Data and methods
On this page In this section
Age Counting clients Counting treatment services Data collection process Drugs of concern Duration Population rates Reason for cessation Remoteness area Service sectors Source of referral: diversion Treatment Trends Imputation methodology for AOD clients Historical data element changesAge
Age is calculated as at the start of the episode.
Counting clients
Every client in the Alcohol and Other Drug Treatment Services National Minimum Data Set (AODTS NMDS) is assigned a statistical linkage key (SLK-581).
Client counts are based on the number of valid SLK-581s in the AODTS NMDS.
National client counts are based on the first time a client’s SLK-581 appears in the AODTS NMDS in the financial year. All clients are counted once in national totals irrespective of the number of times they receive treatment (distinct count).
Treatment and demographic characteristics of clients counted at the national level are based on the first treatment episode for the client within the financial year the data was collected.
State and territory client counts are based on counting the first occurrence of an SLK-581 in the AODTS NMDS in each jurisdiction in that financial year. Clients who receive treatment in more than one jurisdiction will therefore be counted in each of these jurisdictions (overlap count). This is most common among clients who reside close to interstate borders and travel interstate for treatment. For example, clients who reside in Queanbeyan, NSW and travel to Canberra, ACT for treatment. This means that the sum of clients at the state and territory level can be greater than the national total.
Treatment and demographic characteristics of clients are based on the first treatment episode for the client within the state/territory and within the financial year the data was collected.
This report uses both national and state and territory counts to describe trends at both national and jurisdictional levels, as well as movements between jurisdictions. For more information, refer to the supplementary table footnotes and the SLK-581 guide for use [PDF 96kB].
Counting treatment services
The Alcohol and Other Drug Treatment Services National Minimum Data Set (AODTS NMDS) contains information from publicly funded AOD treatment agencies and their service delivery outlets. An agency can have more than one service delivery outlet, located in different areas.
This is a service provision-based collection and not demand-based, noting that services are limited by the number of clients they are able to provide treatment to, and that this is not reflective of the demand for services by the broader community.
Data collection process
