Suicide & self-harm monitoring
Data sources
The NACS linked dataset includes:
- National Deaths Index (NDI)
- Alcohol and Other Drug Treatment Services National Minimum Data Set (AODTS-NMDS)
- Commonwealth funded health services (MBS and PBS)
- Specialist Homelessness Services Collection (SHSC).
For more information about the linkage process, and details of the dataset years included in the NACS, see the technical notes.
Data presentation
Throughout this article:
- values presented in the columns and rows of tables may not sum to the totals shown due to missing and not stated values, as well as rounding
- totals reported include missing and not stated values, unless otherwise noted
- the percentages shown in the tables are calculated excluding the missing and not stated values, unless indicated otherwise
- percentage distributions may not sum to 100 due to rounding
- the Australian Institute of Health and Welfare (AIHW) has strict confidentiality policies which have their basis in section 29 of the Australian Institute of Health and Welfare Act 1987 (AIHW Act) and the Privacy Act 1988 (Privacy Act). Data may be suppressed for either confidentiality reasons or where estimates are based on small numbers, resulting in low reliability. Information that results in attribute disclosure will also be suppressed.
Deaths data and statistics
Data for the number of deaths is sourced from the NACS linked dataset. Deaths in this report are presented by year of occurrence. In the version of the NDI database used in the NACS, data were considered final deaths registered prior to 2020, revised for deaths registered in 2020 and preliminary for deaths registered in 2021 and 2022.
The number of deaths in this report are not comparable to other AIHW publications, such as Deaths in Australia, due to:
- different data sources (National Death Index compared with the AIHW mortality database)
- year of death occurrence compared with year of death registration.
More information on deaths data and statistics for the NACS linked dataset are available in the NACS technical notes.
Specialist homelessness services
Client counts
The number of clients presented in this report will not necessarily match totals presented in other SHS reports. This is more marked for years prior to 2017–18, where SHSC data in other reports were imputed to account for agency non-response and invalid SLKs. Imputation was not required from 2018–19 due to the high rates of agency response and SLK validity. Imputation was not applied to the SHSC data for this project.
Homelessness status
Housing situation is derived at the support period level, using information about a client’s type of residential arrangement, their tenure and conditions of occupancy. Housing situation is available at 3 different time points for every support period within the NACS data:
- a week before they present to an SHS agency
- at presentation
- at the end of support.
Table 2 describes the different housing situations and how they are classified into experiences of homelessness within this report.
Housing situation | Experience of homelessness |
|---|---|
No shelter or improvised/ inadequate dwelling | Rough sleeping |
Short-term temporary accommodation | Other homeless |
House, townhouse or flat – couch surfer or with no tenure | Other homeless |
Other - homeless | Other homeless |
Public or community housing – renter or rent free | Not homeless |
Private or other housing – renter, rent free or owner | Not homeless |
Institutional settings | Not homeless |
Other – at risk | Not homeless |
Not stated | Not stated |
The housing situation of SHS clients described in this report uses all support periods that started, ended or were ongoing within a year using a cascading hierarchy, that is:
- rough sleeping includes any experience of rough sleeping in the year prior to suicide
- other homelessness includes any other experience of homelessness (except rough sleeping), including couch surfing and short-term or temporary accommodation
- not homeless includes housing situations limited to clients being at risk of homelessness
- not stated, all housing situation data was missing or unknown.
Sex
Sex is based on the sex reported to Medicare. If this was not available, the most frequently reported sex in the SHSC for a client was assigned – if there was not a dominant proportion, the client was based on the sex that was recorded for their most recent SHS activity. Sex was missing for some records – the sum of males and females may not add to the total.
The AIHW National Mortality Database (NMD) contains records for deaths in Australia from 1964 to 2023. The database comprises information about causes of death and other characteristics of the person, such as sex, age at death, area of usual residence and Indigenous status.
The AIHW sources causes of deaths data from the Registries of Births, Deaths and Marriages in each state and territory and the National Coronial Information System (NCIS). The cause of death data are compiled and coded by the Australian Bureau of Statistics (ABS) to the International Statistical Classification of Diseases and Related Health Problems (ICD) and maintained at the AIHW in the NMD. Registration of deaths is the responsibility of the Registry of Births, Deaths and Marriages in each state and territory.
To improve the quality of data, the ABS annually revises the causes of death for coroner-referred deaths to reflect the latest available information. This process applies to deaths registered after 1 January 2006. Deaths registered between 2006 and 2020 are finalised. Deaths registered in 2021 are revised, deaths registered in 2022 are preliminary revised, and 2023 registered deaths are preliminary. Revised, preliminary revised, and preliminary data are subject to further revision by the ABS. For a more detailed description of the coverage and processing of deaths data, including deaths certified by the coroner, refer to the ABS Causes of death, Australia, 2023 methodology, Australia (ABS 2024).
In the NMD, the year the death occurred, the year the death was registered with the state and territory registry, and the in scope year the death was lodged with the ABS (ABS reference year) are provided. Year of registration has been used for the purposes of monitoring deaths by suicide. Deaths based on the year the death occurred have also been presented; however, as some deaths at the end of each calendar year may not be registered until the following year, year of death information for the latest available year (2023) is generally an underestimate of the actual number of deaths that occurred in that year. While not as significantly impacted, it should be noted that latest data by year of registration is also an underestimate and subject to revision.
In more recent years, there have been occasions where the ABS has received a large number of deaths, which were registered in earlier years. For examples of where the ABS has received late registrations and the impact on mortality patterns, see Technical Note: Victorian additional registrations and time series adjustment and Technical Note: Victorian additional registrations (2013–2016).
Deaths (such as those from suicide) that are referred to a coroner can take time to be fully investigated, which can influence what information is available to assign a cause of death code during the ABS coding process. Each year, some coroner cases are coded by the ABS before the coronial proceedings are finalised. Coroner cases that have not been closed or had all information made available can impact on data quality as less specific ICD-10 codes often need to be applied. Published data include 2023 preliminary data, 2022 preliminary revised data and 2021 revised data. For more details of revisions to 2021 and 2022 data, refer to the Technical Notes in the 2022 issue of the Causes of Death Methodology. Data for reference years up to and including 2020 are considered final and no longer subject to the standard revisions process. Final data for 2021, revised data for 2022, and preliminary revised data for 2023 will be released in early 2025.
It is expected that deaths due to intentional self-harm will increase through the revisions process. For further information surrounding the revisions process, see 'Coding of suicide' in the 'Deaths due to intentional self-harm (suicide)' section of the ABS Causes of Death, Australia, 2023 methodology page.
The data quality statements underpinning the AIHW NMD can be found on the following ABS internet pages:
- ABS Quality declaration summary for Causes of death, Australia, 2023 methodology.
- ABS Quality declaration summary Deaths, Australia
For more information on the AIHW NMD see National Mortality Database and About National Mortality Database.
