Pregnant women
-

Most injuries were due to falls
71 hospitalisations, 34% of injuries among pregnant women in 2022–23.
-

Assault in pregnancy
Among women hospitalised due to assault in 2022–23, higher proportions of pregnant women were assaulted by their spouses or partners than women who were not pregnant
-
A spouse or domestic partner was the recorded perpetrator for 70% of assault injury hospitalisations for pregnant women
This section will be limited to injury hospitalisations among pregnant women only. ED presentations are not reported for pregnant women due to the quality of available information. For information on deaths during pregnancy, please see AIHW Maternal deaths report.
Injuries occur in around 8% of pregnancies and are one of the leading non-obstetric causes for maternal morbidity and mortality (AIHW 2023; ECI 2018). There are physiological and social factors associated with pregnancy that increases a woman’s risk of injury.
Of the 293,435 women who gave birth in 2022, 246,617 (84%) were aged 25 to 39 years (AIHW 2024a). In 2022–23, 2,130 pregnant women in Australia were hospitalised for an injury. Women aged 25 to 39 made up almost 3 out of 4 of these hospitalisations and had the highest rate of injury hospitalisation (55.0 per 100,000 population) (Table 13).
Age group (years) | Count | % |
|---|---|---|
19-24 | 475 | 22.3 |
25-39 | 1,582 | 74.2 |
40-64 | 73 | 3.4 |
Total | 2,130 | 100 |
Sources: AIHW National Hospital Morbidity Database.
Notes:
- Only includes records where patient was aged 19 and over and patient’s sex recorded as female.
- Due to rounding, sum of column percentages may not equal 100%.
- A hospitalised person was identified as pregnant if they had an additional diagnosis in the ICD-10-AM range O00 to O99 or in Z33, Z34, Z35.
Number of pregnant women hospitalised for injury decreased since COVID-19 period
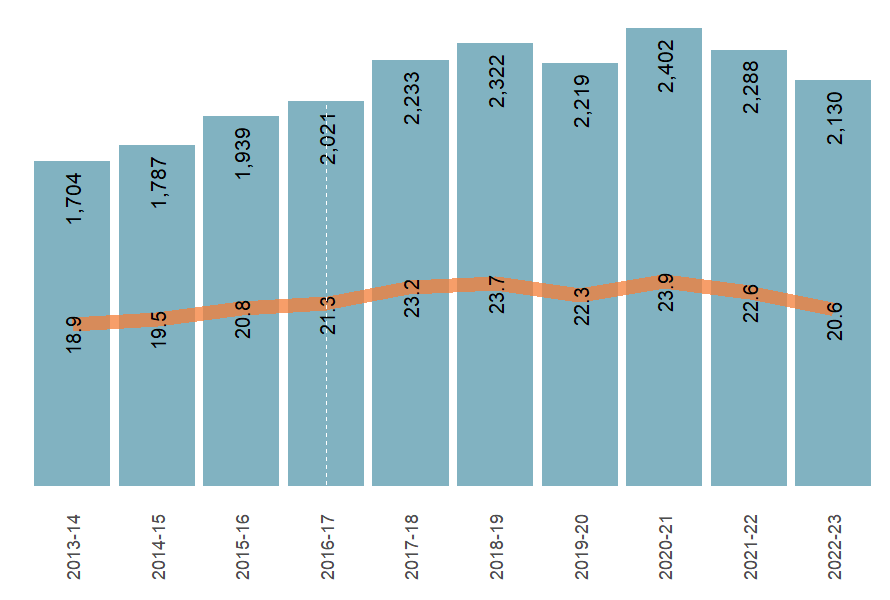
The number of injury hospitalisations among pregnant women has decreased slightly from 2,233 hospitalisations in 2017–18 to 2,130 hospitalisations in 2022–23, peaking at 2,402 hospitalisations in 2020-21 (Figure 36).
Figure 36: Number and crude rate (per 100,000) of injury hospitalisations for pregnant women, Australia, 2013–14 or 2022–23
Sources: AIHW National Hospital Morbidity Database.
Notes:
- Only includes records where patient was aged 19 and over and patient’s sex recorded as female.
