Specialist homelessness services client pathways: analysis insights:
Specialist homelessness services client pathways: Rough sleeping clients in 2016–18
Web article
Last updated:
Topic: Homelessness services
Citation
AIHW (Australian Institute of Health and Welfare) (2024) Specialist homelessness services client pathways: Rough sleeping clients in 2016–18, AIHW, Australian Government, accessed 9 July 2026.
This article is part of Specialist homelessness services client pathways: analysis insights
Children and young people
- Specialist homelessness services client pathways: Children on care and protection orders in 2014–17
- Specialist homelessness services client pathways: Young clients aged 18 to 24 in 2018–20
- Specialist homelessness services client pathways: Young clients aged under 18 in 2011–13
- Specialist homelessness services client pathways: Young clients presenting alone in 2015–16
Client vulnerabilities
- Specialist homelessness services client pathways: Clients exiting custodial arrangements in 2014–17
- Specialist homelessness services client pathways: Clients with mental health issues in 2015–16
- Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16
Indigenous Australians
Specialist homelessness services clients
Family, domestic and sexual violence
- Specialist homelessness services client pathways: Female clients experiencing family and domestic violence and persistent homelessness in 2020–21
- Specialist homelessness services client pathways: Female clients experiencing family and domestic violence and returning to homelessness in 2020–21
- Specialist homelessness services client pathways: Female clients with family and domestic violence experience in 2015–16
Client housing situation
- Specialist homelessness services client pathways: Rough sleeping clients in 2016–18 This page
Introduction
Rough sleeping clients are a highly visible subset of homeless people, often with complex needs and as such are a particularly vulnerable group. Around 43,000 (or 16% of all SHS clients) SHS clients were sleeping rough at some point during their contact with SHS agencies in 2022–23 (see Clients rough sleeping).
Longitudinal analyses have been undertaken for a cohort of rough-sleeping SHS clients aged 16 and over who commenced a period of support with an SHS agency in 2016–18.
Rough sleeping clients are defined as clients who, either the week before, at the time of presenting to an SHS agency, or at the end of their support period with an SHS agency, had no shelter or who were living in non-conventional accommodation, including:
- living on the streets
- sleeping in parks
- squatting
- staying in cars or railway carriages
- living in improvised dwellings or
- living in the long grass.
See Introduction to the SHS longitudinal data for details on the longitudinal analyses.
A comparison homeless non-rough sleeping cohort was defined as clients who were homeless either the week before, at the time of presentation, or at the end of a support period with an SHS agency, but who were not rough sleeping clients in any of their support periods in 2016–18. In contrast to clients rough sleeping, clients in the comparison cohort experienced secondary homelessness, which typically involves short-term or emergency accommodation including:
- refuges
- crisis shelters
- couch surfing or no tenure
- living temporarily with friends and relatives
- insecure accommodation on a short-term basis
- emergency accommodation arranged by a specialist homelessness agency (for example, in hotels, motels and so forth).
The longitudinal SHS data for the period 2014–22 were used to examine characteristics and service use patterns of rough sleeping clients compared with the comparison cohort (the non-rough sleeping cohort) (Figure RS.1).
These analyses are limited to people receiving SHS support.
The retrospective study period for this cohort is the 24 months before the start of the defining study period (which is the 24 months from the start of their first support period in 2016–18). The prospective study period is the 24 months after the end of each client’s 24 month defining study period.
Key findings
- In 2016–18, 61% of SHS clients experiencing rough sleeping were male and 92% presented for support alone.
- Half of the rough sleeping cohort had received SHS support in the previous 2 years, and over one-third received support in the following 2 years.
- Rough sleeping clients had more periods of SHS support than homeless non-rough sleeping clients and were around twice as likely to need counselling for drug or alcohol problems, or for problem gambling.
- Rough sleeping SHS clients who were transitioning from custody or who had mental health or problematic drug or alcohol issues in the defining period were more likely to need future SHS support.
Figure RS.1: Rough sleeping cohort 2016–18, longitudinal analysis overview

Source: AIHW analysis of SHS longitudinal data 2014–22, Table Rough1618.1.
Key characteristics of the rough sleeping cohort
Half of the rough sleeping cohort received SHS support in the previous 2 years, and over one-third received support in the following 2 years.
Over half (54%) of the rough sleeping cohort had a current mental health issue in the defining period.
There were over 52,200 clients in the rough sleeping cohort in 2016–18; these clients had the following key characteristics (Figure RS.2, Table Rough1618.1, Table Rough1618.2):
- Over half (53%, 27,700) were aged 25 to 44 years and 61% were male.
