.
For endometriosis, prevalence derived from ALSWH linked data vary by year: 11.4% of women aged 40–44 in 2018 and 2015, and 9.6% of women aged 35–39 in 2011 and 2003 (AIHW 2019a).
Indigenous specific estimates
The same methods and data sources were used to derive Indigenous estimates, except where noted. Indigenous estimates based on hospital separations data (see above) were adjusted for under-identification using standard adjustment factors (see Years lived with disability (YLD)).
Estimates for polycystic ovarian syndrome were based on Indigenous: national rate ratios applied to national prevalence rates. The rate ratio for endometriosis was obtained from hospital separations data, and from epidemiological studies for polycystic ovarian syndrome.
Due to lack of data, Indigenous prevalence of endometriosis, genital prolapse and infertility was obtained by applying the national distribution directly to the Indigenous population. This assumes the underlying rate is the same between the Indigenous and non-Indigenous populations.
References
AIHW (Australian Institute of Health and Welfare) 2019a. Endometriosis in Australia: prevalence and hospitalisations. Cat. no. PHE 247. Canberra: AIHW.
AIHW 2019b. Incidence of gestational diabetes in Australia. Cat. no. CVD 85. Canberra: AIHW. Viewed 22 November 2019.
AIHW National Perinatal Statistics Unit: Grayson N, Hargreaves J & Sullivan EA 2005. Use of routinely collected national data sets for reporting on induced abortion in Australia. Perinatal statistics series no. 17. Cat. no. PER 30. Sydney: AIHW Perinatal Statistics Unit.
Buttram V & Reiter R 1981. Uterine leiomyomata: etiology, symptomatology, and management. Fertility and Sterility 36(4):433–445.
Goller JL, De Livera AM, Guy RJ, Low N, Donovan B, Law M et al. 2018. Rates of pelvic inflammatory disease and ectopic pregnancy in Australia, 2009–2014: ecological analysis of hospital data. Sexually Transmitted Infections 94(7):534–41.
Hafner LM & Pelzer ES 2011. Tubal damage, infertility and tubal ectopic pregnancy: chlamydia trachomatis and other microbial aetiologies, ectopic pregnancy. In: Kamrava M (ed.). Modern diagnosis and management. InTech; online. Viewed 24 April 2015.
Harvie HS, Lee, DD, Andy UU, Shea JJ & Arya LA 2018. Validity of utility measures for women with pelvic organ prolapse. American Journal of Obstetrics and Gynecology. 218:119.e1–8.
Lawrence JM, Lukacz ES, Nager CW, Hsu J-WY & Luber KM 2008. Prevalence and co occurrence of pelvic floor disorders in community-dwelling women. Obstetrics & Gynecology 111(3):678–85.
Marino JL, Vivienne MM, Rumbold AR & Davies MJ 2011. Fertility treatments and the young women who use them: an Australian cohort study. Human Reproduction 26(2):473–79.
Newman EN, Fitzgerald O, Paul RC & Chambers GM 2019. Assisted reproductive technology in Australia and New Zealand 2017. Sydney: National Perinatal Epidemiology and Statistics Unit, the University of New South Wales Sydney.
NZMOH (New Zealand Ministry of Health) 2012. Ways and Means: A report on methodology from the New Zealand Burden of Diseases, Injuries and Risk Factors Study, 2006–2016. Wellington: Ministry of Health.
Purohit P & Vigneswaran K 2016. Fibroids and Infertility. Current Opinion in Obstetric and Gynecology 5:81–88.
Shankar M, Black KI, Goldstone P, Hussainy S, Mazza D, Petersen K, Lucke J & Taft A 2017. Access, equity and costs of induced abortion services in Australia: a cross-sectional study. Australian and New Zealand Journal of Public Health 41(3):309–14.
Zimmerman A, Bernuit D, Gerlinger C, Schaefers M & Geppert K 2012. Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BioMed Central Women’s Health 12(6):e1–11.
Sequelae and health states
Sequelae and health states assigned to respiratory conditions are shown in the table below. As most of these conditions (except for upper respiratory conditions) are chronic, health loss was assumed to apply for the whole year.