- Rates are crude per 100,000 population.
- A hospitalised person was identified as pregnant if they had an additional diagnosis in the ICD-10-AM range O00 to O99 or in Z33, Z34, Z35.
- Columns are case counts, the line graph presents crude rate per 100,000 population.
- The dashed line presents a break in the time series, see Technical notes for detail.
Falls, transport accidents and assault were the leading causes of injury hospitalisation among pregnant women
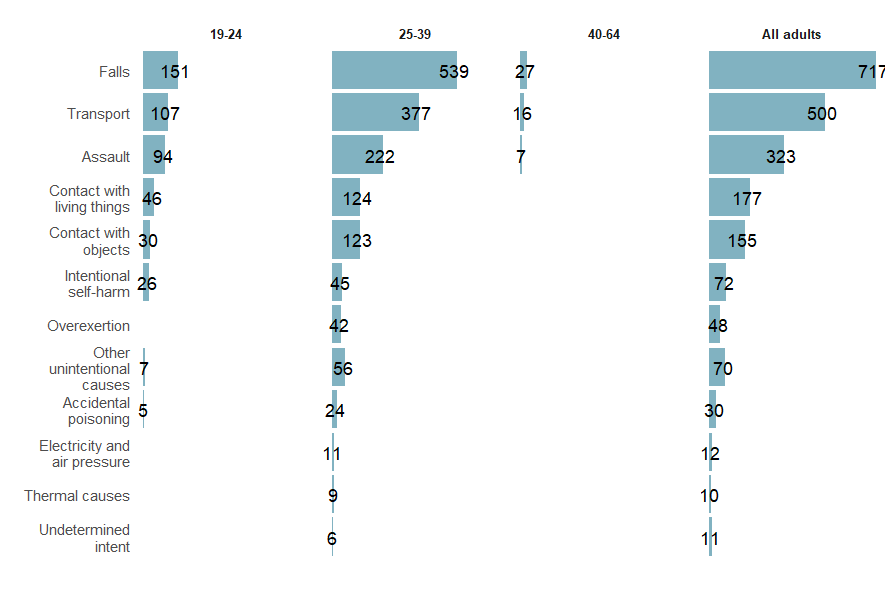
Among pregnant women hospitalised for an injury in 2022–23, the top 3 leading causes were (Figure 37):
- Falls (717 injury hospitalisations, or 33.7%)
- Transport (500 injury hospitalisations, or 23.5%)
- Assault (323 injury hospitalisations, or 15.2%).
These leading causes were consistent across all age groups among pregnant women. Pregnant women aged 25 to 39 had the highest rate of injury hospitalisations for all causes, except for assault, where the highest rate was observed for pregnant women aged 19 to 24 years (94 hospitalisations, 9.8 per 100,000 population).
Figure 37: Number of injury hospitalisations for pregnant women by cause of injury and age group, Australia, 2022–23
Sources: AIHW National Hospital Morbidity Database.
Notes:
- Only includes records where patient was aged 19 and over and patient’s sex recorded as female.
- Counts under 5 are excluded from display.
- Records where external cause of injury was not reported are excluded from display.
- A hospitalised person was identified as pregnant if they had an additional diagnosis in the ICD-10-AM range O00 to O99 or in Z33, Z34, Z35.
Over a third of injury hospitalisations among pregnant women were due to falls
There are physiological factors associated with pregnancy that can increase a woman’s risk of injury. These factors include altered balance and increased fatigue which can increase vulnerability to falls and related injuries (Cakmak et al. 2015; Condor et al. 2019).