For most states and territories, the data provided for the national collection are a subset of a more detailed jurisdictional data set used for planning and policy. Figure A1 shows the processes involved in constructing the national data.
Figure A1: Alcohol and other drug treatment data collection flowchart
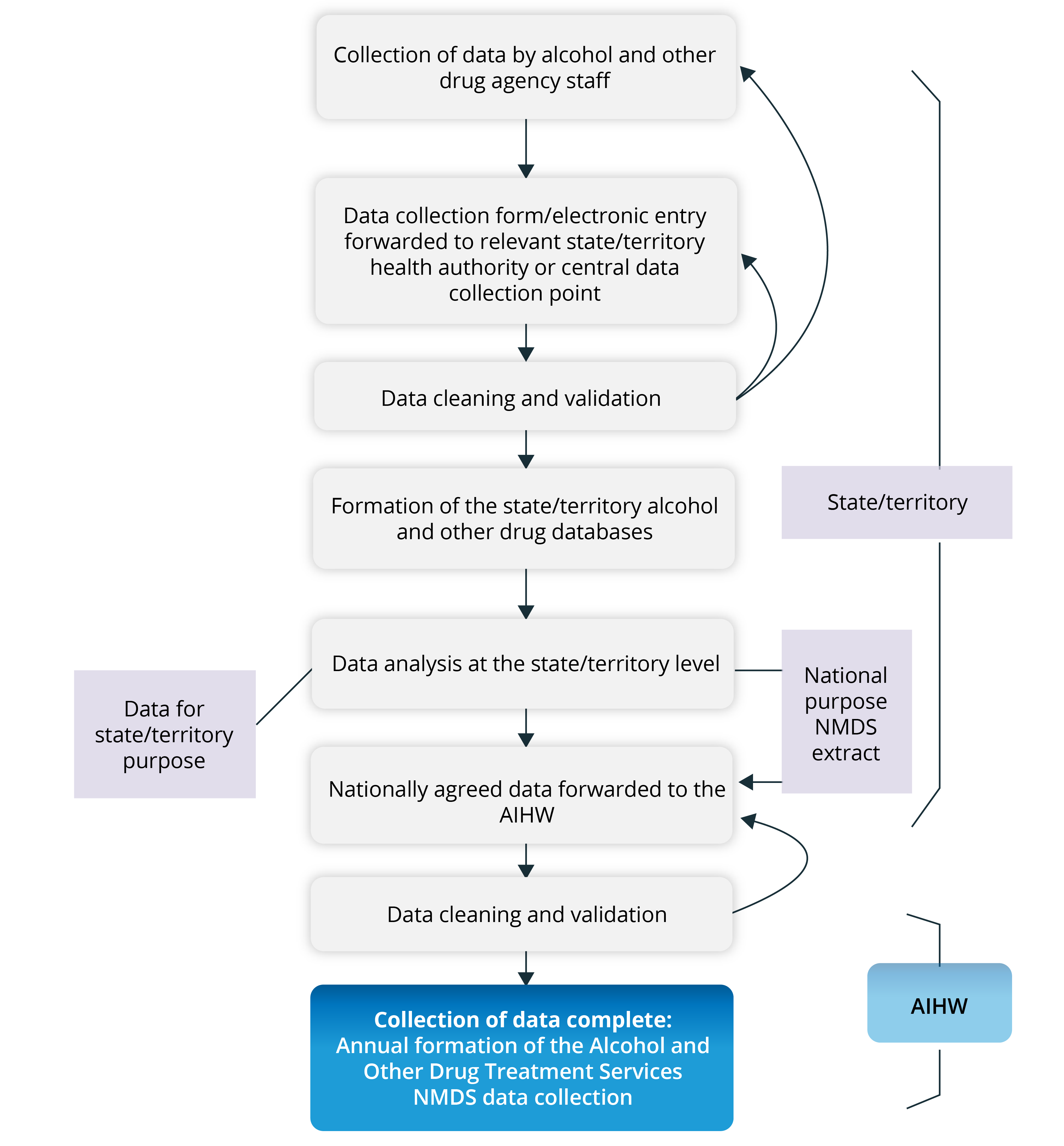
The flowchart depicts the collection process of the Alcohol and Other Drug Treatment National Minimum Data Set. The boxes show the steps involved to submit, clean and validate data at the state and territory level. First, starting with the collection of data by AOD agency staff, data collected via collection form/electronic entry is forwarded to the relevant state/territory health authority of the central data collection point. Data is cleaned, validated and used in the formation of the state/territory AOD databases. Data extracts from state/territories and from services solely funded under the Drug and Alcohol Program at the Department of Health, Disability and Ageing is forwarded to the AIHW. At the AIHW, the data is cleaned, validated and compiled into the national data set for use in the annual formation of the AODTS NMDS.
Drugs of concern
The Alcohol and Other Drug Treatment Services National Minimum Data Set (AODTS NMDS) contains data on drugs of concern that are coded using the ABS Australian Standard Classification of Drugs of Concern (ASCDC) (ABS 2011). In this report, these drugs are grouped (Table A1).
Group | ASCDC codes | Category | Includes |
|---|---|---|---|
Analgesics | 1000–1999 | Codeine | — |
Morphine | — | ||
Buprenorphine | — | ||
Heroin | — | ||
Methadone | — | ||
Other opioids | Oxycodone, fentanyl, pethidine | ||
Other analgesics | Paracetamol | ||
Sedatives and hypnotics | 2000–2999 | Alcohol | Ethanol, methanol and other alcohols |
Benzodiazepines | Clonazepam, diazepam and temazepam | ||
Other sedatives and hypnotics | Ketamine, nitrous oxide, barbiturates and kava | ||
Stimulants and hallucinogens | 3000–3999 | Amphetamines | Amphetamine, dexamphetamine and methamphetamine |
Ecstasy (MDMA) | — | ||
Cocaine | — | ||
Nicotine | — | ||
Other stimulants and hallucinogens | Volatile nitrates, ephedra alkaloids, phenethylamines, tryptamines and caffeine | ||
Cannabinoids | 7000–7199 | Cannabis | — |
Other | 4000–6999 9000–9999 | Other | Anabolic agents and selected hormones, antidepressants and antipsychotics, volatile solvents, diuretics and opioid antagonists |
Not stated | 0000–0002 | Not stated | — |
In this report, pharmaceutical drugs were grouped using 10 drug types, making up the pharmaceuticals group for the purposes of the analysis. These drugs correspond to the ASCDC codes and classifications (Table A2).
