Technical notes
On this page:
Data presented in this web report are sourced from a range of data collections. The latest data have been used wherever possible. Data are subject to change due to:
- the nature and timing of the data collection;
- a regular program of updates and maintenance;
- and revisions to address errors or anomalies.
Revisions and changes in coverage should be considered when interpreting changes over time.
Descriptions of the data sources used in this web report are below. These include information on the data provider and data specifications such as remoteness classification, cultural and linguistic diversity (CALD) definition and sex or gender definition.
Sex and gender
This report uses the terms female/male and women/men interchangeably, unless otherwise stated under data specifications for each indicator. However, it is often not clear from the data sources whether these terms relate to sex or gender. Most data sources are based on surveys or service provision records where a person is likely to record how they identify, so the term ‘gender’ is used, except where the data supplier has requested otherwise. Indicators that may include data relating to children use the term ‘sex or gender’. ‘Other’ or ‘non-binary’ categories are not presented separately in the report due to low counts but may be combined with an ‘unknown’ or ‘missing’ category and included in the Supplementary data tables where available. Reporting will be updated in the future if data permit.
Remoteness areas
Two remoteness classifications are used in this report: the Australian Statistical Geography Standard (ASGS) Remoteness Structure and the Modified Monash Model (MMM). For more information about the impact of geographic location on health outcomes, see Rural and remote health.
Significance testing
When comparing two different estimates, it is important to determine whether the difference is likely to reflect a true difference in the underlying population or whether it may be due to sampling error. This process is called ‘significance testing’. There are several variables that are used to calculate whether two estimates are significantly different – the size of the difference, the variability in the sample collected (which indicates the level of sampling error present), and the size of the sample. Sometimes, even large apparent differences may not be statistically significant. This is particularly the case where there are small sample sizes. Conversely, with a sufficiently large sample, small changes are more likely to be statistically significant.
In this report, significance testing was available for the following data sources, and is described in the sections below:
Data sources
- Australian Dementia Network (ADNeT) Registry
- Aged Care Provider Workforce Survey
- Carer Wellbeing Survey
- Dementia Australia
- Dementia Awareness Survey
- Dementia Support Australia
- Dementia Training Australia
- National Carer Survey
- National Centre for Vocational Education Research (NCVER)
- National Disability Insurance Scheme (NDIS)
- National Health Data Hub (NHDH)
- Palliative Care Outcomes Collaboration (PCOC)
Australian Dementia Network (ADNeT) Registry
The Australian Dementia Network (ADNeT) Registry is a clinical quality registry for people newly diagnosed with dementia or mild cognitive impairment (MCI). Aggregated data was provided to the AIHW through a data request.
ADNeT Registry participating sites are specialised clinical services where dementia and MCI are diagnosed. These include multi-disciplinary memory and cognitive disorders clinics, other specialised dementia and MCI diagnostic services, aged care outreach services, as well as single-discipline medical practitioners (for example, geriatricians, neurologists, and psychiatrists). Sites represent both public and private services and include clinics that deliver some or all their services via telehealth. Site participation in the ADNeT Registry is voluntary.
The ADNeT Registry has ethical approval from the Alfred Hospital Human Research Ethics Committee under the National Mutual Acceptance Scheme (Project Number: 44037). Eligible participants for the ADNeT Registry are individuals aged 18 years and over who receive a new diagnosis of either dementia or MCI at a participating site. After a participant is deemed eligible by the participating site, they are recruited using an opt-out approach. A participant may be recruited using a waiver of consent in certain circumstances (for example, the participant has impaired decision-making capacity and does not have a person responsible who can make decisions on their behalf).
Participating sites enter data for eligible participants at the time of diagnosis, based on the ADNeT Registry Minimum Data Set. These data include personal identifiers, demographics, and relevant clinical details pertaining to diagnostic work-up, diagnosis, cognition, function, comorbidities, and aspects of initial management.
After a participant is recruited into the Registry, where appropriate, data on health and wellbeing and the experience of clinical care at the participating site are collected via surveys completed by the participants and their carers (if identified). These surveys have been developed by a working group comprising representatives of people with lived experience, carers, peak bodies, clinicians, and researchers, and underwent consultation with people with living experience of dementia and MCI and their carers (facilitated by Dementia Australia).
ADNeT Registry data may not be representative of all people being diagnosed with dementia or MCI in specialist diagnostic services across Australia. In 2024, 74 services participated across Australia: 54 services were located in Major cities, 14 in Inner regional areas, 6 in Outer regional areas, and none were located in Remote or Very remote areas. Nationally representative data on specialist diagnostic services are needed to complement ADNeT Registry data and better understand the national impact of the Action Plan. The ADNeT Registry expanded in July 2025 to collect post-market surveillance data on disease-modifying therapies that are approved in Australia for people living with dementia or MCI.
Indicators reflect baseline values from the 2024 reference period. Additional data from 2020-2023 are included in the supplementary tables.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 1.4 People in regional, rural and remote settings have improved access to dementia diagnosis and support |
Indicator | Number of services participating in the Australian Dementia Network (ADNeT) Registry that are located in regional or remote areas. |
Time period | Data covers the period from March 2020 (registry commencement) to December 2024. |
Disaggregation | Age group, sex, type of diagnosis. |
Definitions | Remoteness data are based on the site’s location, and based on the Remoteness structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Note that no ADNeT sites were located in Remote or Very remote areas. |
Measure | 1.4 People in regional, rural and remote settings have improved access to dementia diagnosis and support |
Indicator | Number of new participants who joined the Australian Dementia Network (ADNeT) Registry who live in regional or remote areas. |
Disaggregation | Age group, sex, type of diagnosis. |
Definitions | Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in the 2020–2023 period. For 2024 data, participants with missing postcodes are reported as having missing remoteness. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Age of participants refers to age at time of diagnosis. Ages were aggregated into three broad groups when the data was supplied to the AIHW, due to privacy reasons: under 65 years; 65–84 years; 85+ years. Type of diagnosis: dementia or mild cognitive impairment. |
Measure | 4.2 Increased number of people assessed in memory clinics |
Indicator | Number of new participants who joined the Australian Dementia Network (ADNeT) Registry. |
Time Period | Data covers the period from March 2020 (registry commencement) to December 2024. |
Disaggregation | Age group, sex, type of diagnosis, remoteness area, whether born in a main English-speaking country. |
Definitions | Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in the 2020-2023 period. For 2024 data, participants with missing postcodes are reported as having missing remoteness. ‘Regional areas' includes Inner regional, Outer regional, Remote and Very remote areas. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Age of participants refers to age at time of diagnosis. Ages were aggregated into three broad groups when the data was supplied to the AIHW, due to privacy reasons: under 65 years; 65–84 years; 85+ years. Main English-speaking countries are grouped based on the ABS’ definition, and include Australia, the United Kingdom, Republic of Ireland, New Zealand, Canada, the United States of America, and South Africa. Type of diagnosis: dementia or mild cognitive impairment. |
Measure | 4.4 Increased number of people with signs and symptoms of dementia who are seen by a specialist within 3 months of receiving a referral |
Indicator | Proportion of participants in the Australian Dementia Network (ADNeT) Registry who had their initial appointment with a specialist diagnostic service within 3 months of referral. |
Time period | Data covers the period from March 2020 (registry commencement) to December 2024. |
Numerator | Number of all ADNeT Registry participants who were seen by a specialist within 3 months. |
Denominator | Number of all ADNeT Registry participants. Participants with missing/unknown responses were excluded from the denominator. |
Disaggregation | Age group, sex, type of diagnosis, remoteness area, whether born in a main English-speaking country. |
Definitions | Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in the 2020-2023 period. For 2024 data, participants with missing postcodes are reported as having missing remoteness. ‘Regional areas' includes Inner regional, Outer regional, Remote and Very remote areas. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Age of participants refers to age at time of diagnosis. Ages were aggregated into three broad groups when the data was supplied to the AIHW, due to privacy reasons: under 65 years; 65–84 years; 85+ years. Main English-speaking countries are grouped based on the ABS’ definition, and include Australia, the United Kingdom, Republic of Ireland, New Zealand, Canada, the United States of America, and South Africa. Type of diagnosis: dementia or mild cognitive impairment. |
Measure | 4.5 Reduction in the average time taken for people to receive a diagnosis of dementia from the onset of first symptoms |