Table 4.38: Sequelae and health states for respiratory diseases
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
|---|---|---|
|
Asthma |
Asthma |
52, 53, 54 |
|
Chronic obstructive pulmonary disease (COPD) |
COPD |
55, 56, 57 |
|
Sarcoidosis |
Sarcoidosis |
262, 55, 56, 57 |
|
Interstitial lung disease |
Interstitial lung disease |
55, 56, 57 |
|
Asbestosis |
Asbestosis |
55, 56, 57 |
|
Silicosis |
Silicosis |
55, 56, 57 |
|
Other pneumoconiosis |
Other pneumoconiosis |
55, 56, 57 |
|
Upper respiratory conditions |
Upper respiratory |
262, 207 |
|
Other respiratory disease |
Other respiratory |
207 |
(a) See ABDS 2018 health states.
Prevalence estimation
Asthma and upper respiratory conditions
The NHS 2017–18 was the main data source used to estimate the national prevalence of asthma and upper respiratory conditions. The NHS did not include people who lived in institutionalised facilities, such as hospitals or aged care facilities, so estimates on the prevalence of asthma and upper respiratory disease (mainly in the older age groups) in these institutions were not included.
To generate prevalence for the national population, rates derived from the surveys were applied to the national population.
Asthma
Prevalence of asthma was based on self-reported symptoms of diagnosed asthma in the previous 12 months. As this data source did not provide levels of control of asthma consistent with the available health states, the severity distribution was based on an Australian cross‑sectional web-based survey (Reddel et al. 2015). The following proportions were used: 54.4% controlled, 22.6% partially controlled and 23.0% uncontrolled. Health loss was assumed to last for the entire year.
Upper respiratory conditions
Upper respiratory conditions include hayfever, sinusitis and other upper respiratory tract disorders. Prevalence was derived from the proportion of participants who reported having an upper respiratory condition that had lasted, or was expected to last, at least 6 months. The total duration of health loss from upper respiratory conditions was assumed to be 3 months in the year. Health loss was assigned to 33% of cases based on findings from allergic rhinitis studies in the United States and Australia (Meltzer et al. 2012; Tan et al. 2017), with the remainder considered asymptomatic.
Chronic obstructive pulmonary disease
Prevalence for COPD was based on measured data from the Australian arm of the Burden of Obstructive Lung Disease (BOLD) Study (Toelle et al. 2013), provided by the Woolcock Institute of Medical Research. This study involved a prevalence survey of nearly 3,500 randomly selected men and women aged 40 and over. It was done in 6 locations around Australia between 2007 and 2010, and measured spirometric lung function after an inhaled bronchodilator was administered. Severity distributions were based on spirometric function in accordance with the BOLD study procedure (Buist et al. 2007).
Prevalence rates calculated using revised data weighted to the 2016 Census population supplied by the BOLD study team (Toelle et al. 2021) were applied to the 2018 ERP to generate prevalence estimates for the 2018 reference year. An assumption was made that the rate of COPD in Australia had not changed significantly between these time points.
The BOLD study experts advised that the rate of COPD in older people should increase with age, and the rates from GBD support this, so the data from BOLD was modelled using a polynomial curve for each sex to estimate rates for people aged 75 and over. This was done for the BOLD data weighted to the 2016, 2011 and 2006 populations supplied to the AIHW by the BOLD investigators.
Sarcoidosis, asbestosis, silicosis, other pneumoconiosis and interstitial lung disease
These conditions are rare and so their prevalence cannot be reliably estimated in population health surveys. Instead, prevalence estimates were based on mortality and hospitalisation data. Persons-to-separations ratios derived using linked hospitalisations and deaths data from the NIHSI AA v0.5 were applied to the national hospitalisations to account for repeat admissions per person.
Mortality and hospitalisation data were used to estimate the prevalence of moderate and severe cases for these diseases. Prevalence for the mild or asymptomatic health states was then derived, by extrapolating these estimates for moderate and severe disease, based on severity distributions obtained from GBD 2015 data (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators 2016). The severity distributions used for sarcoidosis and interstitial lung disease are listed below.
Table 4.39: GBD severity distributions (%) for sarcoidosis
|
|
Asymptomatic |
Mild |
Moderate |
Severe |
|---|---|---|---|---|
|
Sarcoidosis – GBD 2013 |
23.9 |
55.0 |
16.0 |
5.1 |
|
Sarcoidosis – GBD 2015 |
22.2 |
50.8 |
14.8 |
12.2 |
Notes
- In the GBD study, pulmonary sarcoidosis and interstitial lung disease are grouped together.