Quality of Indigenous status data
The Indigenous status of a deceased person is captured through the death registration process; however, it is recognised that not all such deaths are captured through these processes, leading to under-identification. The Aboriginal and Torres Strait Islander (First Nations) origin of a deceased person is noted on the Death Registration Form (DRF) and the Medical Certificate of Cause of Death (MCCD).
For 2022 for New South Wales, information from the MCCD has been used for the first time. Using both sources (the DRF and MCCD) resulted in a greater proportion of deaths of First Nations origin, compared to 2021. This change has introduced a break in time series in First Nations death statistics in New South Wales and Australia. Therefore, caution should be used when making comparisons with previous years. For more information on this change and the impacts refer to the Technical Note: The impact of using two sources for deriving the Indigenous status of deaths in NSW in 2022.
Data on deaths by suicide in First Nations people have been compiled by jurisdiction of usual residence for New South Wales, Victoria, Queensland, Western Australia, South Australia and the Northern Territory only. Data for Tasmania and the Australian Capital Territory have been excluded in line with national reporting guidelines.
The National Mortality Database (NMD) contains data on all deaths in Australia, including those by suicide. It includes individual level data on sex, age at death, area of usual residence, and First Nation status as well as causes of death. Data are sourced from Registries of Births, Deaths and Marriages in each state and territory and the National Coronial Information System (managed by the Victorian Department of Justice).
The NMD is compiled and coded by the Australian Bureau of Statistics (ABS) to the International Statistical Classification of Diseases and Related Health Problems (ICD) and maintained at the AIHW in the NMD. For more information on the NMD, see NMD technical notes section, above.
The ICD is a coding framework published by the World Health Organization and is used to compare mortality and morbidity statistics internationally. Chapters 5 and 21 were used to analyse the data on the NMD. Chapter 5 of the ICD-10, Mental and Behavioural Disorders is a list of codes for all diagnosable mental and behavioural disorders, including acute toxicities (codes F00-99) and are sometimes known as ‘F-codes’. Chapter 21 of the ICD-10, Factors Influencing Health Status and Contact with Health Services, includes ‘psychosocial risk factors’ for mortality and morbidity (codes Z00 – Z99). These codes are used to identify factors which might have influenced a person’s health as well as affected their ability to contact health services. For more information on how deaths are coded by the ABS, please see the ABS Causes of Death methodology.
As part of the National Suicide and Self-harm Monitoring Project, the AIHW commissioned the ABS to code psychosocial risk factors (‘Z-codes’) among cases of suicide. Data coding began in 2017 and is available for all deaths by suicide since 2017.
For the analysis Suicide among people with legal system contact and associated risk factors: Data from the National Mortality Database, specific Z-codes were used to flag in the NMD whether a person who died by suicide had contact with the legal system. Table 1 provides an overview of the included codes and their inclusion and exclusion criteria from the ABS.
| ICD-10 Z-code | ABS inclusion/exclusion criteria |
|---|---|
Z65.0 ‘Conviction in civil and criminal proceedings without imprisonment’ | Includes:
Excludes:
|
Z65.1 ‘Imprisonment and other incarceration’ | Includes:
|
Z65.2 ‘Problems related to release from prison’ | Includes:
|
Z65.3 ‘Problems related to other legal circumstances’ | Includes:
|
Source: ABS (2019) ‘Psychosocial risk factors as they relate to coroner-referred deaths in Australia’
If a case has any one of above the listed codes, it was flagged as ‘had contact with the legal system’. Codes were applied to all deaths by suicide between 2017 and 2022. Due to the small numbers, data was aggregated across all available years.
Table 2 defines how mental and behavioural disorders were identified in the NMD:
| Mental and behavioural disorder | Definitions and underlying codes |
|---|---|
Mood [affective] disorders | Mood [affective] disorders (F30-9). |
Anxiety disorders (includes neurotic, stress, and somatoform disorders) | Neurotic, stress-related and somatoform disorders (F40.0-8). |
Alcohol disorders | Mental and behavioural disorders due to use of alcohol (F10.0-9). |
Other substance disorders | Includes mental and behavioural disorders due to use of: sedatives or hypnotics, cocaine, hallucinogens, tobacco, volatile solvents, and multiple drug use and use of other psychoactive substances (F13.0-14.9, F16.0-19.9). |
Other mental and behavioural disorders | Includes Behavioural syndromes associated with physiological disturbances and physical factors, mental retardation, disorders of psychological development, behavioural and emotional disorders with onset usually in childhood and adolescence and unspecified mental disorders (F50.0-9, F45.4, F70-99). |
Stimulant disorders | Mental and behavioural disorders due to use of other stimulants, including caffeine (F15.0-9). |
Personality disorders | Disorders of adult personality and behaviour (F60-9). |
Opioid disorders | Mental and behavioural disorders due to use of opioids (F11.0-9). |
Schizophrenia, schizotypal, and delusional disorders | Schizophrenia, schizotypal, and delusional disorders (F20-29). |
Cannabinoid disorders | Mental and behavioural disorders due to use of cannabinoids (F12.0-9). |
Organic disorders | Organic, including symptomatic, mental disorders (F00-09). Includes dementia and Alzheimer’s disease. |
Limitations of using NMD data to identify legal system contact, psychosocial risk factors and mental and behavioural disorders
Data collection varies by each state and territory and between individual cases. There may have been cases where the person had contact with the legal system or experienced other psychosocial risk factors and mental and behavioural disorders, but it was not noted in their coronial file and therefore not counted and compiled by the ABS.
Furthermore, psychosocial risk factors and mental and behavioural disorders can be either constant or temporary. An example of a constant psychosocial risk factor is something which cannot be changed, like a personal history of self-harm or the death of a family member. Temporary psychosocial risk factors are those which can change or resolve over time, some examples might include unemployment or problems within the social group, such as family or friends. An experience of one or more psychosocial risk factors or mental and behavioural disorders does not mean a person will die by suicide.
Depending on the type of mental and behavioural disorder, some may also be treatable and resolve over time. Mental and behavioural disorders relating to alcohol and substance use included ‘acute intoxication’ which, if not fatal, can resolve over time. A permanent mental or behavioural disorder is one which may or may not be treated but does not resolve over time.
Caution must be taken when interpreting some of the data. Many of the proportions are based on small numbers, sometimes fewer than 10. Where amalgamated data were less than 5 they are shown as ‘not presented’ (‘n.p.’). Consequential suppressions were applied if other groups could be used in conjunction with totals to calculate the suppressed numbers. Consequential suppressions are also shown as ‘n.p.’
Codes from the ICD-10 may not be culturally sensitive to the lives and experiences of First Nations people (AIHW 2022). Therefore, care must be taken when interpreting and comparing data among First Nations and non-Indigenous Australians.