Indicator | Proportion of people with dementia participating in the Australian Dementia Network (ADNeT) Registry who had an initial appointment with diagnostic services within 1 year of symptom onset. |
Time Period | Data covers the period from April 2023 (commencement of data collection for this variable) to December 2024. |
Numerator | Number of all ADNeT Registry participants diagnosed with dementia, who had an initial appointment with diagnostic services within 1 year of symptom onset. |
Denominator | Number of all ADNeT Registry participants who were diagnosed with dementia. Participants with missing/unknown responses were excluded from the denominator. |
Disaggregation | Age group, sex, remoteness area, whether born in a main English-speaking country. |
Definitions | Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in 2023. For 2024 data, participants with missing postcodes are reported as having missing remoteness. ‘Regional areas' includes Inner regional, Outer regional, Remote and Very remote areas. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Age of participants refers to age at time of diagnosis. Ages were aggregated into three broad groups when the data was supplied to the AIHW, due to privacy reasons: under 65 years; 65–84 years; 85+ years. Main English-speaking countries are grouped based on the ABS’ definition, and include Australia, the United Kingdom, Republic of Ireland, New Zealand, Canada, the United States of America, and South Africa. Only people with a diagnosis of dementia are included in this indicator. |
Measure | 4.7 Increased number of people living with dementia and their carers reporting a positive experience of diagnostic and post-diagnostic care |
Indicator | Proportion of Australian Dementia Network (ADNeT) Registry survey respondents whose experience with diagnostic services was good or very good. |
Time Period | Data covers the period from March 2021 to December 2024. |
Numerator | Number of post-diagnostic survey respondents who reported having a good or very good experience. |
Denominator | Number of all post-diagnostic survey respondents. |
Disaggregation | Sex, type of diagnosis, remoteness area, whether born in a main English-speaking country. |
Definitions | Data reported for this indicator relates to participants whose data were submitted to the ADNeT Registry since the commencement of survey implementation in March 2021 to December 2024. The survey response rate was 50.1% for the period March 2021 to December 2023, and 42.6% for 2024. Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in the 2021-2023 period. For 2024 data, participants with missing postcodes are reported as having missing remoteness. ‘Regional areas' includes Inner regional, Outer regional, Remote and Very remote areas. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Main English-speaking countries are grouped based on the ABS’ definition, and include Australia, the United Kingdom, Republic of Ireland, New Zealand, Canada, the United States of America, and South Africa. Data for 2024 were not published due to low counts. Type of diagnosis: dementia or mild cognitive impairment. Carer Survey results are provided in Supplementary table S4.7.1c and are stratified by year only, not type of diagnosis. |
Measure | 4.7 Increased number of people living with dementia and their carers reporting a positive experience of diagnostic and post-diagnostic care |
Indicator | Proportion of people participating in the Australian Dementia Network (ADNeT) Registry referred to a post-diagnostic program at the time of a dementia diagnosis. |
Time Period | Data covers the period from April 2023 to December 2024. |
Numerator | Number of ADNeT Registry participants diagnosed with dementia who were referred to a post-diagnostic program at the time of a dementia diagnosis. |
Denominator | Number of ADNeT Registry participants diagnosed with dementia. Participants with missing/unknown responses were excluded from the denominator. |
Disaggregation | Age group, sex, remoteness area, whether born in a main English-speaking country. |
Definitions | Remoteness data are based on participants postcodes and the Remoteness Structure as defined by the Australian Statistical Geography Standard (ASGS) Edition 3. Site postcodes were used for participants with missing values in 2023. For 2024 data, participants with missing postcodes are reported as having missing remoteness. ‘Regional areas' includes Inner regional, Outer regional, Remote and Very remote areas. Only a small number of participants were located in Remote or Very remote areas. Due to low counts, breakdowns by sex exclude participants who did not identify as male or female. These participants are included in the ‘Missing/unknown’ category. Age of participants refers to age at time of diagnosis. Ages were aggregated into three broad groups when the data was supplied to the AIHW, due to privacy reasons: under 65 years; 65–84 years; 85+ years. Main English-speaking countries are grouped based on the ABS’ definition, and include Australia, the United Kingdom, Republic of Ireland, New Zealand, Canada, the United States of America, and South Africa. The ADNeT Registry only collects this information for people diagnosed with dementia. |
Aged Care Provider Workforce Survey
The 2023 Aged Care Provider Workforce Survey provides the government with information on the size, composition and characteristics of the aged care workforce in residential aged care and in-home care settings.
The survey captures information across five key industry service care types:
- Residential Aged Care (RAC) services
- the Home Care Packages Program (HCPP)
- the Commonwealth Home Support Program (CHSP)
- the Multi-Purpose Services (MPS) Program
- the National Aboriginal and Torres Strait Islander Flexible Aged Care (NATSIFAC) Program.
Information was collected from in-scope active registered services which employed direct care staff (nurses, personal care workers or allied health staff) and had one or more eligible aged care clients during the reporting period. Services were asked to provide information relevant to the first fortnightly pay period in March 2023.
The sampling design involved 3,000 services who were invited to participate in the survey. Of those invited, 1,401 services provided submissions, giving an overall response rate of 47%. Importantly, weighting was used, so that the population estimates align with known population proportions. While this aims to reduce the impact of non-response bias, some unknown level of bias will remain, particularly for survey questions with a high proportion of non-response. Headcounts presented are weighted estimates. Headcount estimates may overstate the size of the workforce where staff work for multiple providers or across different service care types.
For more on the survey methods and data considerations, see the Data quality statement.
The baseline indicator value is based on the 2023 survey. For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 7.1 Increased training opportunities and resources about dementia available for the health, aged care, disability, and community services workforce 7.2 Increased number of primary care, acute, aged care, disability, and community service workers undertaking dementia specific training. This includes Aboriginal and Torres Strait Islander Health Workers and Health Practitioners 7.3 Increased capability of health, community services, disability and aged care sectors in working with people living with dementia |
Indicator | Proportion of aged care workers who completed dementia care training in the previous 12 months. |
Numerator | Weighted estimate of the number of aged care workers (headcounts) who completed dementia care training in the previous 12 months. |
Denominator | Weighted estimate of the total number of aged care workers (headcounts). |
Disaggregation | Job role, type of aged care service. |
Definitions | Job role: data were available for personal care workers, nurse practitioners, registered nurses and enrolled nurses. Type of aged care service: data were available for RAC, CHSP, HSCP, MPS and NATSIFAC services. |
Australian Institute of Health and Welfare (2024) 2023 Aged Care Provider Workforce Survey, AIHW, Australian Government, accessed 6 September 2024.
Carer Wellbeing Survey
Indicators measuring the needs, access to services, and wellbeing of carers of people living with dementia come from the Carer Wellbeing Survey (CWS). In the most recent year available (2024), 9,166 carers participated across Australia.
The CWS data used in this report were collected between February and April, 2024. The CWS was initiated and is managed by the WellRes Unit, University of Canberra and Carers Australia, and is funded by Australian Research Council (ARC) Industry Fellowship Grants, and by Department of Social Services funding provided through Carers Australia. The findings and views reported in this publication, however, are those of the AIHW and should not be attributed to either the funders or managers of the CWS. The CWS was approved by the University of Canberra Human Research Ethics Committee, protocol number HREC 1887.
Participants could complete the survey online or on a paper form, which was translated into simplified Chinese, Arabic, Italian and Vietnamese. In 2024, CWS recruited participants by: inviting previous survey participants; through care provider organisations (via client email lists); through carer representative organisations (including websites and social media channels), and through social media advertising (including some advertising in different languages the survey is available in). A prize draw was offered to encourage participation in the survey.
Methods used to collect data in the 2024 CWS are described further in the CWS User Guide (Mylek and Schirmer 2025), available at https://www.regionalwellbeing.org.au/carer-wellbeing-survey/
AIHW analysis of CWS data are reported as weighted percentages (Mylek and Schirmer 2025). To ensure reliability of comparisons presented, only percentages with a relative standard error of less than 25% are reported. Statistical significance (or non-significance) of differences in proportions between population groups has been calculated based on a two-proportion z-test using weighted proportions.
Remoteness area in the CWS uses the Australian Statistical Geography Standard (ASGS) Remoteness Structure. In this report ‘regional or remote’ incorporates the categories of Inner regional, Outer regional, Remote and Very remote.
The CWS asks about the gender respondents identify as, with response options ‘female’, ‘male’, ‘other (e.g. non-binary, gender-fluid, no gender)’ and ‘Prefer not to answer’. The survey does not ask about sex assigned at birth. Results in this report are only presented for male and female as counts for ‘other’ and ‘prefer not to answer’ were too low to report.