Drug category | ASCDC | ASCDC classification | Drug description |
|---|---|---|---|
Codeine | 1101 | Analgesics Organic opiate analgesics | Codeine |
Morphine | 1102 | Analgesics Organic opiate analgesics | Morphine |
Buprenorphine | 1201 | Analgesics Semisynthetic opioid analgesics | Buprenorphine |
Oxycodone | 1203 | Analgesics Semisynthetic opioid analgesics | Oxycodone |
Methadone | 1305 | Analgesics Synthetic opioid analgesics | Methadone |
Benzodiazepines | 2400–2499 | Sedatives and hypnotics Benzodiazepines | Benzodiazepines n.f.d., alprazolam, clonazepam, diazepam, flunitrazepam, lorazepam, nitrazepam, oxazepam, temazepam, benzodiazepines n.e.c. |
Steroids | 4000–4999 | Anabolic agents and selected hormones Anabolic androgenic steroids Beta2 agonists Peptide hormones, mimetics and analogues Other anabolic agents and selected hormones Not further defined | Anabolic agents and selected hormones n.f.d., anabolic androgenic steroids n.f.d., boldenone, dehydroepiandrosterone, fluoxymesterone, mesterolone, methandriol, methenolone, nandrolone, oxandrolone, stanozolol, testosterone, anabolic androgenic steroids n.e.c., beta2 agonists n.f.d., eformoterol, fenoterol, salbutamol, beta2 agonists n.e.c., peptide hormones, mimetics and analogues n.f.d., chorionic gonadotrophin, corticotrophin, erythropoietin, growth hormone, insulin, peptide hormones, mimetics and analogues n.e.c., other anabolic agents and selected hormones n.f.d., sulfonylurea hypoglycaemic agents, tamoxifen, thyroxine, other anabolic agents and selected hormones n.e.c. |
Other opioids | 1100, 1199, 1200, 1299, 1300–1304, 1306–1399 | Analgesics Organic opiate analgesics Semisynthetic opioid analgesics Synthetic opioid analgesics Not further defined | Organic opiate analgesics n.f.d., organic opiate analgesics n.e.c., semisynthetic opioid analgesics n.f.d., semisynthetic opioid analgesics n.e.c., synthetic opioid analgesics n.f.d., fentanyl, fentanyl analogues, levomethadyl acetate hydrochloride, meperidine analogues, pethidine, tramadol, synthetic opioid analgesics n.e.c. |
Other analgesics | 0005, 1000, 1400–1499 | Analgesics Non-opioid analgesics Not further defined | Analgesics n.f.d., non-opioid analgesics n.f.d., acetylsalicylic acid, paracetamol, ibuprofen, non-opioid analgesics n.e.c. |
Other sedatives and hypnotics | 2000, | Sedatives and hypnotics Anaesthetics Barbiturates Gamma-hydroxybutyrate (GHB) type drugs and analogues Other sedatives and hypnotics | Sedatives and hypnotics n.f.d., anaesthetics n.f.d., ketamine, nitrous oxide, phencyclidine, propofol, anaesthetics n.e.c., barbiturates n.f.d., amylobarbitone, methylphenobarbitone, phenobarbitone, barbiturates n.e.c., GHB-type drugs and analogues n.f.d., GHB, gamma-butyrolactone, 1,4-butanediol, GHB-type drugs and analogues n.e.c., other sedatives and hypnotics n.f.d., chlormethiazole, kava lactones, zopiclone, doxylamine, promethazine, zolpidem, other se |
n.f.d – not further defined; n.e.c – not elsewhere classified.
Jurisdictional notes regarding principal drug of concern:
- South Australia reports a high proportion of treatment episodes where amphetamines are the principal drug of concern due to the SA Police Drug Diversion Initiative (PDDI). In addition, adult cannabis offences are not included in the PDDI due to the SA Cannabis Expiation Notice legislation.
- Victoria reported a high number of miscellaneous episodes coded as ‘Other drugs’ due to service provider reporting practices and limitations with the reporting system. This system was replaced in 2019–20. In 2019–20 and 2020–21, Victoria continued to report high levels of miscellaneous episodes coded as ‘Other drugs’ or ‘Not stated’ as principal drugs of concern due to service provider reporting practices with the new data reporting system.
- In Queensland, the proportion of cannabis episodes reported as the principal drug of concern is a result of the Police Drug Diversion Program, Illicit Drugs Court Diversion Program and Drug and Alcohol Assessment Referral Program (DAAR) operating in the state.
- In the Australian Capital Territory, removal of criminal penalties for possession of small quantities of cannabis in the ACT at the end of January 2020 reduced the number of cannabis-related diversions recorded as treatment episodes to low levels (mainly under-18s). Data collection improvements at government-operated services resulted in fewer ‘not stated’ responses in the 2022–23 collection.
