Gap in disease burden
Figure 1: Age-specific total burden rates (DALY per 1,000 people) and rate ratios, by age group, by Indigenous status, 2022
Grouped column chart showing both absolute and relative difference by Indigenous status. Across all age groups, First Nations people experience higher rates of burden than non-Indigenous people.

Figure 2: Gap (rate ratio and rate difference) in total burden, by disease group, 2022
Combined column chart showing the gap (rate ratio and rate difference) in total burden by disease group. The largest rate ratio was for kidney & urinary diseases and the largest rate difference was for cardiovascular diseases.

Figure 3: Percentage contribution (% of rate difference) of disease groups to the gap in total (DALY), non-fatal (YLD) and fatal (YLL) burden, 2022
Stacked bar chart showing proportional contribution of disease groups to the gap by type of burden. For DALY and YLL, cardiovascular was the largest contributor. For YLD, it was mental health conditions and substance disorders use.

Figure 4: Percentage contribution (% of rate difference) of disease groups to the gap in total disease burden (DALY), by sex, 2022
Stacked bar chart showing proportional contribution of diseases groups to the gap in DALY, by sex. For males, the largest contributor was cardiovascular diseases, while for females, it was mental health conditions and substance disorders use.

Figure 5: Percentage contribution (%) to the health gap (based on DALY rate difference) between First Nations people and non-Indigenous Australians, by age and disease group, 2022
Stacked bar chart showing proportional contribution to the health gap (based on DALY difference), by age and disease group. The contribution of different disease groups to the gap in total disease burden vary by age.