While other demographic information is collected in the CWS, these were not presented in the current report due to low counts and/or high relative standard errors.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 5.1 Improved coordination of care for people living with dementia |
Indicator | Proportion of carers of people living with dementia who reported that poor coordination of care was a moderate or large barrier to accessing services for the person they care for. |
Numerator | Carers of people living with dementia who reported that poor coordination of care was a moderate or large barrier to accessing services for the person they care for. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked to indicate to what extent each of a list of issues (for example, cost, transport, funding) ‘present barriers to or problems when trying to access services such as in-home support, respite care, cleaning services for the person or people you care for?’. For this reporting, respondents who rated ‘Poor coordination between different services accessed by the person/people you care for’ as 3-5 (moderate barrier) or 6-7 (large barrier) on a scale from 1 ‘NOT a problem’ to 7 ‘VERY BIG problem’ were included in the numerator. |
Measure | 5.2 People living with dementia and their carers find it easier to navigate the health, aged care and disability support systems to access the services and supports they need |
Indicators |
|
Numerators |
|
Denominators |
|
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked: ‘Have you received any assistance to help you navigate government systems such as NDIS, My Aged Care, Carer Gateway etc.?’ with the response options: ‘Yes, and it was helpful’; ‘Yes, but it wasn’t very helpful’; ‘No, I needed to access help but wasn’t able to access it’; ‘No, I didn’t need to access help’. Categories ‘Yes and it was helpful’ and ‘Yes, but it wasn’t very helpful’ were grouped to calculate the proportion of carers who received assistance navigating government services. To calculate the proportion who received services and reported it was helpful, the numerator included respondents who reported ‘Yes, and it was helpful’ while the denominator included both ‘Yes and it was helpful’ and ‘Yes, but it wasn’t very helpful’ response categories. |
Measure | 5.9 Improved advance care planning and palliative care for people living with dementia |
Indicator | Proportion of carers of people living with dementia who reported the person they care for has an Advance Care Plan. |
Numerator | Carers of people living with dementia who reported that the person they care for has an Advance Care Plan. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked to indicate ‘Yes’, ‘No’ or ‘Unsure’ to the question ‘Does the person you care for have an advance care plan?’. For this reporting, respondents who indicated ‘Yes’ were included in the numerator. |
Measure | 6.1 Increased carer awareness, access and satisfaction with dementia support services and resources |
Indicator | Proportion of carers of people living with dementia who connected with other carers to share experiences and advice in the past year. |
Numerator | Carers of people living with dementia who connected with other carers to share experiences and advice in the past year. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked to indicate whether they had accessed different types of supports as a carer. For this reporting, respondents who indicated yes to the question: ‘In the last 12 months, how satisfied were you with your access to different types of support as a carer?: Ability to connect to other carers to share experiences and advice.’ were included. |
Measure | 6.1 Increased carer awareness, access and satisfaction with dementia support services and resources |
Indicator | Proportion of carers of people living with dementia who had accessed carer training and skills courses in the past year. |
Numerator | Carers of people living with dementia who accessed carer training and skills courses in the last year. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked to indicate whether they had accessed different types of supports as a carer. For this reporting, respondents who indicated yes to the question: ‘In the last 12 months, how satisfied were you with your access to different types of support as a carer?: Access to carer training and skills courses.’ were included in the numerator. |
Measure | 6.3 Increased availability and use of respite services by people living with dementia |
Indicator | Proportion of carers of people living with dementia who had accessed respite care services in the past year. |
Numerator | Carers of people living with dementia who had accessed respite care services for the person they care for in the past year. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | Survey respondents were asked to indicate whether they had accessed different types of supports as a carer. For this reporting, respondents who indicated yes to the question: ‘In the last 12 months, how satisfied were you with your access to different types of support as a carer?: Access to respite care services.’ were included. |
Measure | 6.6 Improvements in self-reported wellbeing among dementia carers |
Indicator | Proportion of carers of people living with dementia who experienced high personal wellbeing. |
Numerator | Carers of people living with dementia who reported a high personal wellbeing score. |
Denominator | Carers of people living with dementia. Excludes individuals who did not respond to the survey item. |
Disaggregation | Gender, remoteness area. |
Definitions | For this reporting, Personal Wellbeing Index (PWI) was used. PWI is a commonly used measure of subjective personal wellbeing (International Wellbeing Group, 2013). A ‘high’ personal wellbeing score was defined as a mean score of 80 or higher on the PWI measure, while ‘typical’ wellbeing was defined as a mean score of 60-79. Respondents may have been missing up to 2 items and their response was imputed from the mean of the remaining items. |
International Wellbeing Group. 2013. Personal Wellbeing Index: 5th Edition. Melbourne: Australian Centre on Quality of Life, Deakin University.
Mylek and Schirmer, 2025. Carer Wellbeing Survey User guide, August 2025. University of Canberra, accessed 10 October 2025.
Dementia Australia
Indicators measuring the use of Dementia Australia services, and client satisfaction with services, come from Dementia Australia. Dementia Australia collect a limited range of data for the purposes of understanding their clientele, what groups in Australia seek or do not seek their supports, and for annual reporting and acquittals to their funders, including the Australian Department of Health, Disability and Ageing. Aggregated data was provided free of charge by Dementia Australia to the AIHW. The findings and views reported in this publication are those of the AIHW and should not be attributed to either Dementia Australia or their funders.
Data from Dementia Australia are reported as raw tallies or percentages. Readers are advised that Dementia Australia do not always collect data for enquirers calling the National Dementia Helpline, and that the data that is collected may be incomplete. This is due to the complexity of calls and/or level of distress of the client. This means that while it is important for governments to understand how many people from priority groups receive support from Dementia Australia, coding this information is not the main task or priority in a Dementia Australia National Dementia Helpline interaction. Indicators based on data from Dementia Australia are therefore indicative only. The Dementia Australia client survey is sent to program participants twice annually and data used in this report are from aggregated November 2023 and May 2024 surveys.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 1.2 Increased access to and understanding of supported decision making for all people living with dementia, including for First Nations, cultural and linguistically diverse (CALD), and other diverse communities |
Indicator | Number of contacts to the National Dementia Helpline who received a recommendation for external legal or financial advice. |
Disaggregation | None |
Definitions | Clients include people living with dementia or their carers or family who have contacted the National Dementia Helpline for support or information. There is currently no information on whether people received the recommended advice. |
Measure | 1.4 People in regional, rural and remote settings have improved access to dementia diagnosis and support |
Indicator | Number of people living in regional and remote areas who accessed Dementia Australia supports. |
Disaggregation | Gender, age group, remoteness. |
Definitions | This indicator is the number of people living in regional or remote areas who accessed the National Dementia Helpline, the National Dementia Support Program, the Commonwealth Home Support Program or other state-funded services through Dementia Australia in 2023–2024. Clients include people living with dementia or their carers or family. Remoteness data are based on participants postcodes. ‘Regional or remote’ includes Inner regional, Outer regional, Remote, and Very remote areas classified according to the Australian Statistical Geography Standard (ASGS) Remoteness Structure. |
Measure | 2.4 Increased number of dementia-friendly communities |
Indicator | Number of dementia-friendly communities registered with Dementia Australia. |
Disaggregation | None |
Definitions | This indicator defines dementia-friendly communities as the number of Dementia-Friendly Alliances and Dementia-Friendly organisations registered with Dementia Australia in 2023-24. |
Measure | 4.7 People living with dementia and their carers reporting a positive experience of diagnostic and post‑diagnostic care |
Indicator | Number of people who accessed post-diagnostic supports through Dementia Australia. |
Disaggregation | Gender, age group, remoteness area. |
Definitions | This indicator is the number of Dementia Australia clients who accessed the Post-Diagnostic Support Program, funded by the National Dementia Support Program, in 2023–24. Clients include people living with dementia or their carers or family. Remoteness data are based on participants postcodes. ‘Regional or remote’ includes Inner regional, Outer regional, Remote, and Very remote areas classified according to the Australian Statistical Geography Standard (ASGS) Remoteness Structure. |
Measure | 6.1 Increased carer awareness, access and satisfaction with dementia support services and resources |
Indicator | Number of family and carers who receive support through Dementia Australia. |
Disaggregation | Gender, age group, remoteness area, Indigenous status, CALD status |
Definitions | This indicator is the number of family and carers of people living with dementia who accessed the National Dementia Support Program, the Commonwealth Home Support Program or other state-funded services through Dementia Australia in 2023–24. Remoteness data are based on participant postcodes. ‘Regional or remote’ includes Inner regional, Outer regional, Remote, and Very remote areas classified according to the Australian Statistical Geography Standard (ASGS) Remoteness Structure. |
Dementia Awareness Survey
The Dementia Awareness Survey (DAS) was first run in 2023, surveying more than 5,400 Australian adults to understand general knowledge of dementia and dementia risk factors, and community attitudes towards dementia and people living with dementia in Australia.
The Australian Government Department of Health, Disability and Ageing commissioned the AIHW to manage the Dementia Awareness Survey, and the AIHW commissioned the Social Research Centre to conduct the survey fieldwork.
Significance testing: some Dementia Awareness Survey figures include 95% confidence intervals (CI): the range between the lower and upper 95% CI contains the true value of the percentage, with 95% confidence. These have not been adjusted for other demographic factors such as age, gender or remoteness, and differences between groups may not be present when adjustment has been made. The p value was used to determine if the difference between the reference group and other group/s was statistically significant. P values were calculated using a regression model that adjusted for other demographic factors, including age, gender and remoteness. A difference was deemed to be statistically significant if the chance of seeing the observed difference under the null hypothesis was less than 5% (p <0.05).
For more detailed data, including the counts used to calculate proportions, see the Supplementary data tables. Comprehensive technical notes detailing survey methodology, questionnaire design, sampling and weighting are available from the Dementia Awareness Survey technical notes.