In 2022–23, 717 pregnant women were hospitalised for injury due to falls, making up 34% of all injury hospitalisations for pregnant women. The top 3 leading type of falls resulting in injury hospitalisation were:
- Fall on same level from slipping, tripping and stumbling (W01) (336 hospitalisations)
- Other fall on same level (W18) (123 hospitalisations)
- Fall on and from stairs and steps (W10) (120 hospitalisations)
Among women’s assault injury hospitalisations, a higher proportion of pregnant women were assaulted by their spouse or partner than women who were not pregnant
Pregnancy and assault: a broader context
Women are at an increased risk of experience family, domestic and sexual violence (FDSV) during pregnancy and if they are already experiencing violence, the severity is likely to increase while pregnant (AIFS 2015; AIHW 2024b; AIJA 2022). National guidelines for clinical care recommend all women are routinely screened for FDSV during pregnancy and in first year after birth (Highet et al. 2023). The increased risk of FDSV during pregnancy is often linked to factors such as dependency and relationship power dynamics, increased stress and social isolation (AIJA 2024). Please refer to the AIFS’ paper on Domestic and family violence in pregnancy and early parenthood for more detail on the factors and effects of FDSV during pregnancy.
Among assault injury hospitalisations in women in 2022–23, 323 (4.2%) were pregnant. A spouse or domestic partner was reported as the perpetrator for 70.3% of assault injury hospitalisations among pregnant women compared with 50.0% of assault injury hospitalisations among women who were not pregnant (Table 14). For 4.0% of assault injury hospitalisations among pregnant women, the reported perpetrator was an unspecified person, a lower proportion than for assault injury hospitalisations among non-pregnant women (15.0%).
Perpetrator | Assault injury hospitalisations of pregnant women | % | Assault injury hospitalisations of not pregnant women | % |
|---|---|---|---|---|
Spouse or domestic partner | 227 | 70.3 | 3,475 | 50.0 |
Parent | 7 | 2.2 | 69 | 1.0 |
Other family member | 33 | 10.2 | 927 | 13.2 |
Acquaintance or friend | 10 | 3.1 | 515 | 7.4 |
Person unknown to the victim | 9 | 2.8 | 390 | 5.6 |
Multiple persons unknown to the victim | 5 | 1.5 | 149 | 2.1 |
Other specified person | 19 | 5.9 | 357 | 5.1 |
Unspecified person | 13 | 4.0 | 1,046 | 15.0 |
All assault hospitalisations | 323 | 100 | 6,955 | 100 |
Sources: AIHW National Hospital Morbidity Database.
Notes:
- Only includes records where patient was aged 19 to 64 years and patient’s sex recorded as female.
- Counts under 5 are excluded from display.
- A hospitalised person was identified as pregnant if they had an additional diagnosis in the ICD-10-AM range O00 to O99 or in Z33, Z34, Z35.
- Perpetrator is derived from the nominal external cause.
Pregnant women were more likely to be assaulted and injured on their trunk than women who were not pregnant
Around one in 3 pregnant women (105 hospitalisations or 32.5%) who were hospitalised for an assault injury were hospitalised for an injury to their trunk (thorax, abdomen, lower back, lumbar spine & pelvis) in 2022–23, a higher proportion than those who were not pregnant (969 hospitalisations or 13.9%) (Table 15). For women hospitalised for an assault injury, injuries to the head and neck were less common among pregnant women (149 hospitalisations or 46.1%) than women who were not pregnant (4,106 hospitalisations or 59.0%).
Body part injured | Hospitalisations for pregnant women | % | Hospitalisations for non-pregnant women | % |
|---|---|---|---|---|
Head and neck | 149 | 46.1 | 4,106 | 59.0 |
Trunk (thorax, abdomen, lower back, lumbar spine & pelvis) | 105 | 32.5 | 969 | 13.9 |
Shoulder and upper limb (excluding wrist and hand) | 26 | 8.0 | 622 | 8.9 |
Hip and lower limb (excluding ankle and foot) | 13 | 4.0 | 328 | 4.7 |
Wrist and hand | 9 | 2.8 | 534 | 7.7 |
Injuries not described in terms of body location | 19 | 5.9 | 305 | 4.4 |
Sources: AIHW National Hospital Morbidity Database.
Notes:
- Only includes records where patient was aged 19 to 64 years and patient’s sex recorded as female.
- Counts under 5 are excluded from display.
- A hospitalised person was identified as pregnant if they had an additional diagnosis in the ICD-10-AM range O00 to O99 or in Z33, Z34, Z35.
- Body part injured is derived from the principal diagnosis.
For more information, see supplementary data tables.