Summary
In June 2020, the Australian Sports Commission (ASC) commissioned the AIHW to investigate the benefits and costs to the health system associated with participation in sport and physical activity. This analysis is part of a broader project to develop methodology for gathering evidence around injuries arising from sport participation and the potential population benefits achieved through improved injury prevention and management and increased physical activity.
The purpose of this project is to quantify the health spending related to physical activity, including sport participation, within the Australian population. This is done by assessing:
- costs due to immediate and long term risk of injuries; and
- the avoided health spending due to better health status.
This report generally uses the term physical (in)activity, which includes sport, as well as other forms of exercise and bodily movements for leisure, transportation, and work.
The AIHW has previously published detailed estimates of the costs of physical activity related injuries in the Economics of sports injuries publication. These estimates are expanded in this report to include estimates of the long-term outcomes of injuries, relating to post-traumatic osteoarthritis. In 2018-19, it was estimated that $149 million of spending on osteoarthritis related to a prior injury that occurred while doing physical activity.
Preliminary estimates of the avoided health spending due to improved health status indicated a number of limitations to physical activity models used, due to the limited number of conditions included. This current report seeks to improve these initial estimates by incorporating associations of physical activity with a broader range of health conditions – both directly, and through intermediate risk factors (such as blood pressure). The additional disease estimates in this report include: depression, anxiety, falls, and the physical activity related proportion of diseases due to high blood pressure, high blood glucose, and low bone mineral density.
These estimates represent a first attempt to comprehensively quantify disease costs incurred due to physical inactivity and those potentially avoided through participation in physical activity through these additional conditions and intermediate risk factors.
Attributing disease burden and health costs to diseases is complex and generally not undertaken annually. The most recent year for which estimates of both disease burden due to risk factors and disease spending are available is 2018-19. Disease burden and risk factor estimates from the Australian Burden of Disease Study 2018 and the Disease expenditure in Australia 2018-19 report are the basis for inactivity costs and avoided spending estimates in this report.
Cost of disease due to physical inactivity
It is estimated that the cost to the health system of diseases caused by physical inactivity was $2.4 billion in 2018-19, with:
- $1.7 billion from the direct effects of physical inactivity, of which:
- $369 million was from coronary heart disease, $319 million from falls (due to poorer muscle tone and balance), and $302 million from depressive disorders
- $560 million due to high blood pressure caused by inactivity
- $125 million due to high blood plasma glucose caused by inactivity
- $81 million due to osteoporosis (low bone mineral density) caused by inactivity
Physical activity likely also reduces cholesterol, which is further linked to coronary heart disease and stroke. However, this association is currently unable to be included in the model due to inadequate data to sufficiently quantify the reduction in cholesterol according to activity level. Similarly, while physical activity can influence body mass index (BMI), this does not occur independently of the overall energy balance achieved through food consumption. This model therefore does not include physical activity reducing BMI, as this may overestimate the impact activity has on health and healthcare spending
Disease prevented through physical activity
In addition to estimating the cost of diseases due to physical inactivity, this report further quantifies the estimated disease spending prevented in 2018-19 due to diseases averted through physical activity undertaken over the year.
In 2018-19, physical activity prevented $1.7 billion of disease spending. The benefit was similar for males ($820 million) and females ($832 million). Around $190 million in benefit was due to reduced blood pressure and associated diseases, while $108 million was due to improved bone mineral density and reduced fracture costs.
Information on physical inactivity costs and activity related injuries and health benefits are presented by age, sex, condition, and treatment location. Data in this report is available to download as an Excel workbook.
This report complements several others by the AIHW:
- Sports injury hospitalisations in Australia, 2019–20
- National sports injury data strategy
- Australian Burden of Disease Study 2018: Interactive data on risk factor burden
- Reducing the burden due to overweight (including obesity) and physical inactivity.
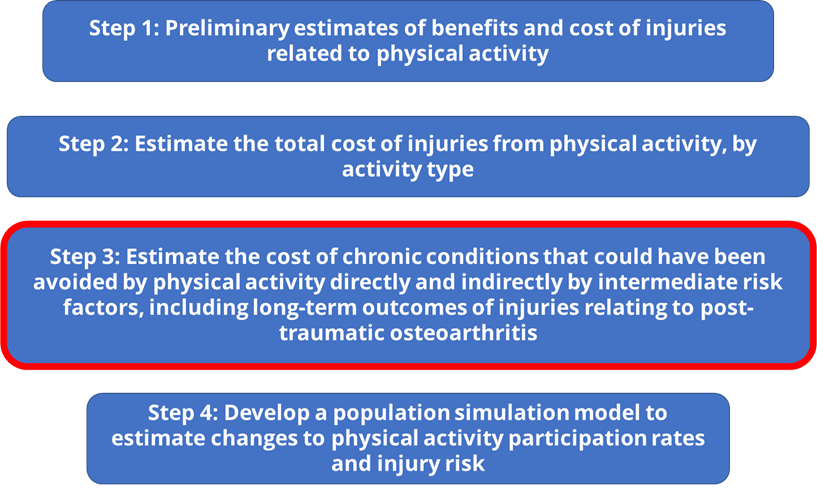
Work to estimate the benefits of sport and physical activity are ongoing, and this report is the third part of a series on methodology development of the economics of sports injury (Figure 1). The methods used in this report provide an average ‘snapshot’ in a year of the health effects of physical activity, and does not capture any dynamic effects on population health through changes to life expectancy, diagnosis of other conditions, or remission of disease. This will be incorporated into future reports through the development of a population simulation model, that will also include effects on the broader economy (such as productivity).
Figure 1: Overview of methodology development series.