Measure | 2.1 Reduced stigma and improved attitudes among Australians towards people living with dementia |
Indicator | Average dementia stigma scores among Australians (using the Dementia Public Stigma Scale). |
Disaggregation | Only those population groups with a statistically significant difference are shown in this dashboard: gender, country of birth, language spoken at home, sexual orientation, family or friend with dementia, worked with people living with dementia. Data on other population groups are available in the Dementia Awareness Survey (figures 4.1 and 4.2). |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 2.2 Improved knowledge among Australians about what dementia is and how it affects people living with dementia |
Indicator | Average dementia knowledge scores among Australians (using the Dementia Knowledge Assessment Scale). |
Disaggregation | Only those population groups with a statistically significant difference are shown: gender, country of birth, education level, annual household income, sexual orientation, family or friend with dementia, worked with people living with dementia, remoteness area. Data on other population groups are available in the Dementia Awareness Survey web report (figures 1.1 and 1.2). |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 2.3 Increased willingness of people to seek help if they thought they had symptoms of dementia and share their dementia diagnosis |
Indicator | Proportion of Australians willing to seek help if they thought they had symptoms of dementia. |
Disaggregation | None. |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 2.3 Increased willingness of people to seek help if they thought they had symptoms of dementia and share their dementia diagnosis |
Indicator | Proportion of Australians who would be willing to share their dementia diagnosis if they developed dementia. |
Disaggregation | Population groups are shown for the proportion of Australians who would be willing to share their dementia diagnosis with family members if they developed dementia: age group, gender, education level, family or friend with dementia, worked with people living with dementia, language spoken at home, country of birth, Indigenous status, sexual orientation, annual household income, and remoteness area. |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 3.1 Improved knowledge among the general population and communities at higher risk of developing dementia about risk factors for dementia |
Indicator | Average dementia risk knowledge score among Australians. |
Disaggregation | Only those population groups with a statistically significant difference are shown: gender, education level, sexual orientation, family or friend with dementia, worked with people living with dementia. Data on other population groups are available in the Dementia Awareness Survey (figures 2.1 and 2.2). |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 3.1 Improved knowledge among the general population and communities at higher risk of developing dementia about risk factors for dementia |
Indicator | Proportion of Australians who agree that information about reducing dementia risk is easily available. |
Disaggregation | Figure: Indigenous status. Supplementary tables: age group, gender, education level, family or friend with dementia, worked with people living with dementia, language spoken at home, country of birth, Indigenous status, sexual orientation, annual household income, and remoteness area. |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 3.3 Increased number of Australians taking steps to reduce their risk of developing dementia |
Indicator | Average number of actions Australians are taking out of a list of known actions that can reduce their dementia risk. |
Disaggregation | This indicator summarises findings from the Dementia Awareness Survey (Figure 3.1) by gender and age group. |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Measure | 3.3 Increased number of Australians taking steps to reduce their risk of developing dementia |
Indicator | Proportion of Australians who agree they are more likely to adopt a healthy lifestyle if it reduces dementia risk. |
Disaggregation | Age group, gender, education level, family or friend with dementia, worked with people living with dementia, language spoken at home, country of birth, Indigenous status, sexual orientation, annual household income, and remoteness area. |
Definitions | Comprehensive technical notes detailing survey methodology, questionnaire design, sampling, weighting and significance testing are available from the Dementia Awareness Survey technical notes. |
Australian Institute of Health and Welfare (2024) Dementia Awareness Survey, AIHW, Australian Government, accessed 7 October 2025.
Dementia Support Australia
Dementia Support Australia (DSA) represents a series of federally funded programs run by HammondCare that help formal and informal care givers support a person living with dementia.
Aggregated demographic data about DSA clients are used in this report. This means AIHW has not received any personal information about any people living with dementia or their carers who have been assisted by DSA. Aggregated data was provided free of charge by DSA to the AIHW. All numbers from DSA have been rounded to the nearest multiple of 5, 10 or 100.
The findings and views reported in this publication are those of the AIHW and should not be attributed to either DSA, HammondCare, or their funders.
Data were provided for services delivered from January 2019 to December 2024, with 2024 data used as the baseline indicator value.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 1.4 People in regional, rural and remote settings have improved access to dementia diagnosis and support. |
Indicator | Number of referrals received by Dementia Support Australia (DSA) for people living in regional and remote areas. |
Disaggregation | Year, gender, remoteness area, Indigenous status, cultural and linguistic diversity (CALD) status. |
Definitions | This indicator is the number of people living in regional and remote areas who were participants in the Dementia Behaviour Management Advisory Service (DBMAS), Severe Behaviour Response Teams (SBRT) program, or Needs Based Assessment (NBA) program. Remoteness is classified according to the Australian Statistical Geography Standard (ASGS) Remoteness Structure. Data on Indigenous status and CALD status do not include information on Not stated or missing records. |
Measure | 4.8 More people living with younger onset dementia and children with dementia are accessing and satisfied with diagnostic and post-diagnostic services and supports, including through disability services |
Indicator | Number of people living with younger onset dementia referred to Dementia Support Australia (DSA). |
Disaggregation | Year, age group, sex or gender, Indigenous status, CALD status. |
Definitions | This indicator is the number of people living with younger onset dementia who were participants in the DBMAS, SBRT program, or Needs Based Assessment program. DSA defines younger onset dementia as clients who were aged under 65 upon first referral to DSA. Data are provided for the age groups: 0–49, 50–54, 55–59 and 60–64 years. As the data may include children, the term ‘sex or gender’ is used. Remoteness is classified according to the Australian Statistical Geography Standard (ASGS) Remoteness Structure. Data on Indigenous status and CALD status do not include information on Not stated or missing records. |
Dementia Training Australia
These data come from Dementia Training Australia (DTA). DTA is a consortium funded by the Australian Government to provide education and training on the care of people living with dementia, across Australia.
It is important to note that DTA is a major provider, but is not the only provider, of dementia-specific training. Data from other organisations are not currently available.
The indicator reports the number of occasions of dementia training completed through DTA in 2024: if a person completed more than one course during a period, they would be counted more than once. The indicator is presented as a raw number because there are currently no suitable denominator data that represent the total number in the target population.
Data on breakdowns by different population groups are currently only available for people who completed an online DTA course in 2024, whereas the baseline indicator value includes people who completed any DTA course (whether online and face-to-face). DTA has advised the AIHW that the demographic profiles are likely to be similar.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 7.1 Increased training opportunities and resources about dementia available for the health, aged care, disability, and community services workforce 7.2 Increased number of primary care, acute, aged care, disability, and community service workers undertaking dementia specific training. This includes Aboriginal and Torres Strait Islander Health Workers and Health Practitioners 7.3 Increased capability of health, community services, disability and aged care sectors in working with people living with dementia |
Indicator | Number of occasions of dementia training completed through Dementia Training Australia. |
Disaggregation | Gender, age group, type of care setting, remoteness area. |
Definitions | Remoteness is classified according to the Modified Monash Model (MMM). MMM classification for remoteness was based on postcode. |
National Carer Survey
The National Carer Survey (NCS) is a survey of carers in Australia run every two years by Carers NSW with the support of the state and territory carer organisations. In the most recent year available (2024), 10,096 carers were surveyed across Australia. The survey is funded by the NSW Department of Communities and Justice.
Aggregated data from the NCS were provided free of charge by Carers NSW to the AIHW. All indicators use the 2024 survey data for baseline values. The AIHW calculated 95% confidence intervals around the proportion. Statistical significance (or non-significance) of differences in proportions between population groups has been calculated based on a two-proportion z-test.
While various demographic information is collected in the NCS, those with low counts and/or high relative standard errors are not presented in this report.
Remoteness area in the NCS uses the Australian Statistical Geography Standard (ASGS) Remoteness Structure. In this report ‘regional or remote’ incorporates the categories of Inner regional, Outer regional, Remote and Very remote.
While the NCS may under-represent carers who are not well connected with carer organisations and supports, it still provides important insights into the experiences of carers of people living with dementia.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 5.2 People living with dementia and their carers find it easier to navigate the health, aged care and disability support systems to access the services and supports they need |
Indicators | Proportion of carers of people living with dementia who found it difficult to find information about:
|
Numerators | Carers of people living with dementia who found it difficult to find information about:
|
Denominator | Current carers of people living with dementia. |
Disaggregation | Gender, remoteness area |
Definitions | Survey respondents were asked to tick all that apply from a list of challenges experienced with ‘NDIS or other disability services’, and the same list for challenges experienced with aged care services. Respondents who ticked ‘It was difficult to find information about what services were available and how to access them’ were included in the numerator. |
Measure | 5.2 People living with dementia and their carers find it easier to navigate the health, aged care and disability support systems to access the services and supports they need |
Indicators | Proportion of carers of people living with dementia who were not provided with all the information they needed from:
|
Numerators | Carers of people living with dementia who were not provided with all the information they needed from:
|
Denominator | Current carers of people living with dementia. |
Disaggregation | Gender, remoteness area |
Definitions | Survey respondents were asked to indicate their agreement with the statements ‘When I accompanied the person I care or cared for to visit a GP I was provided with all the information I needed’ and 'When I accompanied the person I care for on a visit to the hospital or community health service I was provided with all the information I needed' on a 5-point scale ‘Strongly agree to ‘Strongly disagree’ (or ‘Not applicable’). For this reporting, respondents who responded ‘agree’ or ‘strongly agree’ were included in the numerators. |
Measure | 6.6 Improvements in self-reported wellbeing among dementia carers |
Indicator | Proportion of carers of people living with dementia who were socially connected. |
Numerator | Carers of people living with dementia who were socially connected. |
Denominator | Current carers of people living with dementia. |
Disaggregation | Year, gender, remoteness area |
Definitions | Social connectedness was measured using the Hawthorne Friendship Scale (Hawthorne 2000). This scale provides a measure of overall social connectedness and social isolation. Scores can be categorised into 5 levels, from ‘highly socially isolated’ to ‘highly socially connected’. For this indicator, carers who reported being ‘socially connected’ or ‘highly socially connected’ were included in the numerator. |
Hawthorne G and Griffith P (2000). The friendship scale: Development and properties. West Heidelberg, Victoria, Australia: Centre for Health Program Evaluation.