Finally, the ABS does not code for perpetration or victimisation. For example, a case which included mention of a domestic and family violence order will be counted under ‘Problems related to other legal circumstances’ regardless of whether the person received (or was subject to) the order or was the person who applied for it.
This analysis compliments the National Deaths in Custody Program and the National Prisoner Health Data Collection by including people who may not have been in custody but who nonetheless had contact with the legal system. People who died by suicide and who had contact with the legal system were not necessarily imprisoned but may have had an upcoming proceeding or experienced other legal processes such as Domestic Violence Orders and restraining orders. This analysis adds another dimension to our overall understanding of the link between contact with the legal system in Australia and deaths by suicide.
It should be noted that due to the differences in data collection there are some discrepancies between the numbers of people who died in prisons between the NMD and the National Deaths in Custody Project (NDICP). In the NMD, numbers of people who were coded to as having had “imprisonment and other incarceration” mentioned in the case also included ‘impending imprisonment’ which may have affected these numbers. The criteria for a death in custody on the NDICP is slightly different, it does not include impending incarceration and includes police custody (see NDICP report).
References
ABS (Australian Bureau of Statistics) (2019) Annex listing: Psychosocial codes (inclusions and exclusions), ABS, Australian Government, accessed 24 January 2024.
ABS (Australian Bureau of Statistics) (2019) Psychosocial risk Factors as they relate to coroner-referred deaths in Australia, ABS, Australian Government, accessed 8 August 2024.
ABS (Australian Bureau of Statistics) (2023) Causes of Death, Australia Methodology. ABS, Australian Government, accessed 29 January 2024.
AIHW (Australian Institute of Health and Welfare) (2022a) Protective and risk factors for suicide among Indigenous Australians, Australian Government, accessed 10 April 2024.
McAlister M, Bricknell S (2023) AIC Statistical Report 41: Deaths in custody in Australia 2022–23 , AIC, Australian Government, accessed 10 April 2024.
WHO (World Health Organization) 2019, The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification, 11th Edition.
The primary data source for this analysis was the AIHW National Mortality Database (NMD), which holds records for deaths in Australia from 1964.
An age-period-cohort analysis was undertaken, and descriptive results visualised. Within an age-period-cohort analysis, age effects are due to biological and social ageing processes. Period effects are due to events that occur at a particular calendar time and impact all individuals, regardless of age. Finally, cohort effects arise from unique experiences shared by a group of people that remains impactful across the lifespan.
Data sources
National Mortality Database
The National Mortality Database (NMD) data analysed was preliminary revised for 2022, revised for 2021 and finalised for 2006 to 2020 registered data. Deaths registered between 1964 and 2005 were not subject to a revisions process. Data are presented by year of death occurrence and approximate year of birth. Data are not presented by Year of death registration. More information about the registrations and revisions processes for the causes of deaths data is provided within the Australian Bureau of Statistics Causes of Death, Australian methodology publication.
The following ICD codes were used to identify suicide deaths and methods within the causes of deaths data:
Methods of suicide death | ICD version and years | ICD codes |
|---|---|---|
All suicide deaths |
| |
| ICD-7 1958–1967 | E970–E979, E963 |
| ICD-8 1968–1978 | E950–E959 |
| ICD-9 1979–1996 | E950–E959 |
| ICD-10 1997–present | X60–X84, Y87.0 |
Suicide deaths by firearms |
|
|
| ICD-7 1958–1967 | E976 |
| ICD-8 1968–1978 | E955 |
| ICD-9 1979–1996 | E955 |
| ICD-10 1997–present | X72–X75 |
Suicide deaths by gas |
|
|
| ICD-7 1958–1967 | E972, E973 |
| ICD-8 1968–1978 | E951, E952 |
| ICD-9 1979–1996 | E951, E952 |
| ICD-10 1997–present | X67 |
Suicide deaths by hanging |
|
|
| ICD-7 1958–1967 | E974 |
| ICD-8 1968–1978 | E953 |
| ICD-9 1979–1996 | E953 |
| ICD-10 1997–present | X70 |
Suicide deaths by poisoning (except gas) |
|
|
| ICD-7 1958–1967 | E970, E971 |
| ICD-8 1968–1978 | E950 |
| ICD-9 1979–1996 | E950 |
| ICD-10 1997–present | X60–X66, X68–X69 |
Estimate Resident Populations and Census Counts
Estimate Resident Populations (ERPs) at June 30 were used to estimate the population at risk of suicide and generate rates. ERPs at June 30 are available by sex and single year age groups for the calendar years 1971 to 2022. For calendar years 1964 to 1970 ERPs are only available by sex and 5-year age group. ERPs by single year age groups were estimated for 1964 through to 1970 using single year age group data from the 1966 Census and 1971 ERPs. AS such, the percentage distribution of single year age groups within each 5-year age group was calculated for the 1966 Census counts and 1971 ERPs. These 1966 Census count distributions were then applied to the 1964 through 1968 ERPs. The 1971 ERP distributions were applied to the 1969 and 1970 ERPs. More information about Estimate Resident Populations is provided within the ABS National, state and territory population methodology publication.
Dataset construction and smoothing
Data for suicide deaths were extracted from the NMD with the following details included: year of death, method of death, and age at death (in whole years). Consistent with Spittal et al. (2024), approximate year of birth was estimated by subtracting age at death from year of death (Cohort = Period – Age). ERPs were then matched to suicide death counts using year of death, single year of age at death, and sex. ERP matching was done separately for each method of death.
Three separate datasets were then generated and visualised. The age at death and approximate decade of birth dataset was generated by summing deaths and ERPs by single year age at death, sex, method, and decade of birth. The year of death and age group dataset was generated by summing deaths and ERPs by single year of death, sex, method and 10-year age groups. Lastly, the approximate year of birth and age group dataset was generated by summing deaths and ERPs by single year of approximate birth, sex, method and 10-year age group.
Moving average smoothing was applied to death and population counts within each of the three datasets. The rolling average was calculated using three lagged observations, the current observation, and three lead observations. Smoothed crude rates of death were then generated per 100,000 population. Due to data custodian requirements, only smooth data have been visualised and supplied in data tables. Exact Binomial (Clopper–Pearson) 95% confidence intervals were calculated for smoothed crude rates.
Data for patients who were hospitalised with intentional self-harm injuries are sourced from the AIHW’s National Hospital Morbidity Database (NHMD). Most of the data used for the monitoring of hospitalisations for intentional self-harm are from 2008–09 to 2022–23. For each reference year, the NHMD includes all hospitalisations for patients who were discharged between 1 July and 30 June.
The NHMD is a compilation of episode-level records from admitted patient morbidity data collection systems in Australian hospitals. It has records for all separations of admitted patient care from essentially all public and private hospitals in Australia.