Which specific diseases and injuries contribute most to the gap?
Table 3 presents the top 5 specific causes contributing to the gap in total burden for First Nations males and females in 2022; together they accounted for over about one-third of the gap (33% for males and 31% for females). For information on how specific causes are classified under each disease group see Australian Burden of Disease Study: Methods and supplementary material 2018, Disease specific methods - morbidity.
For males in 2022, the specific causes that were leading contributors to the gap in total burden between First Nations people and non-Indigenous Australians were:
- coronary heart disease (CHD) (accounting for 10% of the gap for males)
- chronic obstructive pulmonary disease (COPD) (7.5% of the gap)
- suicide & self-inflicted injuries (5.6% of the gap).
For females in 2022, the specific causes that were leading contributor to the gap in total burden between First Nations people and non-Indigenous Australians were:
- COPD (accounting for 8.6% of the gap for females)
- CHD (7.6% of the gap)
- Type 2 diabetes (5.9% of the gap).
Sex and leading specific diseases | First Nations rate per 1,000 | Non-Indigenous rate per 1,000 | Rate ratio | Rate difference | Gap contribution (percent) |
|---|---|---|---|---|---|
Males | - | - | - | - | - |
Coronary heart disease | 41.6 | 16.3 | 2.6 | 25.3 | 10.5 |
COPD | 24.3 | 6.1 | 4.0 | 18.1 | 7.5 |
Suicide & self-inflicted injuries | 21.6 | 8.1 | 2.7 | 13.5 | 5.6 |
Type 2 diabetes | 17.0 | 5.0 | 3.4 | 12.0 | 5.0 |
Alcohol use disorders | 13.7 | 3.7 | 3.7 | 10.1 | 4.2 |
Females | - | - | - | - | - |
COPD | 24.1 | 5.8 | 4.1 | 18.2 | 8.6 |
Coronary heart disease | 23.0 | 6.7 | 3.4 | 16.3 | 7.6 |
Type 2 diabetes | 15.6 | 3.1 | 5.0 | 12.5 | 5.9 |
Chronic kidney disease | 12.2 | 1.7 | 7.1 | 10.5 | 4.9 |
Lung cancer | 13.6 | 4.4 | 3.1 | 9.1 | 4.3 |
Source: AIHW First Nations Burden of Disease Database
Gap in burden has narrowed over time
After removing differences in population size and age structure, the absolute gap in burden (DALY rate difference) between First Nations people and non-Indigenous Australians decreased by 8.8% between 2011 and 2022, from 249 to 227 per 1,000 people. There was a small drop in the relative gap, from a rate ratio of 2.2 in 2011 to 2.1 in 2022. This was largely driven by a narrowing of the gap for fatal burden, which decreased by 9.8% between 2011 and 2022. The gap in non-fatal burden also decreased during this period, by 7.4% (Figure 6). There was no change in the relative gap for fatal burden (a rate ratio of 2.4 in 2011 and 2022), while there was a slight drop for non-fatal burden (from a rate ratio of 2.0 in 2011 to 1.9 in 2022).
Figure 6: Change between 2011 and 2022 in the gap in age-standardised total (DALY), fatal (YLL), and non-fatal (YLD) burden rate (per 1,000 people) between First Nations people and non-Indigenous Australians
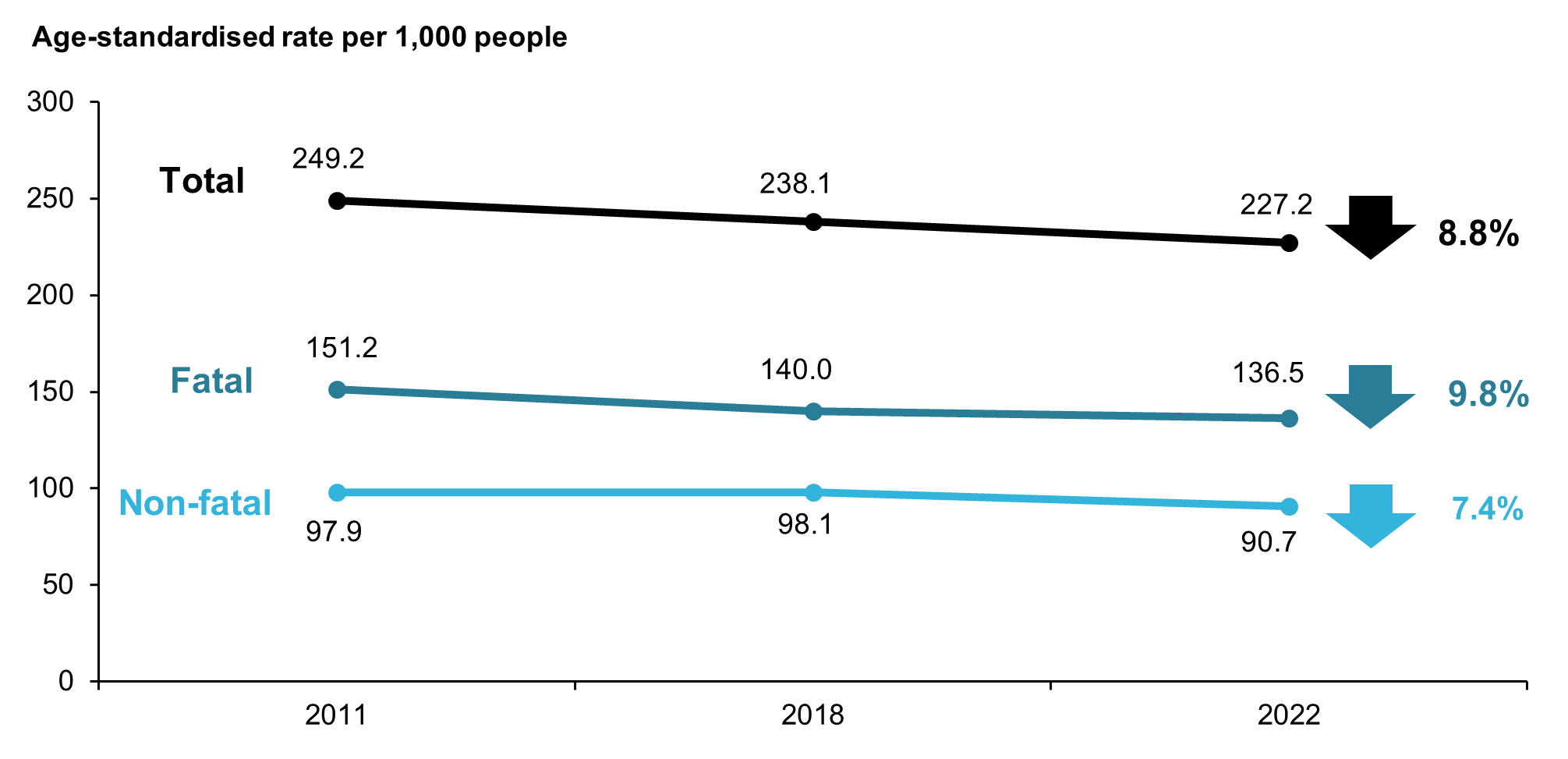
Note: Rates were age-standardised to the 2001 Australian Standard population.
Source: AIHW First Nations Burden of Disease Database
Change in the absolute gap in burden (DALY rate difference) was driven by a larger proportional decrease in the rate of total burden for First Nations people (6.3% decrease, from 457 to 429 DALY per 1,000 people) than for non-Indigenous Australians (3.2% decrease, from 208 to 202 per 1,000 people) between 2011 and 2022 (Figure 7).
For fatal burden, there were similar proportional declines in the age-standardised rate for First Nations people (11% decrease, from 262 to 233 YLL per 1,000 people) and non-Indigenous Australians (12% decrease, from 111 to 97 YLL per 1,000 people) (Figure 7).
For non-fatal burden, there was no substantial change in the age-standardised rate for First Nations people between 2011 and 2022 (0.1% decrease) but the rate for non-Indigenous Australians increased (7.3% increase, from 98 to 105 YLD per 1,000 people) over the same period (Figure 7).
Figure 7: Change between 2011 and 2022 in the age-standardised total (DALY), non-fatal (YLD), and fatal (YLL) burden rate (per 1,000 people), First Nations people and non-Indigenous Australians
Line graph showing change in age-standardised burden rates over between 2011 and 2022 for First Nations people and non-Indigenous Australians, by type of burden, sex and disease group. There was a larger proportional decrease in the rate of total burden for First Nations people than non-Indigenous people.