- Over 14,000 clients (27%) were Indigenous Australians.
- Around 16% (8,200 clients) presented for support with children sometime in the defining study period (that is, they received SHS support sometime in 2016–18 and had one or more children with them at the time of receiving any of the periods of support). Over 92% (48,100 clients) presented for support alone at some time.
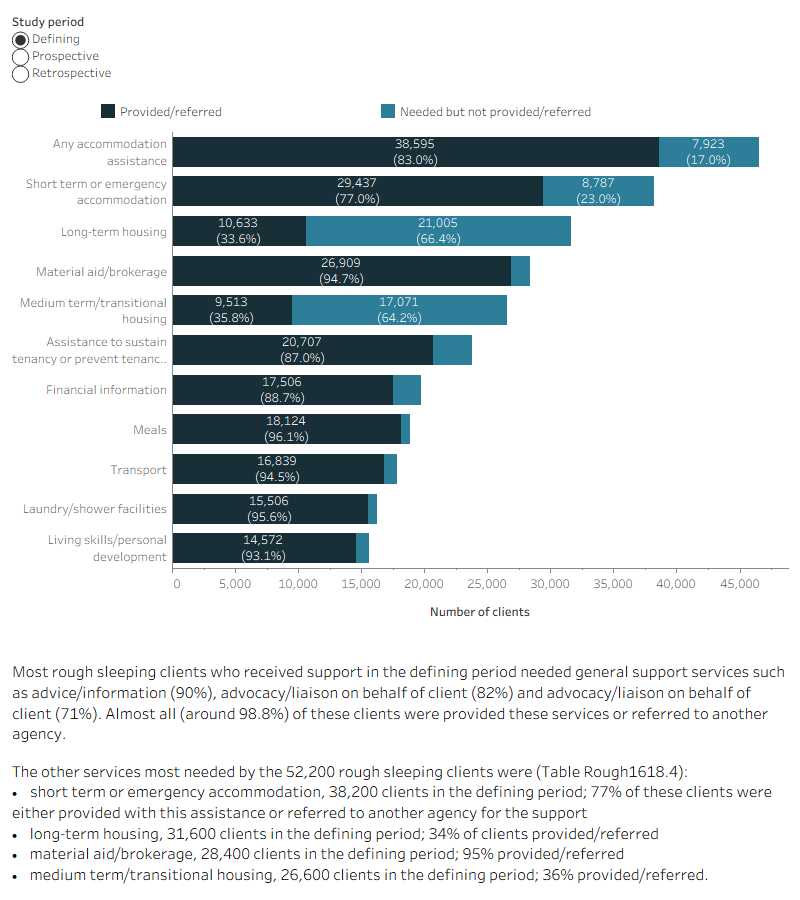
- Three quarters (73% or 38,200 clients) needed short-term accommodation in the defining period, and 65% (25,100) of those received that type of accommodation.
- Over 1 in 3 clients (17,400 clients, 33%) had one support period during the defining study period and 47% (24,400 clients) had three or more support periods.
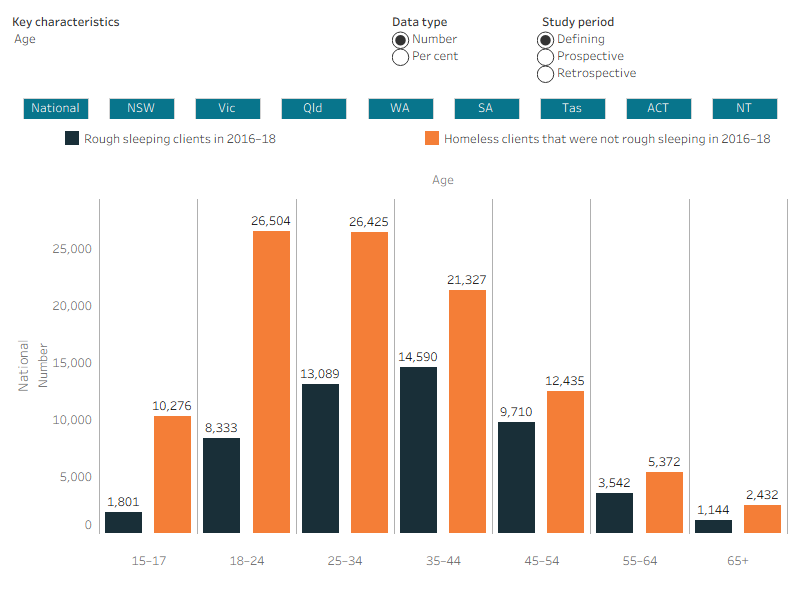
Figure RS.2: Rough sleeping and non-rough sleeping cohorts 2016–18, client key characteristics, by study period
This interactive bar chart shows a comparison between the rough sleeping and non rough-sleeping cohorts, in terms of key characteristics and across all study periods (defining, retrospective and prospective). A radio button allows selection for the individual state/territory and Australia. For Australia, rough sleeping clients were more likely to be aged 35–44 (rough sleeping clients 28% compared with 20% non rough-sleeping clients), have had drug/alcohol issues (29% compared with 15%), had mental health issues (54% compared with 44%). They were less likely to have one support period (33% compared with 47%) and more likely to have three or more support period (47% compared with 31%). Rough sleeping clients were also more likely to receive accommodation (of any type) (52% compared with 40%).