The data supplied are based on the National Minimum Data Set (NMDS) for Admitted Patient Care and include administrative, demographic, and length of stay data, as well as data on the diagnoses of the patients, the procedures they underwent in hospital and external causes of injury and poisoning.
The purpose of the NMDS for Admitted Patient Care is to collect information about care provided to admitted patients in Australian hospitals. The scope of the NMDS is episodes of care for admitted patients in all public and private acute and psychiatric hospitals, free standing day hospital facilities, and alcohol and drug treatment centres in Australia. Hospitals operated by the Australian Defence Force, corrections authorities and in Australia’s off-shore territories are not in scope but may be included.
episode of care: The period of admitted patient care between a formal or statistical admission and a formal or statistical separation, characterised by only one care type (see care type and separation). METEOR identifier: 268956.
separation: The process by which an episode of care for an admitted patient ceases. A separation may be formal or statistical. METEOR identifier: 327268.
formal separation: The administrative process by which a hospital records the cessation of treatment and/or care and/or accommodation of a patient.
statistical separation: The administrative process by which a hospital records the cessation of an episode of care for a patient within the one hospital stay.
The criteria used to describe intentional self-harm hospitalisations reported in Suicide and self-harm monitoring is described in Codes and classifications.
Data limitations
States and territories are primarily responsible for the quality of the data they provide. However, the AIHW undertakes extensive validations on receipt of data, checking for valid values, logical consistency and historical consistency. Where possible, data in individual data sets are checked with data from other data sets. Potential errors are queried with jurisdictions, and corrections and resubmissions may be made in response to these queries. Except as noted, the AIHW does not adjust data to account for possible data errors or missing or incorrect values.
The most recent Data quality statement for Admitted Patient Care is available in METeOR. The Data Quality Statement contains information on other changes that may affect interpretation of the data for the relevant year. Please also see technical appendices for more information.
Quality of Indigenous status data
In 2011–12, an estimated 88% of Indigenous patients were correctly identified in public hospitals (AIHW 2013). The overall quality of the data provided for Indigenous status needs some improvement and varied between states and territories. It is unknown to what extent Indigenous Australians might be under-identified in private hospital admissions data. See Admitted patient care 2022–23 [PDF 580KB] for information supplied by the states and territories to provide some additional insight into the quality of Indigenous status data in the NHMD.
The National Ambulance Surveillance System (NASS) is a public health monitoring system, which aims to provide timely and comprehensive data on intentional self-harm (including suicidal behaviours with self-injurious intent), mental health, and alcohol and drug harms in the community. Data for the NASS are compiled by Turning Point in partnership with Monash University and are sourced from paramedic electronic patient care records provided by Australian state and territory-based ambulance services. As part of the National Suicide and Self-harm Monitoring Project, the AIHW has contracted Turning Point through Monash University to develop and maintain the NASS for self-harm related ambulance attendances. Self-harm (suicide, suicidal ideation, suicide attempt, and self-injury) related modules from the NASS are reported here.
Information is obtained and coded through manual scrutiny of de-identified electronic patient care records (ePCRs), including paramedic clinical assessment, patient self-report, information from third parties and other evidence at the scene, such as written statements of intent (including social media, text messages and written notes), as recorded by paramedics. Intent of self-harm behaviours derived from the ePCR may be from either stated or physical evidence, or where there is evidence, but the patient may have denied the behavioural intent (Lubman et al. 2020).
Self-harm related ambulance attendances are included if self-harm occurred in the preceding (past 24 hours) or during the ambulance attendance, with 4 categories of self-harm related ambulance attendances defined and coded as:
- self-injury (non-fatal intentional injury without suicidal intent)
- suicidal ideation (thinking about killing oneself without acting on the thoughts)
- suicide attempt (non-fatal intentional injury with suicidal intent, regardless of likelihood of lethality)
- suicide (fatal intentional injury with suicidal intent).
Suicide, suicide attempt and suicidal ideation are considered mutually exclusive; however, self-injury could be simultaneously coded with any other self-harm case category.
The number of attendances related to suicide is under-represented as ambulances do not attend all deaths. Furthermore, when they do attend there may be insufficient information to determine suicidal intent at the scene.
Methods of suicide, suicide attempt or suicidal ideation are coded as are methods of self-injury and categories of suicidal ideation preparation (planned, unplanned and unknown if planned) using a modified ICD-10 coding framework.
For more information see Lubman et al.2020.
Data limitations
Data are collected for operational rather than monitoring or research purposes with paramedics only recording information that they either observe or is provided to them by the patient or bystanders, and which they deem clinically relevant to patient care. It is possible that relevant information with respect to self-harm or mental health variables is not recorded, or similar events may not be recorded consistently by different paramedics over time.
External factors also need to be considered which may impact the interpretation of the data. When interpreting ambulance attendance rates across states and territories, several factors can influence differences. For instance, the number of ambulance services available may vary by state and territory. Some states offer free ambulance services to their residents, while others are covered by private health insurance or out-of-pocket costs or are only free to vulnerable populations (ACT Emergency Services Agency n.d.; NSW Ambulance n.d.; Queensland Government 2020; Tasmanian Government Department of Health 2021 & Victorian Government Department of Health 2022). Access to 24-hour health centres is also not the same in all jurisdictions. For example, access to these services may be lower in states and territories with higher regional and remote populations, and greater geographical spread, such as Queensland (Lubman et al. 2020). Furthermore, paramedics record information that is relevant to patient care, and not for research purposes and, therefore, patient records may be inconsistent between jurisdictions, although the coding of these records by Turning Point provides a degree of consistency in the data obtained (Lubman et al. 2020). Factors such as these are not measurable in the data and the extent to which they influence the differences in rates of ambulance attendances between states and territories is unknown.
Technical issues outside of the control of Turning Point may impact ambulance attendance data such as industrial action, information technology issues and transportation of data. Every attempt, if possible, is made to fully retrieve lost data. Specific issues that have occurred are listed below:
- Data unavailable for NSW for June 2021.
- Industrial action occurred in NSW in April 2022, with a minimal impact on ambulance services and demand.
- A small decrease in the number of NSW ambulance attendances was observed in July and August 2022 due to technical issues.
- Industrial action in NSW during late January to early February 2023, which could result in lower numbers.
- A computer-aided dispatch outage in Qld on 10 March 2023 resulted in no cases being recorded for that date.
References
ACT Emergency Services Agency (n.d.) Fees and charges, ACT Emergency Services Agency website, accessed 25 May 2023.
Lubman DI, Heilbronn C, Ogeil RP, Killian JJ, Matthews S, Smith K, Bosley E, Carney RMcLaughlin K, Wilson A, Eastham M, Shipp C, Witt K, Lloyd B, and Scott D (2020) ‘National ambulance surveillance system: A novel method using coded Australian ambulance clinical records to monitor self-harm and mental health-related morbidity’. PLoS ONE, 15:e0236344, doi:org/10.1371/journal.pone.0236344.