- The change in severity distribution between the GBD 2013 and the GBD 2015 is a result of a methodology change in 2015 in which secondary diagnosis data in hospitalisation data were used.
The severity distributions used for asbestosis, silicosis and other pneumoconiosis are listed below.
Table 4.40: GBD severity distributions (%) for asbestosis, silicosis and other pneumoconiosis
|
|
Asymptomatic |
Mild |
Moderate |
Severe |
|---|---|---|---|---|
|
Asbestosis – GBD 2013 |
30.8 |
43.9 |
17.8 |
7.5 |
|
Asbestosis – GBD 2015 |
23.0 |
32.7 |
12.9 |
31.4 |
|
Silicosis – GBD 2013 |
31.8 |
44.8 |
17.2 |
6.2 |
|
Silicosis – GBD 2015 |
23.4 |
33.2 |
13.2 |
30.2 |
|
Other pneumoconiosis – GBD 2013 |
29.0 |
41.6 |
16.2 |
13.3 |
|
Other pneumoconiosis – GBD 2015 |
22.8 |
32.3 |
12.8 |
32.1 |
Notes
- In the GBD distributions, ‘Other pneumoconiosis’ did not include ‘Coal workers pneumoconiosis’, but the proportions were very similar.
- The change in severity distribution between the GBD 2013 and the GBD 2015 is a result of a methodology change in 2015 in which secondary diagnosis data in hospitalisation data were used.
Other respiratory conditions
The prevalence of other respiratory conditions was derived using the YLD:YLL ratio for the following identified conditions: sarcoidosis, asbestosis, silicosis and other pneumoconiosis and interstitial lung disease. The ratio was applied to YLL for other respiratory conditions identified using the ICD-10 codes outlined in Table 2.1.
Sub-national estimates
National estimates were apportioned into each state/territory, remoteness area and socioeconomic group, based on the proportions obtained from either survey (NHS) or hospitalisation (NHMD) data. Due to the small number of cases for asbestosis, silicosis and other pneumoconiosis, data from the NHMD and the NMD were used for all these diseases and the proportions applied to national estimates for each disease.
Given that the NHS did not include people living in Very remote areas an adjustment based on population size was performed to inflate prevalence estimates to account for these people for asthma and upper respiratory conditions.
2015, 2011 and 2003 estimates
The same methods used for the 2015 estimates were used for 2011 estimates of non-fatal burden respiratory disease. The severity distributions used for 2011 estimates are included in the tables with the distributions used for 2015 estimates so they can be easily compared. It is important to note that some of the differences between 2015 and 2011 estimates will be due to differences in the severity distributions, particularly for sarcoidosis, asbestosis, silicosis, other pneumoconiosis and interstitial lung disease.
National 2003 estimates of asthma and upper respiratory conditions used a similar method to that used for 2018, 2015 and 2011 estimates but drew on the NHS 2004–05. Estimates of COPD were also based on the BOLD study, with rates weighted to the 2006 Census population applied to the 2003 population. The remaining conditions used a similar method but drew on 2003 hospital data.
Indigenous specific estimates
Indigenous estimates of asthma and upper respiratory conditions for 2018, 2011 and 2003 were based on self-reported data from the 2018–19, 2012–13 and 2004–05 National Aboriginal and Torres Strait Islander Surveys, using similar methods as for national estimates. As there were no Indigenous-specific severity distributions, the national severity distributions were assumed. Severity distributions for asthma were further adjusted in those aged 30 and over to reflect higher severities in older age groups. These adjustments were based on hospitalisations data.
Indigenous prevalence estimates and severity distributions for chronic obstructive pulmonary disease for 2018, 2011 and 2003 were based on the results of a cross-sectional BOLD study of the Indigenous population conducted in the Kimberley region of Western Australia (Cooksley 2013) and using age-sex distributions from hospitalisations data. As hospitalisations and survey data indicate that Indigenous Australians experience chronic obstructive pulmonary disease at younger age groups, estimates were adjusted to include prevalence in ages less than 40 years.
Sarcoidosis and intestinal lung disease are very rare in the Indigenous population (MacGinley & Allen 1997). Indigenous prevalence estimates for these conditions in 2018, 2011 and 2003 were based on hospitalisations and mortality data adjusted for under-identification using standard adjustment factors.
Prevalence estimates for asbestosis, silicosis and other pneumoconiosis (including coal worker’s lung) were also based on hospitalisations and mortality data adjusted for under-identification using standard adjustment factors.