Drugs of concern supplementary tables
Data for drugs of concern published in the supplementary tables may differ from results published within other tables, due to different counting methodology. Tables have been footnoted where there is different counting methodology. For example, where the principal drug of concern is coded as fentanyl (1301) and other drug of concern is coded as tramadol (1307), these drugs are within the same drug grouping (synthetic opioid analgesics) and counted only once.
Methamphetamine coding
Over the last 10 years, treatment episodes for amphetamines and amphetamines not further defined have decreased as coding practices improved in reporting treatment for methamphetamine. The rise in reported episodes for methamphetamine is likely to be due to a combination of factors, including improvements in agency coding, treatment system updates and increases in funded treatment services.
Method of use of amphetamines as a principal drug of concern
A client’s usual method of administering their principal drug of concern may indicate the form of drug used, particularly for amphetamines. For example:
- Clients who report smoking or inhaling amphetamines are most likely to be using amphetamines in crystal form.
- Clients who report ingesting or snorting are most likely to be using a powder form.
- Clients who report injecting amphetamines may be using any form of amphetamines, as each form (base, crystal and powder) can be injected. However, recent data from the Illicit Drug Reporting System (an annual survey of people who inject drugs) indicate that crystal and powder are the most common forms used among people who inject methamphetamine (Sutherland et al. 2022).
Duration
Duration is calculated in whole days, and only for closed episodes.
Population rates
In this publication, crude rates were calculated using the ABS’s estimated resident population at the midpoint of the data range: that is, rates for 2024–25 data were calculated using the estimated resident population at 31 December 2024. Rates for previous years may differ to previously reported due to updated estimated resident population.
Rates may differ from previously published data based on revised Australian population estimates. Due to non-demographic changes in the 2021 Census-based Aboriginal and Torres Strait Islander population estimates, rates for 'Aboriginal and Torres Strait Islander (First Nations) people', rates are only available for 2016–17 onwards.
The COVID-19 pandemic and the resulting Australian Government closure of the international border from 20 March 2020, caused significant disruptions to the usual Australian population trends. This report uses Australian Estimated Resident Population (ERP) estimates that reflect these disruptions.
In the year July 2020 to June 2021, the overall population growth was much smaller than the years prior and in particular, there was a relatively large decline in the population of Victoria. ABS reporting indicates these were primarily due to net-negative international migration (National, state and territory population, June 2021).
Note that this change in the usual population trends may affect interpretation of statistics calculated from these ERPs. For example, rates and proportions may be greater than in previous years due to decreases in the denominator (population size) of some sub-populations.
Reason for cessation
The AODTS NMDS contains data on the reason an episode ended (reason for cessation). In this report, these reasons are grouped (Table A3), but data for the individual end reasons are available in the online supplementary tables.
A different method was used for grouping end reasons in reports released before 2014, so trend comparisons across reports should be made with caution. It is possible to compare data at the individual end reasons using the supplementary tables.
Outcome type | Reason for cessation |
|---|---|
Expected/planned completion | Treatment completed |
Ceased to participate at expiation | |
Ceased to participate by mutual agreement | |
Ended due to unplanned completion | Ceased to participate against advice |
Ceased to participate without notice | |
Ceased to participate due to non-compliance | |
Referred to another service/change in treatment mode | Change in main treatment type |
Change in delivery setting | |
Change in principal drug of concern | |
Transferred to another service provider | |
Other | Drug court or sanctioned by court diversion service |
Imprisoned (other than drug court sanctioned) | |
Died | |
Other | |
Not stated |
Remoteness area
This report uses the ABS’s Australian Statistical Geography Standard (ASGS) Edition 3 (ABS 2021) to analyse the proportion of AOD treatment agencies by remoteness area. This structure allows areas that share common characteristics of remoteness to be classified into broad geographic regions of Australia. These areas are:
- Major cities
- Remote
- Inner regional
- Very remote
- Outer regional
The remoteness structure divides each state and territory into several regions based on road distance to population centres of various sizes. This allows a proxy to be created for relative access to services.
Examples of urban centres in each remoteness area are:
- Major cities Canberra, Newcastle
- Inner regional Hobart, Bendigo
- Outer regional Cairns, Darwin
- Remote Katherine, Mount Isa
- Very remote Tennant Creek, Meekatharra.