NSW Ambulance (n.d.) Accounts & Fees, NSW Ambulance website, accessed 25 May 2023.
Queensland Government (2020) Interstate Ambulance Treatment and Transport Information for Queensland Residents, Queensland Government website, accessed 25 May 2023.
Tasmanian Government Department of Health (2021) Ambulance costs, Tasmanian Government Department of Health website, accessed 25 May 2023.
Victorian Government Department of Health (2022) Ambulance fees Victorian Government Department of Health website, accessed 25 May 2023.
The Multi-Agency Data Integration Project (MADIP) is a partnership among Australian Government agencies to develop a secure and enduring approach for combining information on healthcare, education, government payments, personal income tax, and demographics (including the Census) to create a comprehensive picture of Australian populations over time (ABS 2018). The key MADIP datasets used in analysis published on the Suicide and Self-Harm Monitoring site were:
- Person Linkage Spine (Australian Bureau of Statistics)
- 2011 Census of Housing and Population (Australian Bureau of Statistics)
- Causes of Death (Australian Bureau of Statistics)
- Personal Income Tax (Australian Taxation Office)
- Social Security and Related Information (Department of Social Services)
- Synthetic income data developed by the Australian National University using personal income tax data, social security payment information and Census (for more information see Biddle & Marasinghe 2021).
Linkage approach
In order to identify socioeconomic factors associated with deaths by suicide in Australia, 2011 Census and 2011 to 2017 Causes of Death data were linked to the ABS Person Linkage Spine (Spine). The Spine is comprised of all persons in the Medicare Enrolments Database, Personal Income Tax or Social Security and Related Information data sets at any point between 2006 and 2016 (ABS 2019). As the baseline population, 2011 Census was considered a closed population and several assumptions were made about this population. These include:
- everyone in the 2011 Census who did not die over the period were still in the population up to the end of 2017, that is, no migration occurred
- person information in the 2011 Census were held constant over the analysis period. However, in the modelling analysis conducted, time varying age and income of the year before suicide were calculated and applied.
Table 1 shows the linkage coverage of Census 2011 and deaths by suicide from the ABS Causes of Death. The Estimated Residential Population of Australia at 30 September 2011 was 22.43 million people (ABS 2021). Of these, 20,739,159 were accounted for in the Census 2011, noting that the Census 2011 started in August 2011. In total, the linked Census 2011 population was 16,700,062 (74.4% of the total Australian population of September 2011). According to the National Deaths Index, there are 17,306 deaths by suicide from September 2011 to December 2017, of which 11,580 (67%) deaths by suicide were linked to the linkable Census 2011 data. Suicide was defined by ICD-10 external cause codes X60–X84 and Y87.0
Total (n) | Linked (n) | Linked (%) | |
|---|---|---|---|
ERP(a) at Sept 2011 | 22,432,771 | 16,700,062 | 74 |
Deaths by suicide(b) | 17,306 | 11,580 | 67 |
- Estimated resident population. Linked records are from 2011 Census population.
- Linked deaths by suicide weighted to all deaths by suicide from September 2011 to December 2017.
Estimated suicide risk by educational attainment and employment method
Imputing weights for unlinked suicide deaths and 2011 Census
To address the issue of unlinked deaths by suicide and 2011 Census records, an imputation weighting technique was used. This section describes the method used to develop these weights, which involved a three-staged approach.
First stage: imputing weights to scale up the Census population. The ABS historical ERP for 31 December 2011 by states, sex and 5-year age groups were used to derive weights by these demographic characteristics, based on the assumption that there were no significant differences in the age distribution of the population. The derived weight was applied at the person level for each record of Census that has ABS Person Linkage Spine (Spine) information to enable analysts to weight the analyses to the 31 December 2011 total ERP.
Unlike the original ABS research paper (ABS 2016) describing the creation of a linked data set between 2011 Census and deaths registered in the following 13 months, the imputation method did not calculate weights by Indigenous and non-Indigenous populations. Also, note that Diplomatic personnel resident in Australia have not been excluded from total ERP.
Second stage: suicide weights were calculated by using all deaths by suicide from 2011 to 2017 by states and territories, sex and 5-year age groups. Suicide weights were then applied at person level to only those linked Census records with suicide information. This made it possible to weight the analyses to all deaths by suicide (18,848) from 2011–2017.
An issue with applying suicide weights is that suicide weights are slightly higher when compared with population weights applied in the first stage. As such, the combined weights of the linked records with both 2011 Census and suicide information when aggregated, the weighted ERP will be slightly higher than that of 31 December 2011. Hence the need for a scale down adjustment factor.
Third stage: Finally, a scale down adjustment factor, derived based on total ERP, linked deaths by suicide and all deaths by suicide, was applied at the person level to only Census records without linked death by suicide information. Hence the weights of the Census population with or without linked death by suicide information, aggregated to the 31 December 2011 ERP (22,340,025).
Cumulative suicide incidence
Australian residents in the 2011 Census, weighted to 31 December 2011 estimated resident population (ERP) and linked to ABS Causes of Death data from 2011 to 2017 created a binary outcome of either died by suicide (ICD 10 external cause codes X60–X84, Y87.0) or not. Note that deaths by suicide used in this analysis are based on year of occurrence. These may differ from deaths by suicide data used in other AIHW publications which are based on year of registration. In addition to the closed population assumptions noted above, due to data quality issues the age in this analysis is at the time of the 2011 Census except for those who have died by suicide.
Over the period 2011 to 2017, Australia recorded more than 18,800 deaths by suicide of people who were in the 2011 Census. This resulted in a cumulative incidence of about 84 per 100,000 people during the 7-year period. The cumulative number and incidence of deaths by suicide that occurred over the 7 years varies considerably by sex, educational attainment and labour force status.
Uncertainty in the estimates
All data are subject to some level of uncertainty. For the data presented in this analysis the sources of uncertainty include:
Linkage error: Uncertainty is introduced when there is error in linking data sets. The data used in this report carries some risk of linkage error. An attempt has been made to reduce this error through imputation weighting process but some uncertainty remains.
Timeliness of data: Some of the data used in this analysis is Census data collected in August 2011. A person’s education status and employment status can change over time, particularly for certain population groups. The use of out-of-date information introduces a source of error to the analysis.
Randomness in the number of deaths by suicide that occur in a given time period, 2011–2017: The number of deaths by suicide that occur in a given time period fluctuate, even if the underlying population risk remains the same. The exact distribution of the counts is unknown. With deaths by suicide being a rare event it is often assumed that the counts follow a Poisson distribution. If this is the case then the relative level of uncertainty due to randomness decreases as the number of deaths by suicide increase.
