Unmet need
Figure 26: Whether Aboriginal and Torres Strait Islander people had an unmet need for dental care in the last 12 months, by selected categories and survey cycle
Bar chart shows that in 2022–23, 84% of Aboriginal and Torres Strait Islander people aged 2 and over in Very remote areas did not have an unmet for a dentist in the last 12 months, compared with 77% in Inner regional areas.
Notes:
- The percentage distribution is calculated only on those who had at least one occasion of unmet need in the last 12 months.
- Only reasons with an acceptable standard error were included.
- Respondents were allowed to select multiple responses.
- Data are population weighted estimates.
Source: AIHW analysis of 2022–23 NATSIHS using TableBuilder (ABS 2025).
In 2022–23, of the estimated 91,600 Aboriginal and Torres Strait Islander people aged 2 and over who had unmet need for dental care because of cost:
- 60,200 (66%) usually went to a mainstream GP
- 53,500 (58%) were female
- 50,900 (56%) had disability
- 39,900 (44%) lived in Major cities
- 39,400 (43%) were in the most disadvantaged areas (1st SEIFA quintile).
The reasons for unmet need for dental care differ from that for GPs with respect to the number and proportion who disliked the service/professional or were afraid or embarrassed – 23% of those aged 2 and over (or an estimated 45,600 of 202,000) compared with 8.4% (13,300 of 159,000) for GPs. Understanding this fear and embarrassment is essential to overcome barriers to dental care, even when it is available.
Looking at whether the reasons for unmet need for dental care differed by the usual source of health care (AMS/CC and mainstream GPs only) shows that cost was much less of a barrier for those using an AMS/CC (28% or an estimated 15,000 of 53,300) than for those using a mainstream GP (52% or 60,200 of 116,000), while waiting time being too long or the service not being available at the time required was much less of a barrier for those using a mainstream GP (16% or 18,500 of 116,000) than those using an AMS/CC (31% or 16,300 of 53,300) (Table 7).
Reason for unmet need | AMS/CC | Mainstream GP |
|---|---|---|
Cost | 28.1 | 52.1 |
Too busy (including work, personal, family responsibilities) | 24.2 | 23.9 |
Dislikes (service/professional, afraid, embarrassed) | 24.4 | 20.8 |
Waiting time too long or not available at time required | 30.6 | 16.0 |
Decided not to seek care | 9.9* | 11.2 |
Estimated total with unmet need | 53,300 | 116,000 |
* Estimate has a relative standard error between 25% and 50% and should be used with caution.
Note: Data are population weighted estimates.
Source: AIHW analysis of 2022–23 NATSIHS using TableBuilder (ABS 2025).
Comparisons across survey cycles
Cost has remained the primary reason for unmet need for dental care for Aboriginal and Torres Strait Islander aged 2 and over across the 3 survey cycles, ranging from 43% in 2012–13, to 42% in 2018–19, to 45% in 2022–23 (Figure 28). However, while there appear to have been some changes in these and other proportions across cycles, these differences may fall within the margin of sampling error and should be interpreted with caution.
Figure 28: Aboriginal and Torres Strait Islander people aged 2 and over, selected reasons had unmet need for dental care, by survey cycle
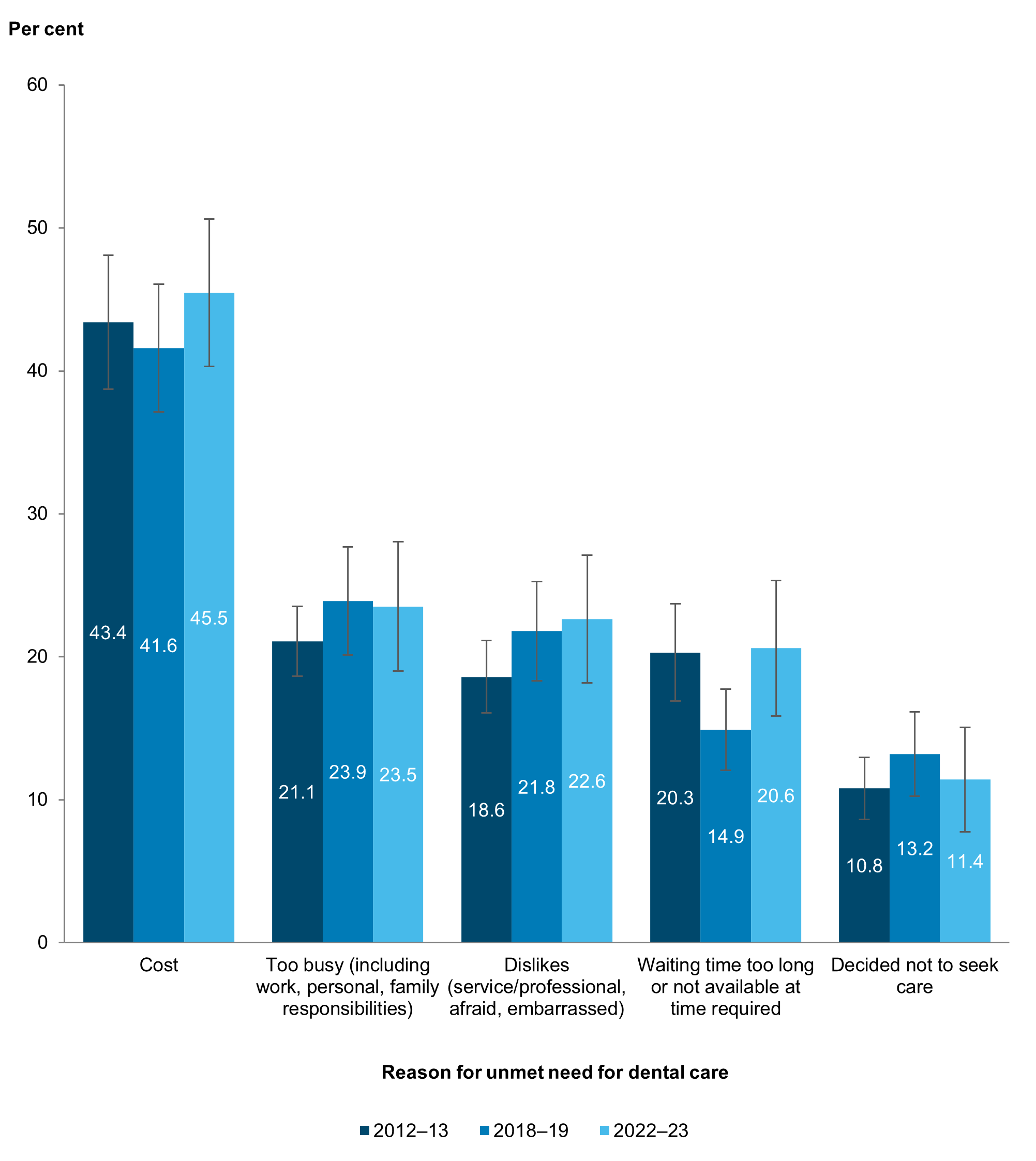
Notes:
- Data are population weighted estimates.
- While non-overlapping confidence intervals (CIs) generally indicate statistical significance, overlapping CIs do not necessarily imply that a difference is not significant. See Technical notes for more information.
Source: AIHW analysis of 2012–13, 2018–19 and 2022–23 NATSIHS using TableBuilder (ABS 2013, 2019, 2025).