National Centre for Vocational Education Research (NCVER)
The National Centre for Vocational Education Research (NCVER) produces a range of data on Australia’s Vocational Education and Training (VET) system (delivered via both public and private providers) including students, participation, courses and qualifications. Data on students and courses are supplied from the National VET Provider Collection.
Data are collected annually for all training activity and quarterly for government-funded training. The latest year of data available is 2024. Time trends include data from 2020 to 2024.
For this report, the AIHW used NCVER’s publicly available DataBuilder to extract the number of people who completed a vocational training subject about dementia as part of their VET course.
Numbers are rounded to the nearest 5. Caution should be taken when using data with a 'not known' response. Data are reported as 'not known' for several reasons, including information was not collected or invalid. Data exclude students with an offshore training delivery location.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measures | 7.1 Increased training opportunities and resources about dementia available for the health, aged care, disability, and community services workforce 7.2 Increased number of primary care, acute, aged care, disability, and community service workers undertaking dementia specific training. This includes Aboriginal and Torres Strait Islander Health Workers and Health Practitioners 7.3 Increased capability of health, community services, disability and aged care sectors in working with people living with dementia |
Indicator | Number of students who completed a vocational training subject about dementia. |
Disaggregation | Student attributes: gender, age group, Indigenous status, remoteness region, socioeconomic area (SEIFA IRSD), country of birth, language other than English spoken at home. Program attributes: Program name. Subject attributes: Funding source. |
Definitions | All data had the following filters applied:
Additional filters were applied for each disaggregation for the year 2024, as listed above. Total numbers were extracted for the years 2020, 2021, 2022, 2023 and 2024. Gender categories: male, female, other, not known Age categories: 15-19, 20-24, 25-29, 30-39, 40-49, 50-59, 60-64, 65+, Not known Indigenous status categories: First Nations, Non-Indigenous, Not known. Country of birth data are only shown for the countries with the 6 highest values and Not known / inadequately described. Language other than English spoken at home categories: Yes, No, Not known. Remoteness area is based on the Australian Statistical Geography Standard (ASGS) Remoteness Structure. An offshore residence is where students are enrolled in Australia but have provided an overseas residential address. Socioeconomic area is based on the Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-Economic Disadvantage (IRSD). All program names (diploma or certificate) were included. |
National Disability Insurance Scheme (NDIS)
These data come from AIHW analysis of National Disability Insurance Scheme (NDIS) data in the Person Level Integrated Data Asset (PLIDA) in the Australian Bureau of Statistics’ DataLab.
Data included in this report were based on data extracts available in PLIDA at the time of analysis (August 2025), so there may be differences in the numbers published in this report and other reports.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
For more information on PLIDA, see Australian Bureau of Statistics (ABS) – Data assets.
Measure | 4.8 More people living with younger onset dementia and children with dementia are accessing and satisfied with diagnostic and post-diagnostic services and supports, including through disability services |
Indicator | Number of approved National Disability Insurance Scheme (NDIS) plans for people living with younger onset dementia. |
Disaggregation | Year (by quarter), gender, age group, Indigenous status, culturally and linguistically diverse (CALD) status, accommodation type (supported independent living at Plan Effective Date and living in residential aged care), and remoteness area. |
Definitions | Younger onset dementia was based on the ‘ICD classification of primary disability’, using the following ICD-10-AM codes: F00 Alzheimer’s, F03 Unspecified dementia, F03.9 Dementia- Rapidly progressing, G30.0 Dementia – Early onset, G31.0 Frontotemporal, G31.83 Neurocognitive disorder with Lewy Bodies. The cohort was limited to people whose age at first approval of their NDIS plan was between 30 and 64 years. Gender categories: Male, Female, Not defined/ No answer/Unknown (aggregated). Age groups: 30–49, 50–54, 55–59, 60–64, 65–69, 70 and over. Indigenous status: First Nations, Non-Indigenous, Not asked/Not stated/Not defined (aggregated). CALD status: Yes, No, Not stated Living in Residential Aged Care: Yes, No Living in Supported Independent Living: Yes, No, Missing Remoteness area is classified according to the Modified Monash Model (MMM), with Very remote areas grouped together with those with a missing remoteness area. |
National Health Data Hub (NHDH)
The National Health Data Hub (NHDH 2021–22) is a longitudinal, person-focused and de-identified health linkage system that comprises data from state and territory, Commonwealth and non-government data sources.
The NHDH is the only linked asset that brings together hospital data on admitted patient care services, emergency department services and outpatient services for all public (and where available, private) hospitals in New South Wales, Victoria, Queensland, South Australia, Tasmania and the Australian Capital Territory. The NHDH also contains datasets relating to pharmaceuticals, health service use, aged care, deaths, disability, intensive care and immunisation information. As of August 2025, it covered data spanning from 1 January 1997 to 30 June 2024, though temporal scope varied by dataset.
Dementia Identification Criteria:
A person was identified as having dementia if they had at least one of the following in NHDH at least 5 years prior to or during the financial year of interest:
- A dementia-specific medication dispensed through the PBS/ RPBS.
- A principal or additional diagnosis of dementia in an emergency department (ED) presentation or hospital admission.
- A supplementary chronic condition code of dementia in a hospital admission.
- A record of dementia in datasets from the National Aged Care Data Clearinghouse (NACDC) including the Aged Care Assessment Program (ACAP) and National Screening Assessment Form (NSAF).
A person could also be identified with dementia if it was recorded as an underlying or additional cause of death during or 6 months after the financial year of interest (Figure T1).
The study cohort was also restricted to people who had at least one Medicare Benefits Schedule (MBS) record during the financial year of interest and to people who did not have missing age information.
Methodological approach to tracking indicators:
Only records from ‘continuous’ datasets were used, that is, datasets that are unlikely to conclude or that have known replacements capable of identifying people with dementia (Figure T2). This supports more robust comparisons in changes of the indicator over time and helps determine whether they signal progress.
A moving lookback window and the use of continuous datasets ensures that observed changes in indicators over time are less likely to reflect inconsistent inclusion criteria over time for the cohort. This method also allows focus on use of services over time for people with dementia, without the need to compare to a non-dementia group at each time point, reducing complexity and the potential for variability or noise to affect observed trends.