Regression risk models for selected census variables
The MADIP datasets used in this modelling are outlined in the Data section of these Technical notes. In this analysis, only people aged 25 to 64 years in the linked 2011 Census have been included, representing, over 9 million people in the 2011 Census and 7,000 deaths by suicide from 2011 to 2017. This age group was chosen because most deaths by suicide occur between these ages and because of the relative stability of socioeconomic factors over time (such as level of education) among this age group. While suicide is the leading cause of death among people aged 15 to 24 years, people in this age group were excluded from the modelling because of their lack of socioeconomic stability.
Missing values have been excluded from this analysis. Educational attainment has the highest proportion of missing values (5.5%). Unlike with the cumulative suicide risk estimations, the data used in the regression modelling has not been weighted.
To identify modelling predictors and explore their association with suicide deaths, an extensive literature review of social factors was carried out. This included earlier analyses published by AIHW, which showed deaths by suicide varied by factors such as employment and educational attainment.
Socioeconomic factors identified from the 2011 Census were used as predictors and deaths by suicide as the outcome variable. A total of 10 factors were included:
- Age (10-year age groups)
- Sex
- Indigenous status
- Registered marital status
- Family household composition
- Highest level of educational attainment
- Labour force participation
- Occupation
- Synthetic total income (quartiles, see Biddle & Marasinghe 2021)
- Need for assistance with core activities of daily living.
Method
Two modelling approaches were tested: Poisson regression and competing-risks regression (as described by Fine & Gray 1999). For Poisson regression, counts of the outcome variable with the value 1 for deaths by suicide and 0 for those who did not die by suicide were created and data aggregated by socioeconomic factor.
For the competing-risks regression, the influence of other causes of death is considered. This is because people who died from any other causes (such as cancer and coronary heart disease) are no longer at risk of dying by suicide.
Sex-stratified and Indigenous-stratified multivariate models were also fitted to investigate the associations within males and females, and within Indigenous and non-Indigenous people. Due to data quality issues including small sample sizes, Indigenous-stratified models have not been published. Univariate and multivariate models (including quasi-Poisson to deal with slight overdispersion) were also refitted. The coefficients obtained were back transformed so they could be interpreted as rate ratios (for Poisson models) and subhazard ratios (for competing-risks models). Analysis was conducted using R (glm package) and Stata (version 16) software.
Of the models tested, competing-risks regression, a method that accounts for people being censored from the risk set because of a competing cause, was used to estimate the risk of death by suicide and the selected socioeconomic factors. Univariate, multivariate and sex-stratified competing-risks models were developed. Generally, competing-risks regression models can be regarded as an extension of the Cox proportional hazards model, where subjects who experience competing events (deaths from other causes) are adequately counted as not having any chance of dying by suicide.
Estimated coefficients of competing-risks models can be interpreted in a similar way as coefficients estimated from a Cox model, except that they estimate the effect of certain covariates in the presence of competing events. Note that the transformed coefficients are known as subhazard ratios, similar to hazard ratios estimated in Cox regression. The subhazard ratio can be interpreted as a rate ratio (Henan 2010), but here we are considering the relative change in rates of the event in those subjects who are either currently event-free or who have previously experienced a competing event (Austin & Fine 2017). For simplicity and ease of understanding, coefficients in this report are referred to as hazard ratios.
Social and economic factors associated with suicide in Australia: a focus on individual income
Researchers from the Australian National University’s Centre for Social Research and Methods (CSRM), in close collaboration with the AIHW, have extended the analysis Regression risk models for selected census variables. An extract from the Multiagency Data Integration Project (MADIP) was used. For this analysis, the following MADIP datasets were utilized. 2011 Census information, 2011-2016 Personal income tax (PIT) records, 2011-2016 Social security and related information (SSRI) and 2011-2016 cause of death data. The data linkage process was identical to the linkage process described in the Data section of these Technical notes.
The following set of explanatory variables were used to capture the social and economic factors. More specifically, the CSRM used the time-invariant 2011 Census data to capture social factors and time-variant PIT and SSRI to capture economic factors of suicide.
Variable | Source | Type |
|---|---|---|
1. Highest level of education | 2011 Census | Social |
2. Age | 2011 Census | Social |
3. Sex | 2011 Census | Social |
4. Indigenous status | 2011 Census | Social |
5. Need for assistance with core activities | 2011 Census | Social |
6. Household composition | 2011 Census | Social |
7. Total income | 2011 – 2016 PIT | Economic |
8. SSRI | 2011 – 2016 SSRI | Economic |
In addition to the variables presented in Table 1, the following variables were derived using Census, PIT and SSRI data.
- A synthetic measure of income – A measure of income that was derived using a machine learning algorithm. This income variable provides a representative measure of income of the entire Australian population (Biddle and Marasinghe 2021). This measure was then divided into quintiles to obtain a relative measure of income.
- Coefficient variation of income (relative standard deviation) – Coefficient of variation of income was used to capture the income uncertainty of each individual. The measure was defined such that it captured income uncertainty between the current year and the previous year (i.e. variation between t and t-1). This measure was then divided into quintiles. An income uncertainty of quintile 1 implied an individual had low-income variation relative those in higher income uncertainty quintiles. Furthermore, since this measure uses data from t-1, the scope of the study was limited to 2012 January to 2016 December.
- Proxy for unemployment – Unemployment status of an individual was captured using SSRI information. More specifically, if an individual received Newstart allowance and Youth allowance, the individual was then classified as being unemployed that period.
Methods
Longitudinal (panel) regression
The MADIP dataset is a longitudinal dataset therefore, utilizing longitudinal regression methods allows us to control for unobserved individual heterogeneity across the time period. For example, longitudinal regression methods would allow us to control for unobserved measures such as behavioural differences and cultural differences across individuals. Given that suicide is a complex individual decision and may not be entirely explained by observed variables, controlling for these unobserved heterogeneity would allow us to obtain unbiased estimates.
In this analysis, two competing longitudinal regression methods were tested – a random effects logistic model and a population-averaged logistic model. Both models were estimated with robust standard errors to account for heteroskedasticity.
Given that the random effects logistic model is dependent on the strong assumption that the underlaying variation have no serial correlation, the population-averaged logistic model was selected as the primary regression method due to its robustness to serial correlation (Hill et al., 2010). Furthermore, a likelihood-ratio test was also undertaken to decide between the two models. The result suggested that the population-averaged model was more appropriate than the Random effects model. Equation (1) and (2) outline the population-averaged model.
Setting up the dataset as a panel allowed us to account for individual heterogeneity. However, given that suicide is a rare event, explanatory variables with large number of categories (for example – occupation) were excluded from the longitudinal analysis. This was primarily due the low number of suicides each year, which in turn made the models more sensitive to variables with a large number of categories. Given this drawback of panel data, a cross-sectional analysis was also conducted as a part of the sensitivity analysis.