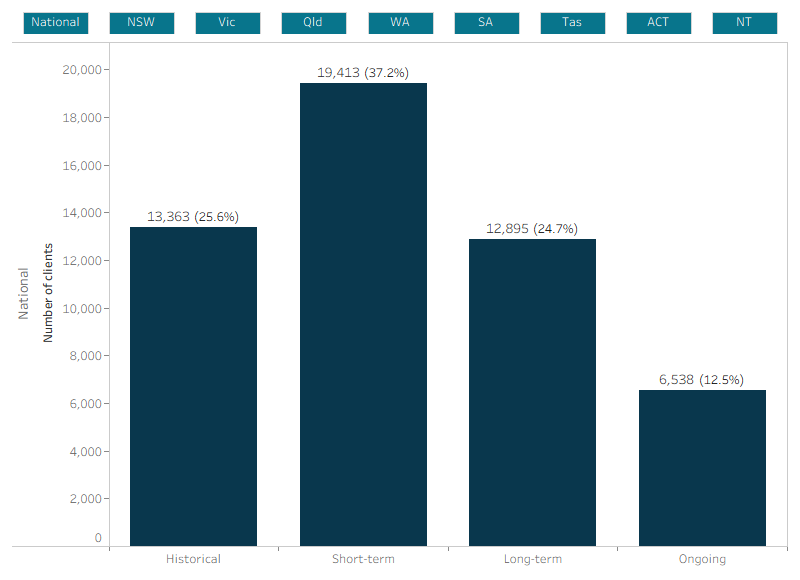
This interactive bar chart shows service use patterns of the 2016–18 rough sleeping cohort over the 2014–22 longitudinal period. Support information was combined from the discrete study periods into four service engagement profile groups (historical, short-term, long-term and ongoing). Engagement profiles for all states and territories and Australia can be selected and displayed. Nationally, of the 52,200 clients that made up the defining period cohort, 19,400 (37%) were short-term clients who only received support during the 24-month defining study period and 12,900 (25%) were long-term clients and had received support in all three study periods.
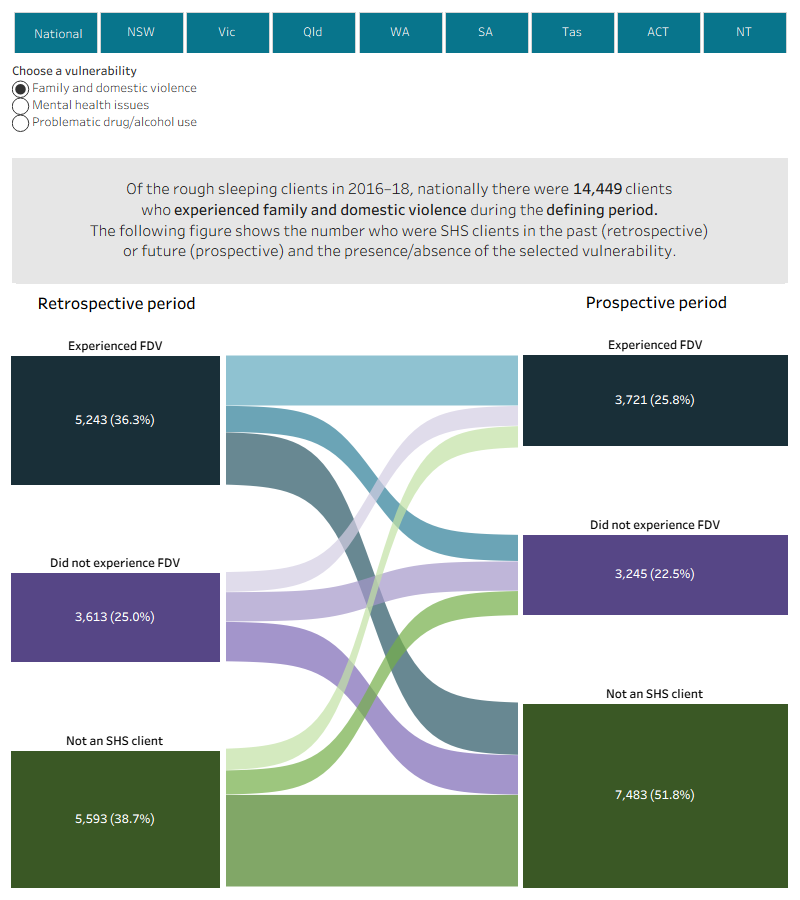
This interactive Sankey diagram shows the 2016–18 rough sleeping clients who experienced three vulnerabilities, clients who had experienced FDV, clients with a mental health issue and those with problems with drugs or alcohol in the defining study period and whether clients also experienced these vulnerabilities in the past and future study periods. These vulnerability pathways are shown separately, using radio buttons to select between vulnerability types. Using data for the entire longitudinal period, SHS rough sleeping clients were assessed for the presence of these vulnerabilities within each of the three study periods – the retrospective, defining and prospective periods. Vulnerability data and pathways for all states and territories and Australia can be selected and displayed. Most clients at the national level experienced the vulnerability in the defining study period and were not SHS clients in the retrospective and prospective study periods. For clients who had problematic drug/alcohol use in the defining period (15,400 clients), 14% did not have problematic use in the retrospective period and were not clients in the prospective period.
The interactive stacked horizontal bar graph shows the select top 10 services needed and the provision/referral status for the 2016–18 rough sleeping cohort (52,200 clients) who received support in each study period. Across all study periods, short term or emergency accommodation was one of the most needed services, around 77% of these clients were either provided this service or referred to another agency. Long-term housing was also needed but only provided or referred to 34% of clients. Material aid/brokerage was also a key service needed by this cohort; this service was provided/referred to 95% of clients.