Figure T1: Data collection periods by year of interest
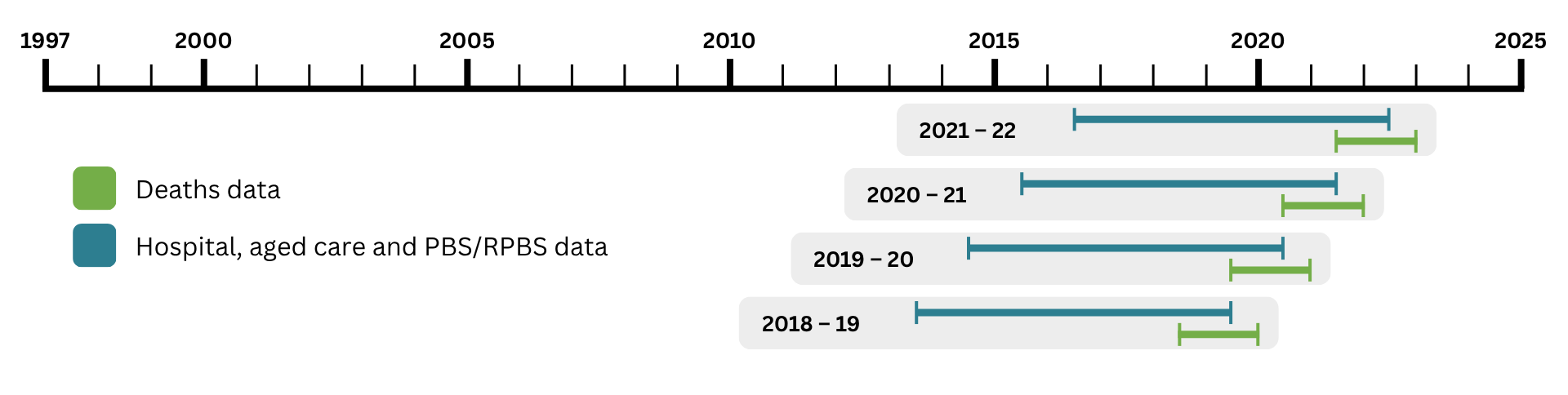
* PBS/ RPBS – Pharmaceutical Benefits Scheme and Repatriation Pharmaceutical Benefits Scheme
Figure T2: Datasets used to identify people with dementia
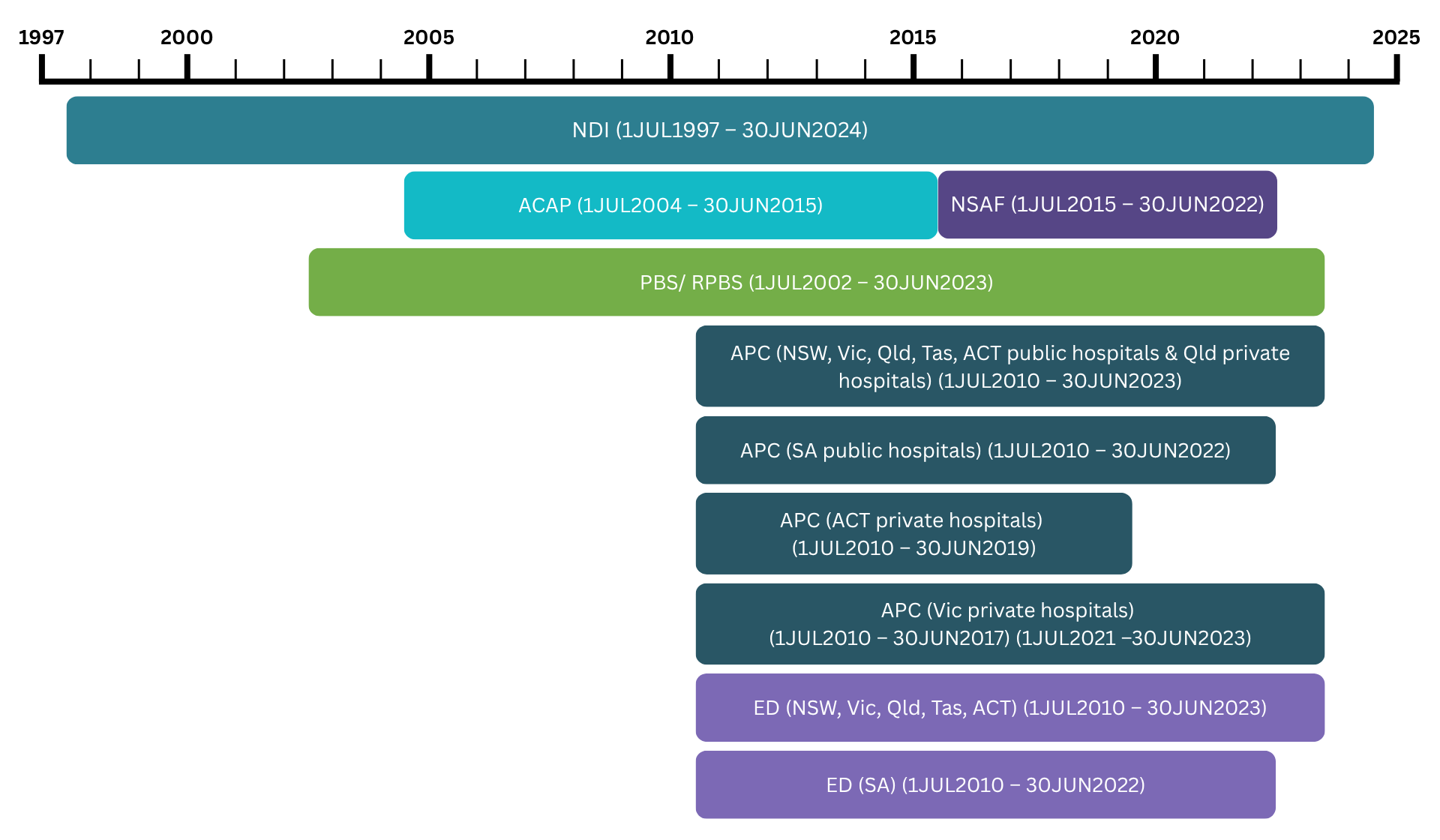
* Private hospital data for the ACT and Victoria includes some but not all private hospitals.
** Includes complete census of licensed private hospitals in Queensland. This includes private psychiatric hospitals.
*** On July 1, 2015, supplementary codes for chronic conditions were implemented in admitted patient care data.
NDI – National Death Index; ACAP – Aged Care Assessment Program; NSAF – National Screening Assessment Form; PBS/ RPBS – Pharmaceutical Benefits Scheme and Repatriation Pharmaceutical Benefits Scheme; APC – Admitted Patient Care; ED – Emergency Department.
Dataset | Reason for exclusion |
Aged Care Funding Instrument (ACFI) | Coverage spans from March 20, 2008, to 30 June 2022. As the ACFI will not be available in future years to identify people with dementia, this dataset was excluded to ensure a consistent approach for flagging dementia cases across all years. This exclusion also increases confidence that any observed changes in service use are not influenced by differences in the characteristics of individuals who were previously identified solely through the ACFI. |
Home care dementia and cognition supplement | People with cognitive impairment associated with conditions other than dementia are eligible for the supplement. Program ends on 30 June 2025. |
Medicare Benefits Schedule (MBS) (Item number 61560) | Item alone does not confirm a dementia diagnosis. |
It should be borne in mind when exploring the results of this report that NHDH data may not be representative of all people living with dementia across Australia, with some people not accessing services offered by the included NHDH data sources.
Table T12 outlines the codes used in each individual dataset to identify dementia and the classification system used in each dataset.
Data source | Classification and dementia-specific codes |
Admitted patient care | ICD-10-AM diagnosis codes: F00, F01, F02, F03, F05.1, F10.7, F13.7, F18.7, G30 Chronic condition supplementary code U791 |
Emergency department presentations | ICD-10-AM diagnosis codes: F00, F01, F02, F03, F05.1, F10.7, F13.7, F18.7, G30, U791 ICD-9-CM diagnosis codes: 290.0, 290.1, 290.10, 290.11, 290.12, 290.13, 290.2, 290.20, 290.21, 290.3, 290.4, 290.40, 290.41, 290.42, 290.43, 290.8, 290.9, 291.2, 294.1, 294.10, 294.11, 294.2, 294.20, 294.21, 331.0 SNOMED CT-AU EDRS diagnosis codes: 52448006, 12348006, 15662003, 26929004, 191461002 |
Pharmaceutical Benefits Scheme | Anatomical Therapeutic Chemical Classification codes: N06DA02 (donepezil), N06DA03 (rivastigmine), N06DA04 (galantamine), N06DX01 (memantine) |
Aged Care Assessment Program | Aged Care Assessment Program minimum dataset (MDS) version 2.0: 0500–0532, 0542, 0584 |
National Screening Assessment Form | Aged Care Assessment Program minimum dataset (MDS) version 2.0: 0500–0532, 0542, 0584 |
National Death Index | ICD-10 Underlying or associated cause of death codes: F00, F01, F02, F03, F05.1, F10.7, F13.7, F18.7, G30, G31.0, G31.8 |
Note: ICD-10 refers to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. ICD-10-AM refers to ICD-10, Australian Modification. ICD-9-CM refers to the ICD, Ninth Revision, Clinical Modification. SNOMED CT-AU EDRS refers to the Systemized Nomenclature of Medicine – Clinical Terms – Australian version (Emergency Department Reference Set).
The Medicare Benefits Schedule (MBS) data collection contains claims data for Medicare services subsidised by the Australian Government. These services include GP Chronic Disease Management Plans and medication management reviews.
People may receive these services in ways that are not captured in MBS data, including services delivered under Department of Veterans’ Affairs arrangements; services provided through hospitals; services provided under a state-funded service; and services provided by a salaried GP or any other salaried medical officer arrangement (AIHW 2024).
Chronic Disease Management Plans and Medication management reviews were identified according to the MBS codes in table T13.
Terminology used in this study | MBS code |
|---|---|
GP plan | BTOS: 0102 and Subgroup: A15.1, A40.13, A40.14 or Items: 229–233, 93469, 93475 |
Medication management review | BTOS: 0102 and Items: 245, 249, 900, 903 |
Note: BTOS = Broad Type of Service.
Although some datasets spanned until the end of the 2023–24 financial year at the time of analysis, NSAF data were only available from 1 July 2015 to 30 June 2022. To ensure a consistent lookback period for identifying people with dementia across financial years, the most recent year of reporting was 2021–22.
Respite care refers to residential respite care and is determined from admission information for residential aged care services. Other types of respite care such as respite care at home, flexible respite care, community and centre-based respite care or cottage respite care are not included. Transitions of care after accessing a residential respite service were only reported among people who exited residential respite care during the first 9 months of 2021–22. This allowed a 3-month window to look at place of residency since data were only available up to 30 June 2022. Transitions are reported once per person, based on their first episode of residential respite care during this period.
Socioeconomic and remoteness area information for a person with dementia was determined by the most recent MBS record during the financial year of interest. Where the most recent MBS record did not have socioeconomic and remoteness area information, the next most recent record with this information was used.
Age was calculated at the start of the financial year of interest, assuming a birth date on the 15th of their birth month, as birth information in the data only include month and year.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
For more information on the NHDH, see National Health Data Hub.