Figure 1 - Annual suicide counts1
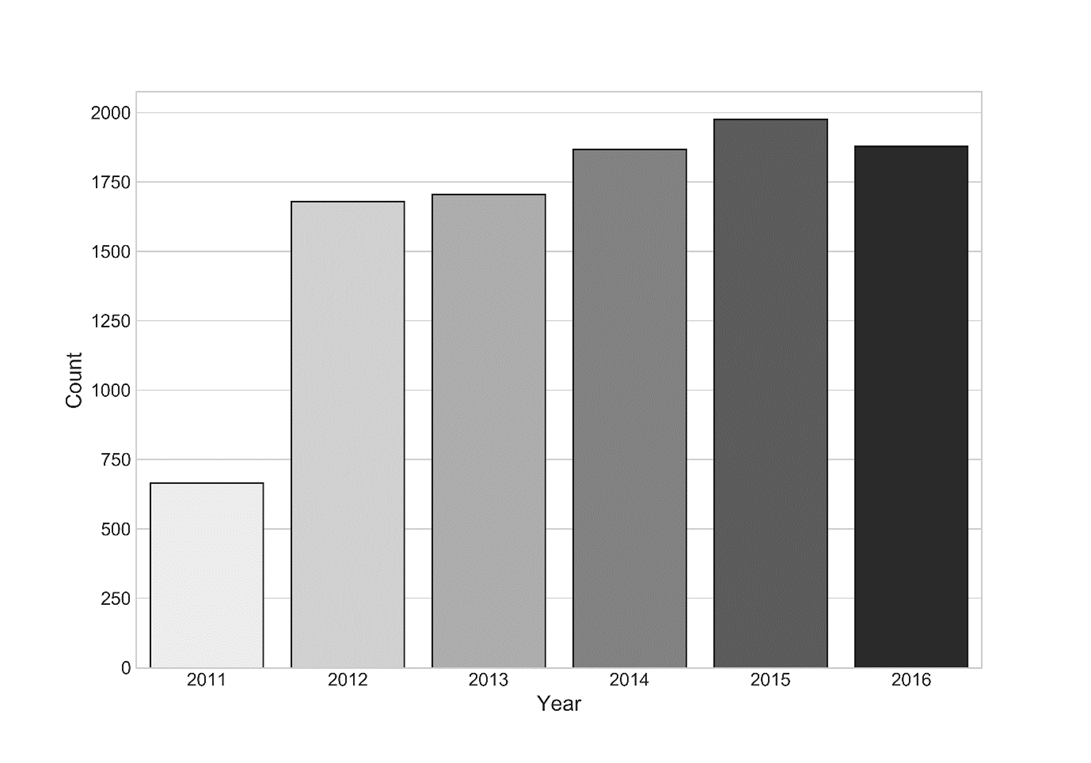
1. Year 2011 was not included in the analysis.
Reference
Hill, R.C., Griffiths, W.E. and Lim, G.C., 2010. Principles of econometrics. pp 537-560. John Wiley & Sons.
In addition to the NMD, the Australian Defence Force (ADF) suicide monitoring analysis used the following data sources:
National Death Index (NDI). The NDI is managed by the AIHW and contains person-level records of all deaths in Australia since 1980 obtained from the Registrars of Births, Deaths and Marriage in each state and territory. Its use is confined to data linkage studies approved by the AIHW Ethics Committee for health and medical research. NDI records are supplemented with cause of death information from the NMD. In this study, the NDI is linked with Defence payroll data to create the linked Defence payroll–NDI data set used in analysis of suicide in the ADF population.
Department of Defence personnel system data. The Department of Defence compiled a file of current and historical Defence personnel systems covering ADF members who have served since 1 January 1985. This combines PMKeyS, Core HR system, D1, CENRESPAY (for reservists), ADFPAY (for permanent members) and other historical payment systems. The Department of Defence and AIHW assessed the resulting file for completeness and duplicates. Comparisons were made with records from Department of Defence annual reports and other sources to validate the list. Data from the National Archives was also investigated for its suitability in validation, however as the majority of records are electronic files based on photos of paper records, this was not usable.
For further supplementary findings from the analyses and more detailed information about the data sources and methodology used in compiling data for serving and ex-serving ADF members, please see Technical notes of the Serving and ex-serving Australian Defence Force members who have served since 1985: suicide monitoring 1997 to 2022.
Estimates of fatal (years of life lost, YLL) and non-fatal burden (years lived with disability, YLD) were sourced from the Australian Burden of Disease Study (ABDS) 2022. The ABDS 2022 used burden of disease analysis to estimate the impact of 220 diseases and injuries on the health of the Australian population. The study provides a detailed picture of the burden of disease and injury in the Australian population in 2003, 2011, 2015, 2018 and 2022. It also includes estimates of the contribution made by selected risk factors on the disease and injury burden in Australia, and by socioeconomic areas for some risk factors.
The ABDS 2022 uses and adapts the methods of global studies to produce estimates that are more relevant to the Australian health policy context. The chosen reference period (2022) reflects the data availability from key data sources (such as the National Health Survey, deaths data, hospital admissions data and various disease registers) at the time of analysis.
Results from the study provide an important resource for health policy formulation, health service planning and population health monitoring. The results provide a foundation for further assessments.
Full details on the various methods, data sources and standard inputs used in the ABDS 2022 are available in Australian Burden of Disease Study 2022, Technical notes - Australian Institute of Health and Welfare (aihw.gov.au)
New South Wales Suicide Monitoring System
The New South Wales (NSW) Suicide Monitoring System contains data on all suspected and confirmed suicide deaths from 2019 to present. Established in October 2020, the system is a collaboration between the NSW Ministry of Health, Department of Communities and Justice, the State Coroner and NSW Police.
The NSW Suicide Monitoring System contains initial police information of suspected suicide deaths from the JusticeLink information system, which is managed by NSW Department of Communities and Justice. The information is manually checked against other data sources, including coronial determination.
NSW Health publishes monthly reports on suspected deaths by suicide in NSW on their website NSW Suicide Monitoring System.
Victorian Suicide Register
The Victorian Suicide Register (VSR) contains data on all suicide deaths reported to the Coroners Court of Victoria (CCOV) from 2000 to present. The Coroners Prevention Unit, a specialist investigative service for Victorian Coroners, has managed the VSR since its implementation in 2012. The VSR operates with funding from the Victorian Department of Health.
VSR data are used to inform investigations into suspected suicides and support coronial recommendations to prevent similar deaths. VSR data are regularly shared with the Victorian Department of Health, AIHW, Victoria Police and other organisations involved in suicide prevention.
Data on the VSR are obtained and coded from materials gathered throughout the course of coronial investigation, including police notification of death, forensic reports (autopsy and toxicology), witness statements and medical records.