References
Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM et al. 2007. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. The Lancet 370:741–50.
Cooksley NAJB, Atkinson D, Marks GB, Toelle BG, Reeve D, Johns DP et al. 2015. Prevalence of airflow obstruction and reduced forced vital capacity in an Aboriginal Australian population: The cross-sectional BOLD study. Respirology 20(5):766–74.
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators 2016. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Supplementary appendix. The Lancet 388:1545–602.
MacGinley RJ and Allen RKA 1997. Sarcoidosis in an Australian Aborigine and a Torres Strait Islander. Sarcoidosis Vasculitis and Diffuse Lung Disease 14:83–85.
Meltzer EO, Gross GN, Katial R & Storms WW 2012. Allergic rhinitis substantially impacts patient quality of life: findings from the Nasal Allergy Survey Assessing Limitations. Journal of Family Practice 61(2 Suppl):S5–10.
Reddel HK, Sawyer SM, Everett PW, Flood PV & Peters MJ 2015. Asthma control in Australia: a cross-section web-based survey in a nationally representative population. Medical Journal of Australia 202(9):492–6.
Tan R, Cvetkovski B, Kritikos V, Price D, Yan K, Smith P et al. 2017. Identifying the hidden burden of allergic rhinitis (AR) in community pharmacy: a global phenomenon. Asthma Research and Practice 21:3–8.
Toelle BG, Xuan W, Bird TE, Abramson MJ, Atkinson SN, Burton DL et al. 2013. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) Study. Medical Journal of Australia 198(3):144–8.
Toelle BG, Ampon RD, Abramson MJ, James AL, Maguire GP, Wood-Baker R et al. 2021. Prevalence of chronic obstructive pulmonary disease with breathlessness in Australia: weighted using the 2016 Australian census. Internal Medicine Journal 51:784–7.
Sequelae and health states
Sequelae and health states assigned to skin disorders are shown below. Where these conditions are chronic, health loss was assumed to apply for the whole year (12 months).
Table 4.41: Sequelae, health states and durations for skin conditions
|
Disease |
Sequela |
ABDS 2018 health state identifier(a) |
Duration |
|---|---|---|---|
|
Dermatitis and eczema |
Eczema |
204, 205, 262 |
12 months |
|
Psoriasis |
Psoriasis |
204, 205, 262 |
12 months |
|
Acne |
Acne |
201, 202, 262 |
12 months |
|
Ulcers |
Decubitus ulcer (pressure ulcer) |
204, 205, 206, 262 |
Various, depending on stage of ulcer |
|
|
Other chronic skin ulcer |
39 |
12 months |
|
Skin infections (including cellulitis) |
Severe skin infection |
3 |
2 weeks |
|
Scabies |
Scabies |
204, 205 |
4.5 months |
|
Other skin disorders |
Other skin disorder: acute |
3 |
2 weeks |
|
|
Other skin disorder: chronic |
202 |
12 months |
(a) See ABDS 2018 health states.
Prevalence estimation
Dermatitis and eczema
The prevalence of eczema was based on a study that conducted clinical examinations for non‑malignant skin conditions in Australian adults living in central Victoria (Plunkett et al. 1999). The overall age-and-sex adjusted prevalence rate (31.6%) was applied to the Australian estimated resident population for all age groups, including children.
The severity distribution for dermatitis and eczema in adults was modified based on the severity of atopic dermatitis reported by Plunkett et al. (1999). The modified severity distribution takes into account that severe atopic dermatitis is likely to be the only dermatitis or eczema condition that would correspond to the most severe health state.
The severity distribution in children was based on the study by Marks et al. (1999a), which investigated atopic eczema in Australian school students (aged 4–18). The study reported four severities (minimal, mild, moderate and severe). Based on expert advice, the minimal and mild groups were combined into the least severe health state. Moderate and severe severities were aligned to the other health states, using the same approach as outlined for adults (only severe atopic dermatitis corresponds to the most severe health state).
Psoriasis
Prevalence was based on the NHS 2017–18 self-reported psoriasis that had lasted, or was expected to last, at least 6 months. Age-and-sex specific prevalence rates were modelled using the NHS 2017–18 psoriasis counts and applied to the Australian estimated resident population to calculate the national prevalence. Although the NHS 2017–18 did not report on Very remote areas, prevalence estimates were modelled to account for these areas.