Measure | 4.6 Increased number of people living with dementia with a Chronic Disease Management Plan in place with their GP |
Indicator | Proportion of the NHDH dementia cohort who had a Chronic Disease Management Plan attendance. |
Numerator | Number of people with dementia who had a Chronic Disease Management Plan attendance during the financial year of interest. |
Denominator | Number of people with dementia during the financial year of interest. |
Disaggregation | Sex, age groups, place of residence, remoteness area, socioeconomic area. |
Definitions | People living in residential aged care refers to those who had a permanent residential aged care episode during the financial year of interest. Anyone who did not have a permanent residential aged care episode was referred to as ‘living in the community’. Remoteness data is based on a person’s postcode. Remoteness categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Remoteness Structure. Socioeconomic data is calculated from the patient postcode. Socioeconomic categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Socio-Economic Indexes for Areas (SEIFA) – Index of Relative Socio-economic Disadvantage (IRSD). |
Measure | 5.5 Increased number of people living with dementia with regular medication reviews |
Indicator | Proportion of the NHDH dementia cohort who had a medication management review. |
Numerator | Number of people with dementia who had a medication management review during the financial year of interest. |
Denominator | Number of people with dementia during the financial year of interest. |
Disaggregation | Sex, age groups, place of residence, remoteness area, socioeconomic area. |
Definitions | People living in residential aged care refers to those who had a permanent residential aged care episode during the financial year of interest. Anyone who did not have a permanent residential aged care episode was referred to as living in the community. Remoteness data is calculated from the patient postcode. Remoteness categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Remoteness Structure. Socioeconomic data is calculated from the patient postcode. Socioeconomic categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Socio-Economic Indexes for Areas (SEIFA) – Index of Relative Socio-economic Disadvantage (IRSD). |
Measure | 6.3 Increased availability and use of respite services by people living with dementia |
Indicator | Proportion of the NHDH dementia cohort who accessed respite care services. |
Numerator | Number of people with dementia who accessed residential respite care services during the financial year of interest. |
Denominator | Number of people with dementia during the financial year of interest. |
Disaggregation | Sex, age groups, place of residence, remoteness area, socioeconomic area, transitions of care. Note: Transitions of care after accessing a residential respite service were only reported among people who exited residential respite care during the first 9 months of 2021–22. This allowed for a 3-month window to look at place of residence since data was only available up to 30 June 2022. |
Definitions | Residential respite care service use is determined from admission information for residential aged care services. People living in residential aged care were defined as those who had a permanent residential aged care episode either the day before, 7 days after, or 3 months following a residential respite care episode. At each of these time points, individuals who were not in permanent residential aged care, residential respite care, or deceased were classified as living in the community. Remoteness data is calculated from the patient postcode. Remoteness categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Remoteness Structure. Socioeconomic data is calculated from the patient postcode. Socioeconomic categories are classified according to the Australian Statistical Geography Standard (ASGS) 2016 Socio-Economic Indexes for Areas (SEIFA) – Index of Relative Socio-economic Disadvantage (IRSD). |
AIHW (Australian Institute of Health and Welfare) (2024) Dementia in Australia, AIHW, Australian Government, accessed 29 July 2025.
AIHW (Australian Institute of Health and Welfare) (2021–22) National Health Data Hub, aihw.gov.au, accessed 5 August 2025.
Palliative Care Outcomes Collaboration (PCOC)
The Palliative Care Outcomes Collaboration (PCOC) is a national palliative care outcomes quality improvement program. The program uses standardised validated clinical assessment tools to benchmark and measure outcomes in palliative care, including pain and symptom control, and timely access to services when they are needed to drive quality improvements. The PCOC data collection includes patient demographics, clinical setting information, and patient outcomes collected via 5 assessment tools (PCOC 2012).
Participation in PCOC is voluntary and open to all palliative care service providers across all Australian States and Territories. Representation is sought from public and private health sectors, rural and metropolitan areas, and inpatient and community settings. However, not all services participate in PCOC and so the data only capture a subset of all palliative care delivered in Australia. A total of 228 services reported data to PCOC in 2024, and work is ongoing to expand this number. Most services that report data to PCOC are specialist palliative care services. For more information about PCOC data including its coverage, see the PCOC Data Quality Statement.
National data on people accessing palliative care outside specialist settings are needed to complement PCOC data. For more information about palliative care data, including a strategic plan to improve national information on palliative care and end-of-life care, see Palliative care services in Australia.
Data for all indicators are for the 2024 calendar year. For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables and PCOC’s National Outcomes reports.
Measure | 5.9 Improved advanced care planning and palliative care for people living with dementia |
Indicator | Proportion of palliative care phases for people with dementia, for which distress related to pain improved or remained at a low level after intervention. |
Numerator | Number of palliative care phases ending within the reference year with a valid Symptom Assessment Scale (SAS) for ‘Distress from Pain’ at phase start and end, and for which SAS ‘Distress from Pain’ improved or remained absent/mild. |
Denominator | Number of palliative care phases ending within the reference year with a valid SAS for ‘Distress from Pain’ at phase start and end, in people with dementia (includes Alzheimer’s dementia and Other Dementia) who received a service from a palliative care service provider participating in PCOC. |
Disaggregation | Alzheimer’s dementia, Other dementia. |
Definitions | Dementia diagnosis: There are 31 PCOC diagnostic groups. The population captured in the above indicators includes those whose principal life-limiting illness responsible for the patient requiring palliative care, was coded as Alzheimer’s dementia (206) or Other Dementia (207). Phase type: A clinically meaningful period in a patient’s condition. The palliative care phase is determined by a holistic clinical assessment, which considers the needs of the patients and their family and carers. The 5 palliative care phases are stable, unstable, deteriorating, terminal and bereavement. A patient may move back and forth between phases (except bereavement). Severity at phase start: Severity of distress related to 7 key symptoms recorded via the SAS tool, and/or severity of problems assessed via the Palliative Care Problem Severity Score (PCPSS) at phase start. The 4 severity categories are: Absent, Mild, Moderate, Severe. Symptom Assessment Scale (SAS): a patient (or proxy) rated tool that assesses the level of distress using a numerical rating scale from 0 – no distress to 10 – worst possible distress for 7 key symptoms (insomnia, appetite problems, nausea, bowel problems, breathing problems, fatigue, and pain). Only SAS ‘Distress from Pain’ was used in analyses. SAS are grouped according to the categories: absent (0), mild (1-3), moderate (4-7) and severe (8-10) (Daveson et al. 2021). All phases without a valid start and end SAS for ‘Distress from Pain’ were excluded. SAS assessments are not performed at death. Most terminal phases end in death. A small number of PCOC services do not collect SAS data. |
Measure | 5.9 Improved advanced care planning and palliative care for people living with dementia |
Indicator | Proportion of palliative care phases for people with dementia, for which family or carer problems improved or remained at a low level after intervention. |
Numerator | Number of palliative care phases ending within the reference year with a valid PCPSS for ‘Family/Carer’ problems at phase start and end, and for which the PCPSS for ‘Family/Carer’ problems improved or remained absent/mild. |
Denominator | Number of palliative care phases ending within the reference year with a valid PCPSS for ‘Family/Carer’ problems at phase start and end, in people with dementia (includes Alzheimer’s dementia and Other Dementia) who received a service from a palliative care service provider participating in PCOC. |
Disaggregation | Alzheimer’s dementia, Other dementia. |
Definitions | Dementia diagnosis: There are 31 PCOC diagnostic groups. The population captured in the above indicators includes those whose principal life-limiting illness responsible for the patient requiring palliative care, was coded as Alzheimer’s dementia (206) or Other Dementia (207). Phase type: A clinically meaningful period in a patient’s condition. The palliative care phase is determined by a holistic clinical assessment, which considers the needs of the patients and their family and carers. The 5 palliative care phases are stable, unstable, deteriorating, terminal and bereavement. A patient may move back and forth between phases (except bereavement). Severity at phase start: Severity of distress related to 7 key symptoms recorded via the SAS tool, and/or severity of problems assessed via the PCPSS at phase start. The 4 severity categories are: Absent, Mild, Moderate, Severe. Palliative Care Problem Severity Score (PCPSS): a clinician rated screening tool to assess the overall severity of problems within four key palliative care domains. This includes family/carer problems associated with a patient's condition or palliative care needs. Written, verbal, or observational information may be used by the clinician to assess severity. The scores are 0 – absent, 1 – mild, 2 – moderate and 3 – severe (Masso et al. 2016). A symptom is considered to have improved over the phase if there was at least a one-point change between phase start and end. All phases without a valid start and end PCPSS for ‘Family/Carer’ problems were excluded. PCPSS assessments are not performed at death. |
Daveson BA, Allingham SF, Clapham S, Johnson CE, Currow DC, Yates P and Eagar K (2021) ‘The PCOC Symptom Assessment Scale (SAS): A valid measure for daily use at point of care and in palliative care programs’, PLoS ONE, 16(3): e0247250, doi.org/10.1371/journal.pone.0247250
Masso M, Allingham SF, Johnson CE, Pidgeon T, Yates P, Currow D and Eagar K (2016) ‘Palliative Care Problem Severity Score: Reliability and acceptability in a national study’, Palliative Medicine, 30(5):479-85, doi:10.1177/0269216315613904.
Palliative Care Outcomes Collaboration (PCOC) (2012) PCOC Version 3.0 Dataset Data Dictionary and Technical Guidelines, PCOC, accessed 7 October 2025.