CCOV releases a range of suicide data reports from the VSR on their website, including information on suspected deaths by suicide on a monthly basis, and overviews of First Nations suicides in Victoria. CCOV has also published a report on suicide among LGBTIQ+ people in Victoria.
Queensland Suicide Register and interim Queensland Suicide Register
In Queensland, there are two systems that are used to monitor suicide deaths: the Queensland Suicide Register (QSR), which includes suicide data since 1990 and is used to monitor longer-term trends, and the interim Queensland Suicide Register (iQSR). The iQSR was established in 2011 to provide real-time information on suicide deaths.
Data on this website are from the iQSR. The iQSR contains interim data on suspected suicides in Queensland, recorded shortly after the death occurs. The data are based on initial police reports and other information that is available to police at the time when they refer the death to the coroner.
The QSR contains information on suicide deaths for which coronial investigations have been finalised. The QSR is based on more information than the iQSR, including toxicology reports, post-mortem examination and the finding from the coroner, including details on the context and circumstances of the death.
The QSR and iQSR are currently managed by the Queensland Mental Health Commission (QMHC) on behalf of the Queensland Government, with support from the Coroners Court of Queensland (CCQ) and Queensland Police Service (QPS). Prior to September 2023, the iQSR was managed by the Australian Institute for Suicide Research and Prevention (AISRAP) at Griffith University. The QMHC publishes monthly reports based on data from the iQSR, around eight weeks from the last day of the reporting month. The QMHC also published the Suicide in Queensland: Annual Report 2023 which utilised data from the iQSR. The annual report summarises data on suspected suicides in Queensland for the calendar year 2023 and includes limited comparative data from previous years. Previous annual reports on the Queensland Suicide Register were published by the Australian Institute for Suicide Research and Prevention (AISRAP).
End of life service use for those who died from suicide in Australia
Data sources
Data are from the National Integrated Health Services Information Analysis Asset (NIHSI AA) version 0.5. This data asset includes mortality data together with information from hospital admissions, Medicare Benefits Schedule (MBS), Pharmaceutical Benefits Scheme (PBS) and residential aged care data.
The analysis population was those who had died between 1 July 2010 and 31 December 2017 in the linked National Deaths Index (NDI). Suicide was defined as the principal external cause of death in X60–X84 and Y87.0 based on the International Classification of Diseases, Tenth Revision (ICD-10) codes. Patient demographic information was taken from the NDI and is therefore accurate at the time of death not time of service. Only people whose age at death was between 15 to 64 years were included in the analysis. This was due to people in this age range making up the majority of those who die from suicide and to allow for better comparisons with deaths from other causes, which mostly occur in people older than 65 (AIHW 2022a). People without a primary cause of death and with sex not stated were also removed from the analysis due to small cell sizes.
Method
The analysis included MBS, PBS emergency department presentation and outpatient services in addition to hospital admissions datasets. For more information on MBS item classification and PBS item classification, drawn from the Anatomical Therapeutic Chemical (ATC) codes (AIHW 2022b), visit Mental health-related prescriptions.
Hospitalisation data was taken from two sources: admitted patients and emergency department (ED) presentations. The method for counting hospital admissions in this analysis based on the method in a similar study by Clapperton et al. (2021).
Within the NIHSI AA v0.5, hospital data pertains to only New South Wales (NSW), Victoria (Vic) (excluding Albury-Wodonga), South Australia (SA) and Tasmania (Tas) public hospitals. Admitted patient information also contains information from private hospitals in Victoria. To ensure accurate comparisons with hospitals data, only deaths registered in NSW, Vic, SA and Tas are included in the analysis.
Admitted patient data refers to only acute admitted and mental health separations (Admitted Patient Care National Minimum Data Set care types of 1, 7.1, 7.2, and 11). In scope separations where the patient was transferred from another hospital or had a change of care type in the same hospital are not counted in the total to avoid duplication.
Any hospital episode (ED presentation, hospital admission) that ended in “death” was excluded as it was considered to be a result of the fatal (suicide) incident. The only exception to this were episodes where the intentional self-harm was coded as occurring in a health service area–these episodes were retained as they were most likely inpatient suicides (Clapperton et al. 2021).
For admitted patient data, the definitions for mental health and self-harm behaviours include:
- ‘Any mental health’ hospitalisations are defined as any diagnosis (principal, secondary, etc.) of a mental disorder (ICD-10-AM codes F00–F99).
- Intentional self-harm hospitalisations are defined based on the ICD-10-AM principal diagnosis in the range S00–T75 or T79 and has a principal external cause code in the range X60–X84 or Y87.0.
- Suicidal ideation hospitalisations (ICD-10-AM code R45.81) are grouped with ‘any mental health’ and intentional self-harm hospitalisations, as this code is usually coded in the absence of a mental health condition.
For ED presentation data, the definitions ‘mental health-related ED presentations’ refers to presentations that have a principal diagnosis that falls within the Mental and behavioural disorders chapter (Chapter 5) of ICD‑10‑AM (codes F00–F99). It should be noted that this definition does not encompass all mental health‑related presentations to ED. See Mental health services in Australia for further information.
Note that diagnosis codes for intentional self-harm sit outside the Mental and behavioural disorders chapter (X60–X84). Additionally, an ED presentation for self-harm may have a principal diagnosis relating to the injury. These presentations cannot be identified as mental health-related presentations and are not included in this analysis (AIHW 2022).
Presentations to hospital emergency departments relating to suicide attempts or intentional self-harm cannot be easily identified in the current national emergency department data collection. Furthermore, ICD‑10‑AM diagnosis codes for intentional self-harm do not specify if there was suicidal intent or not – and therefore includes both suicide attempts and non-suicidal self-harming behaviours (AIHW 2022b). See Intentional self-harm hospitalisations for further information.
‘Any hospitalisation’ refers to any acute admitted/mental health care separation or ED presentation.
Limitations of this analysis includes:
- Mental health items could be miscoded or reported, for example, GP mental health services are typically billed under general GP consultations.
- Service use captured in the NIHSI is influenced by severity of condition, a person’s ability and desire to access a service, and the availability of alternative services not captured in the data (e.g. private community mental health services).
References
Australian Institute of Health and Welfare (AIHW) (2022a) Deaths in Australia, AIHW, Australian Government, accessed 11 October 2022.
Australian Institute of Health and Welfare (AIHW) (2022b) Mental health services in Australia, AIHW, Australian Government, accessed 09 September 2022
AIHW (2022c) Intentional self-harm hospitalisations, National Suicide and Self-harm Monitoring System, AIHW, Australian Government, accessed 14 October 2022.
Clapperton A, Dwyer J, Millar C, Tolhurst P and Berecki-Gisolf J (2021) ‘Sociodemographic characteristics associated with hospital contact in the year prior to suicide: A data linkage cohort study in Victoria, Australia’, PLoS ONE, 16(6): e0252682, doi:10.1371/journal.pone.0252682.