The severity distribution of psoriasis was based on results from a study of 1,700 adults from several European countries who self-reported having had a diagnosis of psoriasis. Severity of psoriasis was assessed using the Dermatological Life Quality Index (Puig et al. 2017). Participants who were classified as ‘no impact’ in the study were considered to have minimal psoriasis. Participants who were classified as ‘small’ or ‘moderate’ impact were considered to have mild psoriasis. Participants who were classified as ‘very large’ or ‘extremely large’ impact were considered to have moderate/severe psoriasis. Proportions of the number of people in each severity were applied to the national prevalence estimates.
Acne
The prevalence of acne in adults was based on a study that conducted clinical examinations of non-malignant skin conditions in Australian adults living in central Victoria (Marks et al. 1999b; Plunkett et al. 1999). Age-specific prevalence rates of acne from this study were applied to the Australian estimated resident population for adults aged 20 and over. The severity distribution for adults was based on proportions that were calculated using scores from the Dermatology Life Quality Index (Marks et al. 1999b) and applied to the estimates.
The prevalence of acne in children was based on a study of clinical examination of Australian school students (aged 4–18) (Kilkenny et al. 1998). Age- and sex-specific prevalence rates were applied to the Australian estimated resident population for those aged 5–19 years. For younger children (0–4 years), the prevalence of acne was assumed to be zero (0). The severity distribution for children was based on proportions calculated using scores from the Acne Disability Index (Marks et al. 1999b) and applied to the estimates.
Ulcers
Pressure ulcers
There are 3 main settings where people are at risk of developing pressure ulcers: patients admitted to hospital; people living in residential care facilities (older Australians and people with disability); and people receiving home-based care in the community (a similar cohort to those living in residential care facilities). The prevalence of pressure ulcers was modelled separately for each of these settings based on different data sources (see table below). These figures were added together to produce the total prevalence of pressure ulcers in Australia.
Table 4.42: Summary of data sources for modelling the prevalence of pressure ulcers by setting, 2018
|
Setting |
Prevalence |
Age distribution |
Severity |
Duration (if required) |
|---|---|---|---|---|
|
Hospitals |
NSW 2018 Pressure Injury Point Prevalence Survey (CEC 2019) Qld 2018 Bedside Audit (Qld Health 2019) WA 2014 PI Point Prevalence Survey (Ferguson et al. 2019) |
NHMD 2018
|
NHMD 2018 |
Dealey et al. 2012 |
|
Residential aged care |
NSW 2018 Pressure Injury Point Prevalence Survey (CEC 2019) |
Santamaria et al. 2009 |
GEN Aged care data 2019 (AIHW 2020) |
No duration required |
|
Home-based care |
NSW 2018 Pressure Injury Point Prevalence Survey (CEC 2019) |
Asimus & Li 2011 |
Asimus & Li 2011 |
No duration required |
Pressure ulcers in the hospital: The prevalence of pressure ulcers acquired in hospitals was based on the proportions of hospital-acquired pressure ulcers from 3 jurisdictions. The proportions of pressure ulcers in New South Wales (CEC 2019), Queensland (Queensland Health 2019) and Western Australia (Ferguson et al. 2019) were applied to the number of hospitalisations (from the NHMD) in these states in 2018 and extrapolated to the remaining states/territories. This estimated the total national prevalence of pressure ulcers in the hospital setting. The age-sex distribution and the severity distribution were both obtained from NHMD hospitalisations data for pressure ulcers (ICD-10-AM: L89) in 2018.
Durations for each stage were based on the mean expected time to heal from ulcers, as reported by Dealey et al. (2012), with more severe ulcers modelled to progress to less severe stages during the healing process. For example, it was estimated that a stage 4 ulcer would take 155 days to heal, and that this was made up of time spent in stages 3, 2 and 1 as healing progressed.
Pressure ulcers in residential age care: The national prevalence of pressure ulcers in residential aged care was based on the proportion of pressure ulcers acquired while in NSW residential aged care facilities in 2018 (CEC 2019). This proportion was applied to the residential aged care population in Australia as at 30 June 2018 (AIHW 2019). The age distribution was modelled based on the findings of Santamaria and others (2009). The severity distribution was based on Residential Aged Care Quality Indicator data pertaining to the July–September 2019 period (AIHW 2020).