Figure 8: Percentage contribution (%) of disease groups to the gap in total disease burden between First Nations people and non-Indigenous Australians (based on DALY rate differences), 2011 and 2022
Stacked bar chart showing proportional contribution of disease groups to the gap (based on DALY rate difference) between 2011 and 2022. The top five causes remained the same between years and their contribution increased for all causes, except cardiovascular diseases.

Figure 9: Percentage contribution (%) of disease groups to excess total (DALY), excess non-fatal (YLD) and excess fatal (YLL) burden, First Nations people, 2022
Stacked bar chart showing proportional contribution of disease groups to excess burden, by burden type. For both DALY and YLD, mental health conditions and substance use disorders was the largest contributor to excess burden. For YLL, injuries was the largest contributor to excess YLL burden.

Figure 10: Expected and excess fatal (YLL) and non-fatal (YLD) burden by type of burden and disease group, First Nations people, 2022
Stacked bar chart showing expected and excess YLL and YLD burden, by type of burden and disease group. Mental health conditions and substance use disorders had the largest number of excess YLD burden and injuries had the largest number of excess YLL burden.

Contribution of fatal and non-fatal burden to excess burden
In 2022, over half of the total excess burden experienced by First Nations people was due to excess fatal burden (57%, 99,033 YLL out of 172,639 DALY) (Figure 11). Among the disease groups with the highest amounts of excess burden:
- almost all the excess total burden from mental health conditions & substance use disorders was non-fatal burden (97%, 31,750 YLD out of 32,674 DALY)
- most of the excess burden from injuries and cardiovascular diseases was fatal burden (90% and 88%, respectively).
Figure 11: Percentage contribution (%) of fatal (YLL) and non-fatal (YLD) to excess total burden (DALY) by disease group, First Nations people, 2022

Note: Data for reproductive & maternal conditions not shown due to small numbers.
Source: AIHW First Nations Burden of Disease Database
Top specific diseases contributing to excess burden
The top 5 specific diseases contributing to excess burden together accounted for over a quarter (28%) of the total excess burden for First Nations people in 2022 (Table 5). The specific diseases that were leading contributors to excess burden were:
- coronary heart disease (accounting for 7.9% of total excess burden, or 13,572 of 172,639 DALY)
- COPD (5.8% of excess burden, 9,983 excess DALY)
- suicide & self-inflicted injuries (5.4% of excess burden, 9,371 excess DALY)
- type 2 diabetes (4.6% of excess burden, 8,024 excess DALY)
- anxiety disorders (4.3% of excess burden, 7,360 excess DALY).
Causes | DALY | Expected DALY | Excess DALY | % of total excess DALY |
|---|---|---|---|---|
Coronary heart disease | 19,023 | 5,451 | 13,572 | 7.9 |
COPD | 12,776 | 2,793 | 9,983 | 5.8 |
Suicide & self-inflicted injuries | 14,421 | 5,050 | 9,371 | 5.4 |
Type 2 diabetes | 10,198 | 2,174 | 8,024 | 4.6 |
Anxiety disorders | 15,832 | 8,473 | 7,360 | 4.3 |
Leading 5 specific causes | 72,250 | 23,941 | 48,309 | 28.0 |
All other causes | 245,083 | 120,753 | 124,329 | 72.0 |
Total | 317,333 | 144,694 | 172,639 | 100.0 |
Source: AIHW First Nations Burden of Disease Database
Excess burden within individual diseases
In 2022, among First Nations people, the amount of burden considered to be excess differed for individual causes of burden. Causes with the highest proportional excess burden included:
- scabies (100% of DALY considered excess, 264 of 264 DALY)
- protein-energy deficiency (94% considered excess, 1,905 of 2,028 DALY)
- rheumatic heart disease (94% considered excess, 1,351 of 1,438 DALY)
- chronic kidney disease (87% considered excess, 5,887 of 6,783 DALY)
- hearing loss (84% considered excess, 6,740 of 8,029 DALY).