Unmet need
Figure 20: Aboriginal and Torres Strait Islander people, unmet need for GP in the last 12 months, by selected categories and survey cycle
Bar chart shows that in 2022–23, 80% of Aboriginal and Torres Strait Islander people in Major cities had no unmet need for GP services in the last 12 months, compared with 93% in Very remote areas.
Notes:
- Percentage distribution is calculated only on those who had at least one occasion of unmet need in the last 12 months.
- Only reasons with an acceptable standard error were included.
- The full wording of the graph label ‘Dislikes’ is ‘Dislikes (service/professional, afraid, embarrassed)’. Respondents were allowed to select multiple responses.
- Data are population weighted estimates.
Source: AIHW analysis of 2022–23 NATSIHS using TableBuilder (ABS 2025a).
Comparisons across survey cycles
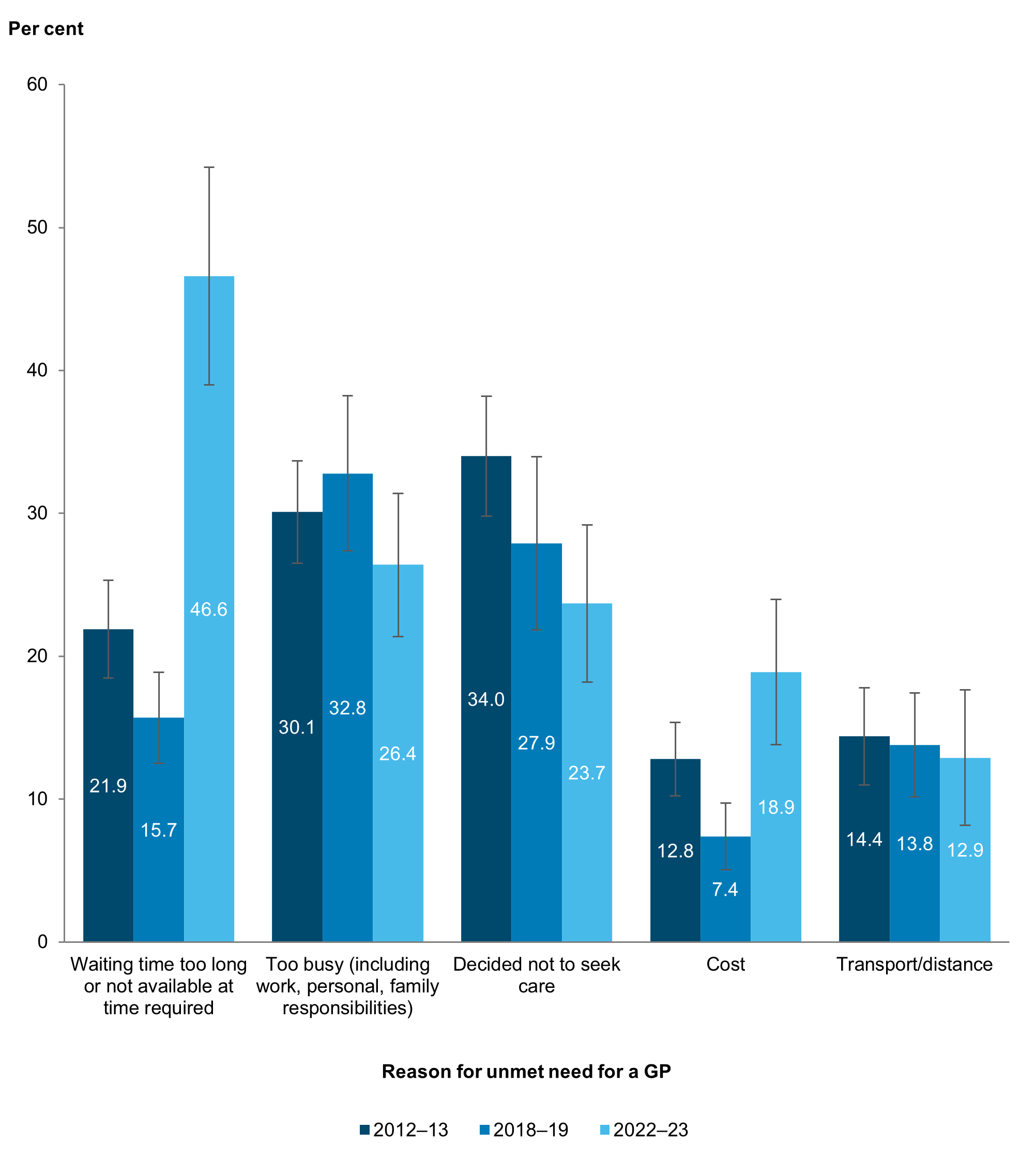
There have been changes across survey cycles in why Aboriginal and Torres Strait Islander people had unmet need for a GP. Long waiting times or the GP not being available at the time needed significantly decreased from 22% (or an estimated 19,200 of 87,700) in 2012–13, to 16% (16,000 of 102,000) in 2018–19, before a large and significant increase to 47% (74,100 of 159,000) in 2022–23 (Figure 22). There was a similar pattern for cost, with a significant decrease from 13% (or 11,200) in 2012–13, to 7% (7,500 of 102,000) in 2018–19, before a large and significant increase to 19% (30,000 of 159,000) in 2022–23.
Figure 22: Aboriginal and Torres Strait Islander people, selected reasons had unmet need for a GP in the last 12 months, by survey cycle
Notes:
- Data are population weighted estimates.
- While non-overlapping confidence intervals (CIs) generally indicate statistical significance, overlapping CIs do not necessarily imply that a difference is not significant. See Technical notes for more information.
Source: AIHW analysis of 2012–13, 2018–19) and 2022–23 NATSIHS using DataLab (ABS 2013b, 2019b, 2025b).