Pressure ulcers in home-based care: The national prevalence of pressure ulcers in home-based care was based on the proportion of pressure ulcers acquired while in NSW community and outpatient facilities in 2018 (CEC 2019). This proportion was applied to the home care population in Australia as at 30 June 2018 (AIHW 2019). The age distribution was modelled using data from an Australian study of patients receiving care from community nurses (Asimus & Li 2011). The severity distribution was also obtained from this study (Asimus & Li 2011).
Chronic skin ulcers
The prevalence of chronic skin ulcers was based on GP encounters for chronic skin ulcers reported in a BEACH study (Harrison et al. 2013). The crude rates from the survey were weighted and modelled according to the method used by Harrison et al. (2013) to estimate the prevalence of chronic conditions. This estimate accounted for the frequency of GP visits in the population and also for those who did not visit a GP in the year, so the prevalence is generalised to the total population in Australia. To avoid double‑counting of chronic ulcers caused by diabetes (diabetic foot ulcers), the proportion of diabetic foot ulcers was removed from the chronic skin ulcer prevalence.
Skin infections
The prevalence of skin infections was based on hospital separations (from the NHMD) in 2018. Separations with a principal diagnosis for skin infections (ICD-10-AM: A46, B08.1, B08.4, H00.0, H60.0–H60.1, J34.0, L00–L04, L08.0–L08.9) were included. A duration of 2 weeks out of 1 year was applied to the separations to estimate the point prevalence of skin infections.
Scabies
Two data sources were used in the estimation of scabies prevalence—the NHMD and a study that measured scabies prevalence before and after two ivermectin mass drug administrations in a remote Australian Aboriginal island community (Kearns et al. 2015). Hospitalisations data were inflated to account for non-hospitalised cases in the community with a duration of 4.5 months applied to each case. Prevalence estimates derived using data from Kearns et al. (2015) were added to the hospitalisation estimates to account for a higher prevalence of scabies in Very remote areas.
Other skin disorders
The prevalence of other acute skin disorders was based on hospital separations (from the NHMD) in 2018. Separations with a principal diagnosis of other acute skin disorders (ICD-10-AM: L05, L10–L13, L28–L29, L41–L45, L50–60, L62–L68, L71–L75, L80–L88, L90–L95, L98.0–L98.3, L98.5–L98.9 and L99) were included. A duration of
2 weeks out of 1 year was applied to the separations to estimate the point prevalence.
Age-and-sex specific prevalence rates for other chronic skin disorders were modelled using the NHS 2017–18 counts of conditions reported as ‘other diseases of skin and subcutaneous tissue’. It was estimated that about half of these conditions would correspond to ‘other chronic skin disorders’ as defined in the ABDS 2018. The rates were applied to the Australian estimated resident population to obtain the national prevalence of other chronic skin disorders.
Sub-national estimates
For dermatitis & eczema, acne and skin ulcers, the proportions of the 2018 Australian estimated resident population in each state/territory, remoteness area and socioeconomic group were applied to the national estimates in order to obtain the sub-national estimates. This method was used because there was a lack of prevalence data specific to the sub-national levels for these conditions.
For skin infections and other acute skin disorders, hospitalisations in 2018 by sub-national groups were obtained from the NHMD and a duration of 2 weeks was applied to the separations to obtain the point prevalence.
For psoriasis and other chronic skin disorders, proportions of the prevalence at sub-national levels were derived from the NHS 2017–18 counts and applied to the national estimates to produce the sub-national point prevalence.
For scabies, national prevalence was split into state/territory and socioeconomic sub-national estimates based on observed splits in hospitalisations data. For scabies remoteness sub-national estimates, national scabies prevalence based on hospitalisations was split based on observed splits in hospitalisations data and all of the Kearns et al. estimates were assigned to Very remote areas.
2015, 2011 and 2003 estimates
Where available and appropriate, the data sources used for the 2003, 2011 and 2015 estimates were the same as those used for the 2018 estimates.
For dermatitis & eczema and acne, the same prevalence rates (sourced from the same studies) were applied to the 2003, 2011 and 2015 populations. For skin infections and other acute skin disorders, 2003, 2011 and 2015 hospitalisations obtained from the NHMD were used to calculate the point prevalence.
For psoriasis and other chronic skin disorders, the prevalence was based on data sourced from the NHS 2004–05, AHS 2011–12 and NHS 2014–15 and used for the 2003, 2011 and 2015 estimates respectively.