For this report, the remoteness area of the agency was determined using the Statistical Area Level 2 (SA2) of the agency. Not all SA2 codes fit neatly within a single remoteness category, and a ratio is applied to reapportion each SA2 to the applicable remoteness categories. As a result, it is possible that the number of agencies in a particular remoteness category is not a whole number. After rounding, this can result in there being ‘<0.5%’ agencies in a remoteness area, due to the agency’s SA2 partially crossing into the remoteness area.
The Australian Statistical Geography Standard ASGS has replaced the Australian Standard Geographical Classification 2006 (ABS 2006), which was used in previous reports to calculate remoteness areas. Therefore, remoteness data for 2011–12 and previous years are not comparable with those for 2012–13 and subsequent years.
Service sectors
From 2008–09, agencies funded by the Department of Health under the Non-Government Organisation Treatment Grants Program (NGOTGP) were classified as non‑government agencies. Before this, many of these agencies were classified as government agencies. As a result, trends in service sectors of agencies should be interpreted with caution.
Source of referral: diversion
Throughout Australia, there are programs that divert people who have been apprehended or sentenced for a minor drugs offence from the criminal justice system. Many of these diversions result in clients receiving drug treatment services, who have been referred to treatment agencies as part of a drug diversion program. Since the 1980s, Australian governments have supported programs aimed at diverting from the criminal justice system people who have been apprehended or sentenced with a minor drugs offence.
In Australia, drug diversion program come in 2 main forms:
- Police diversion occurs when an offence is first detected by a law enforcement officer. It usually applies for minor use or possession offences, often relating to cannabis, and can involve the offender being cautioned, receiving a fine and/or having to attend education or assessment sessions.
- Court diversion occurs after a charge is laid. It usually applies for offences where criminal behaviour was related to drug use (for example, burglary or public order offence). Bail-based programs generally involve assessment and treatment, while pre‑ and post-sentence programs (including drug courts) tend to involve intensive treatment and are aimed at repeat offenders.
Treatment
The number of closed treatment episodes for counselling as a main treatment type has remained the most common treatment type for all clients over all collection years. Fluctuations over time in closed treatment episodes for particular treatment types may be influenced by coding practices, increased funding or changes in treatment policies or capacity to provide specialised alcohol and other drug treatment services, which may contribute to variation in treatment types over time.
Trends
Trend data may differ from data published in previous versions of Alcohol and other drug treatment services in Australia, due to data revisions.
Imputation methodology for AOD clients
A Statistical Linkage Key-581 (SLK) was introduced into the AODTS NMDS for the 2012–13 collection to enable the number of clients receiving treatment to be counted, while continuing to ensure the privacy of these individuals receiving treatment.
An imputation strategy for the collection was implemented in 2012–13, 2013–14 and 2015–16. It was developed to correct for the impact of invalid or missing SLKs on the total number of clients. This strategy took into account several factors relating to the number of episodes per client and makes assumptions relating to spread across agencies. It also took into consideration the likelihood that an episode with a missing SLK relates to a client that has already been counted through other episodes with a valid SLK.
To ensure an accurate representation of the AODTS client population, imputation was applied to the 2012–13, 2013–14 and 2015–16 AODTS NMDS to account for the proportion of valid SLKs being less than 95% for these years. The national rate of valid SLKs for these years was largely affected by low proportions of valid SLKs in New South Wales.
Further information about the imputation methodology applied to historical data can be found the report Alcohol and other drug treatment services in Australia 2015–16, Appendix B: Imputation methodology for AOD clients.
Historical data element changes
Details on historical data element changes are found in Appendix A of the AODTS NMDS Data Collection Manual 2024–25 [PDF 745kB].
ABS (Australian Bureau of Statistics) 2006. Statistical geography: volume 1—Australian Standard Geographical Classification (ASGC). ABS cat. no. 1216.0. Canberra: ABS.
ABS 2011. Australian Standard Classification of Drugs of Concern, 2011. ABS cat. no. 1248.0. Canberra: ABS.
ABS 2016. Estimates of Aboriginal and Torres Strait Islander Australians, July 2016. ABS cat. no.1270.0.55.005. Canberra: ABS.
ABS 2021. Australian Statistical Geography Standard Edition 3, ABS, Australian Government, accessed 29 February 2024.
Sutherland R, Uporova J, King C, Jones F, Karlsson A, Gibbs D, et al. 2022. Australian Drug Trends 2022: Key Findings from the National Illicit Drug Reporting System (IDRS) Interviews. Sydney: National Drug and Alcohol Research Centre, University of New South Wales, accessed 3 April 2023.