Data relating to Australian research on dementia
Research studies including lived experience of dementia
Guidelines relating specifically to dementia related research were sourced from the National Health and Medical Research Council (NHMRC) dementia research webpage and current grants from GrantConnect. Annual Dementia, Ageing and Aged Care Grant Opportunity Guidelines under the Medical Research Future Fund – Dementia, Ageing and Aged Care Mission are reviewed for updated lived experience requirements and assessment criteria that promote lived experience.
Other guidelines and policies were reviewed from the NHMRC and ARC websites, including:
- Australian Code for the Responsible Conduct of Research 2018
- The National Statement on Ethical Conduct in Human Research (2023) (effective as of 1 Jan 2024).
- Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: Guidelines for researchers and stakeholders
- AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander Research (the AIATSIS code)
- Culturally and Linguistically Diverse (CALD) Dementia Research Action Plan
- Strategic Roadmap for Dementia Research and Translation
- The Statement on Consumer and Community Involvement in Health and Medical Research.
Guidelines and dementia grants were searched for the requirement of lived experience across all areas of research, and was considered met if that requirement was explicitly stated. For example, the Code of Ethics for Aboriginal and Torres Strait Islander Research (AIATSIS) has explicitly stated that those with lived experience should be consulted on all stages of the research process:
“It is important that research with Aboriginal and Torres Strait Islander people and communities is led by Aboriginal and Torres Strait Islander people and communities. This can mean that the chief researchers and/or members of the research team are Aboriginal or Torres Strait Islander people. It can also mean that research and its priorities are driven and guided by the Aboriginal and Torres Strait Islander communities with whom the research will take place.”
“The Guidelines should inform all steps in the research process including conception (the initial idea), design (planning the research), conduct (ways of doing the research), reporting (what happened), and dissemination of findings (circulation to relevant bodies).”
This can be compared to the Culturally and Linguistically Diverse (CALD) Dementia Research Action Plan specifications under “Guiding principles for CALD-inclusive dementia research” which present more general guidelines regarding lived experience:
“Research should include co-design and partnership approaches that involve CALD communities and other stakeholders over the life-span of the study.”
“Researchers should work to develop and support partnerships between the health sector, care providers, training organisations, ageing and ethnic peak-bodies, and CALD communities to ensure rapid translation of evidence into practice.”
It is worth noting that having consumers and community members actively involved in the research does not necessarily mean that people with lived experience of dementia were included in the research, and this is a limitation of the current approach to assessing progress against this measure.
The 2024 Dementia, Ageing and Aged Care Grant Opportunity Guidelines for both the Targeted Call for Research and Incubator grants require lived experience involvement in their assessment criterion and reward the following demonstrations of lived experience involvement with maximal scores:
Assessment Criterion 1 – Project Impact
- “comprehensively and convincingly considers the needs, priorities, views and values of consumers (particularly those with lived experience and their carers), the community, health providers and/or other end users”
Assessment Criterion 2 – Project Methodology
- “clearly and comprehensively articulates extensive involvement and contributions of consumers throughout the research journey
- "where relevant, demonstrates comprehensive leadership and involvement of priority population(s) that the research is intended to benefit”
Assessment Criterion 3 – Capacity, capability and resources to deliver the project
- “has comprehensively and convincingly demonstrated it has the skills, experience and capacity to involve and support consumers appropriately and effectively”
Consumers are defined as a person with lived experience as a patient, client, potential patient, user of health services, and/or provider of support as a carer, family or community member.
Data related to research publications in Australia
A search was performed for peer-reviewed published articles on PubMed. PubMed is a free resource from the United States National Library of Medicine that supports the search and retrieval of biomedical and life sciences literature. It has over 30 million citations from journals selected for MEDLINE and PubMed Central.
A search strategy was tested and refined following feedback from experts. A compromise was made between a comprehensive review to include all Australian dementia publications of interest, and a search that did not have a high level of false positives. This approach may not have identified all relevant articles. Details of the resulting search terms can be found in the table below.
The baseline indicators value is based on the 2024 calendar year, but data from the start of the 2020 calendar year were used when discussing changes over time. The baseline and future updates reflect the year of electronic publication. Electronic publication (Epub) dates are more relevant than print publication dates as Epub dates reflect the availability of the most recent research articles.
For more detailed data, see the Supplementary data tables.
Measure | 8.2 Increased number of high quality, peer reviewed, open access Australian dementia studies. |
Indicators |
|
Source for data | |
Filters applied | ("dementia"[MeSH Terms] OR "alzheimer disease"[MeSH Terms] OR "alzheimer*"[Title/Abstract] OR "picks disease"[Title/Abstract] OR "pick disease"[Title/Abstract] OR "pick’s disease"[Title/Abstract] OR "primary progressive aphasia*"[Title/Abstract] OR "CADASIL"[Title/Abstract] OR "cerebral autosomal dominant arteriopathy with subcortical infarcts"[Title/Abstract] OR "CARASIL"[Title/Abstract] OR "cerebral autosomal recessive arteriopathy with subcortical infarcts"[Title/Abstract] OR "leukoencephalopathy"[Title/Abstract] OR "creutzfeldt jakob*"[Title/Abstract] OR "cjd"[Title/Abstract] OR "frontotemporal lobar degenerat*"[Title/Abstract] OR "huntington*"[Title/Abstract] OR "kluver bucy"[Title/Abstract] OR "primary progressive nonfluent aphasia"[Title/Abstract] OR "sundown syndrome"[Title/Abstract] OR "sundowning"[Title/Abstract] OR "korsakoff syndrome"[Title/Abstract] OR "binswanger*"[Title/Abstract] OR "Lewy body*"[Title/Abstract] OR "Lewy bodies*"[Title/Abstract] OR "hiv associated neurocognitive disorder*"[Title/Abstract]) AND ("australia*"[Title/Abstract] OR "australia*"[Grants and Funding] OR "australia*"[MeSH Terms] OR "National Health and Medical Research Council" OR "NHMRC" OR "Dementia Australia Research" OR "Australian Research Council" OR "Australian Government" OR (Australia*[Affiliation]) NOT (review[Publication Type])) AND (YYYYYYYY [Electronic Publication Date]) Electronic publication (Epub) dates were used as most articles are accessed online and this provides the broadest coverage of combined online and print and solely online journals. To calculate the baseline value for number of open access Australian dementia publications, the above search terms were used with the annual year changes to the year of interest and checking that the subset that had “free full text” availability to obtain those with open access. |
Data related to research grants in Australia
The search results of research grants include a spectrum of grants that range from those narrowly focused on dementia research to those that are more distantly able to inform dementia research. In order not to exclude funded grants that were indirectly supporting dementia research, we considered that any mention of dementia (or the alternate search terms used below) in the published summaries was an indicator that it could contribute to the body of knowledge of dementia in Australia.
For some funding, such as from the Australian Research Council (ARC), the amount of funding announced, and the actual funding provided may be different. To compare across funding streams, the funding announced was used, noting that the actual funding provided is often higher for ARC funding.
The announcement year or grant start year (if announcement year wasn’t available) of successful grants were analysed from publicly available data from the NHMRC, ARC and Medical Research Future Fund (MRFF) grant outcome websites.
It is worth noting that the majority of NHMRC and ARC funding is not directed to any specific disease and therefore there is no process in place within these funding bodies which might guarantee an increase in dementia funding over the coming years, so the indicator on the proportion of research dedicated to dementia is largely reflective of proposals put forward by researchers, rather than funding available strictly for dementia.
The ARC funding reported in the Action Plan does not include funding for ARC Centres of Excellence, such as the ARC Centre of Excellence in Population Ageing Research, unless their public descriptions specify one of the specified dementia search terms. This may underestimate dementia research if centres incorporate elements of dementia research in a broader research activity.
The baseline values of indicators are based on the 2024 calendar year, but data from the start of the 2014 calendar year were used when discussing changes over time.
For more detailed data, including the counts used to calculate proportions for relevant indicators, see the Supplementary data tables.
Measure | 8.3 Increased number and value of dementia research grants approved |
Indicator |
|
Source for grants data | NHMRC - data sourced via their website, with the search carried out on Title, Standard Descriptors, and Media Summary. MRFF – data sourced via their website, with the search carried out on Project Name and Project Summary. ARC – data sourced via their website, with the search carried out on Grant Summary and National Interest Test Statement. |
Search terms | A key-word search was performed by announcement year for dementia research grants across all 3 websites (NHMRC, ARC, and MRFF): dementia*; Alzheimer*; pick disease; pick’s disease; Niemann-Pick; primary progressive aphasia*; CADASIL*; cerebral autosomal dominant arteriopathy with subcortical infarcts*; CARASIL*; cerebral autosomal recessive arteriopathy with subcortical infarcts; leukoencephalopathy; creutzfeldt*; frontotemporal lobar degenerat*" OR "huntington*; kluver bucy; primary progressive nonfluent aphasia; sundown syndrome*; sundowner syndrome; sundowning*; korsakoff syndrome; binswanger*; "Lewy body*; Lewy bodies*; or hiv associated neurocognitive disorder. If any of the search terms appeared in the search, then this was counted in the number and the value of dementia grants for that year, by funding organisation. |