For pressure ulcers, the methods of estimating prevalence for 2003, 2011 and 2015 were largely the same as the methods used for the 2018 reference year, however, different data sources were used (see below). The prevalence of pressure ulcers was not always available for the specific reference year, in which case the closest year was used.
There was a notable change in the methods used to estimate prevalence in the ABDS 2018 compared to in the ABDS 2015 and this was updated for all reference years. This change was to use the prevalence of pressure ulcers acquired within each setting (hospital, residential aged care, home care) instead of using the overall prevalence of pressure ulcers reported for each setting. This change was made to avoid double counting of pressure ulcers which may be present within one setting, but were acquired in another. Population counts for residential aged care and home-based care were sourced from AIHW GEN Aged care data for each reference year.
Table 4.43: Summary of data sources for modelling the prevalence of pressure ulcers by setting, 2015, 2011 and 2003
|
Setting |
Prevalence |
Age distribution |
Severity |
Duration (if required) |
|---|---|---|---|---|
|
Hospitals 2015 |
NSW 2016 Pressure Injury Point Prevalence Survey (CEC 2017) Qld 2015 Bedside Audit (ASCQHC 2018) WA 2014 Pressure Injury Point Prevalence Survey (Ferguson et al. 2019) |
NHMD 2015
|
NHMD 2015
|
Dealey et al. 2012 |
|
Residential aged care 2015 |
NSW 2016 Pressure Injury Point Prevalence Survey (CEC 2017) |
Santamaria et al. 2009 |
GEN Aged care data 2019 (AIHW 2020) |
No duration required |
|
Home-based care 2015 |
NSW 2016 Pressure Injury Point Prevalence Survey (CEC 2017) |
Asimus & Li 2011 |
Asimus & Li 2011 |
No duration required |
|
Hospitals 2011 |
Mulligan et al. 2011 (includes data for WA and NSW) Qld 2011 Bedside Audit (Qld Health 2012) |
NHMD 2011 |
Pressure ulcer point prevalence surveys (SA Health 2007, VQC 2006, Mulligan et al. 2011) |
Dealey et al. 2012 |
|
Residential aged care 2011 |
Santamaria et al. 2009 (adjusted to exclude ulcers acquired elsewhere) |
Santamaria et al. 2009 |
GEN Aged care data 2019 (AIHW 2020) |
No duration required |
|
Home-based care 2011 |
Asimus & Li 2011 (adjusted to exclude hospital-acquired ulcers) |
Asimus & Li 2011 |
Asimus & Li 2011 |
No duration required |
|
Hospitals 2003 |
Mulligan et al. 2011 (includes data for Qld, WA, NSW, Vic and SA) |
NHMD 2003 |
Pressure ulcer point prevalence surveys (SA Health 2007, VQC 2006, Mulligan et al. 2011) |
Dealey et al. 2012 |
|
Residential aged care 2003 |
Santamaria et al. 2009 (adjusted to exclude ulcers acquired elsewhere) |
Santamaria et al. 2009 |
GEN Aged care data 2019 (AIHW 2020) |
No duration required |
|
Home-based care 2003 |
Asimus & Li 2011 (adjusted to exclude hospital-acquired ulcers) |
Asimus & Li 2011 |
Asimus & Li 2011 |
No duration required |
For other chronic skin ulcers, the same method based on the study by Harrison et al. (2013) was used to estimate the prevalence. BEACH data from 2003 was used for the 2003 estimates, whereas BEACH data from 2011 was used for the 2011 and 2015 estimates.
For scabies, inflated hospitalisations (from NHMD) from the relevant reference year were used for the 2003, 2011 and 2015 estimates with the addition of estimates derived from rates from Kearns et al. study (2015). Estimates derived from Kearns et al. (2015) were based on rates applied to the Indigenous population for Very remote areas for each year.
Indigenous specific estimates
Due to a lack of available data on Indigenous prevalence, the national prevalence rates were applied to the Indigenous population to produce Indigenous prevalence estimates of dermatitis & eczema and acne, for 2003, 2011 and 2018.
For psoriasis, Indigenous estimates were obtained using the AATSIHS 2018–19 for 2018 estimates, the AATSIHS 2012–13 for 2011 estimates and the NATSIHS 2004–05 for 2003 estimates.
Prevalence for skin infections for the Indigenous population in 2018, 2011 and 2003 were estimated using the NHMD and adjusted for Indigenous under-identification using adjustment factors (see Years lived with disability (YLD)).
For ulcers, hospitalisation rate ratios (Indigenous: national) based on Indigenous hospitalisations adjusted for under-identification using standard adjustment factors, were applied to the national prevalence rates.
To estimate the prevalence of other skin disorders in the Indigenous population, the same methods were used as for national estimates using the AATSIHS 2018–19, AATSIHS 2012–13 and NATSIHS 2004–05.
Indigenous prevalence for scabies were estimated by summing estimates from the NHMD adjusted for Indigenous under-identification using adjustment factors (see Years lived with disability (YLD)) and estimates based on Kearns et al. (2015) for Very Remote areas.
References
ACSQCH (Australian Commission on Safety and Quality in Health Care) 2018. Creating safer, better health care – The impact of the National Safety and Quality Health Service Standards. Sydney: ACSQHC, 50.
AIHW 2019. GEN data: People using aged care services, 30 June 2018. Canberra: AIHW.
AIHW 2020. GEN Aged Care Data – Residential Quality Indicators – July to September 2019. Canberra: AIHW.
Asimus M & Li P 2011. Pressure ulcers in home care settings: is it overlooked? Wound Practice and Research 19(2):88–97.
CEC (Clinical Excellence Commission) 2017. 2016 NSW Pressure Injury Point Prevalence Survey Report. Sydney: Clinical Excellence Commission.
CEC 2019. 2018 NSW Pressure Injury Point Prevalence Survey Report. Sydney: Clinical Excellence Commission.
Dealey C, Posnett J & Walker A 2012. The cost of pressure ulcers in the United Kingdom. Journal of Wound Care 21(6):261–6.
Ferguson C, Crouchley K, Mason L, Prentice J & Ling A 2019. Pressure injury point prevalence: state-wide survey to identify variability in Western Australian hospitals. The Australian Journal of Advanced Nursing 36(4):28.
Harrison C, Britt H, Miller G & Henderson J 2013. Prevalence of chronic conditions in Australia. PLoS ONE 8(7).
Kearns TM, Speare R, Cheng AC, McCarthy J, Carapetis JR, Holt DC et al. 2015. Impact of an ivermectin mass drug administration on scabies prevalence in a remote Australian Aboriginal community. PLoS Neglected Tropical Diseases 9(10):e0004151.
Kilkenny M, Merlin K, Plunkett A & Marks R 1998. The prevalence of common skin conditions in Australian school students: acne vulgaris. British Journal of Dermatology 139(5):840–5.
Marks R, Kilkenny M, Plunkett A & Merlin K 1999a. The prevalence of common skin conditions in Australian school students: atopic dermatitis. British Journal of Dermatology 140(3):468–73.
Marks R, Plunkett A, Merlin K & Jenner N 1999b. Atlas of common skin diseases in Australia. Melbourne: Department of Dermatology, St Vincent’s Hospital.
Mulligan S, Prentice J & Scott L 2011. WoundsWest Wound Prevalence Survey 2011: state‑wide overview report. Perth: Ambulatory Care Services, Western Australian Department of Health.
Plunkett A, Merlin K, Gill D, Zuo Y, Jolley D & Marks R 1999. The frequency of common non‑malignant skin conditions in adults in central Victoria, Australia. International Journal of Dermatology 38(12):901–8.
Puig L, van de Kerkhof PC, Reich K, Bachelez H, Barker J, Girolomoni G et al. 2017. A European subset analysis from the population‐based Multinational Assessment of Psoriasis and Psoriatic Arthritis shows country‐specific features: results from psoriasis patients in Spain. Journal of the European Academy of Dermatology and Venereology 31(7):1176–82.
Queensland Health 2019. Pressure Injury Prevention program overview. Queensland: Clinical Excellence Queensland.
SA Health (South Australian Department of Health) 2007. South Australian Pressure Ulcer Point Prevalence Survey report 2007: increasing validity and reliability of findings, category A1. Adelaide: SA Health
Santamaria N, Carville K, Prentice J, Ellis I, Ellis T, Lewin G et al. 2009. Reducing pressure ulcer prevalence in residential aged care: results from phase II of the PRIME trial. Wound Practice and Research: Journal of the Australian Wound Management Association 17(1):12–22.
VQC (Victorian Quality Council) 2006. Pressure Ulcer Point Prevalence Survey: statewide report 2006. Melbourne: Victorian Department of Human Services.