The interactive risk ratio plot shows the differences in service need and reasons for seeking assistance between rough sleeping and homeless non rough-sleeping clients receiving SHS support in each study period, these associations are presented as relative risks. The top services and reasons more likely to be selected by rough sleeping cohort clients compared with non rough-sleeping clients (that is, those with the largest relative risk) have been shown in the figure. A radio button allows selection of the services or reasons for assistance for each of the study periods (defining, retrospective and prospective). Rough sleeping clients were 2 times more likely to need drug/alcohol counselling (relative risk [RR] 1.99) and 3 times more likely to select itinerant as a reason for seeking assistance (relative risk [RR] 3.35) than clients in the non rough-sleeping cohort during the 2016–18 defining study period.
![The interactive risk ratio plot shows the differences in service need and reasons for seeking assistance between rough sleeping and homeless non rough-sleeping clients receiving SHS support in each study period, these associations are presented as relative risks. The top services and reasons more likely to be selected by rough sleeping cohort clients compared with non rough-sleeping clients (that is, those with the largest relative risk) have been shown in the figure. A radio button allows selection of the services or reasons for assistance for each of the study periods (defining, retrospective and prospective). Rough sleeping clients were 2 times more likely to need drug/alcohol counselling (relative risk [RR] 1.99) and 3 times more likely to select itinerant as a reason for seeking assistance (relative risk [RR] 3.35) than clients in the non rough-sleeping cohort during the 2016–18 defining study period.](https://viz.aihw.gov.au:443/t/Public/views/ROUGH_1618/Figure_6RelativeRisk-Cohort.png?%3aembed=y&%3ashowVizHome=no&%3adisplay_spinner=no&%3ahost_url=https%3a%2f%2fviz.aihw.gov.au)
The interactive risk ratio plot shows the differences in the characteristics or reasons for presenting between the rough sleeping and non rough-sleeping cohorts, these associations are presented as relative risks. Relative risks for Australia are displayed. The regression model contains client characteristics and as well as reasons for seeking support in the defining study period. The model also examines associations between reasons and sex. The figure shows that rough sleeping clients were more likely to have inadequate or inappropriate dwelling conditions as a reason for seeking support (relative risk [RR] 1.58), being itinerant as a reason (RR 1.43), or having owned a home (RR 1.27).
Much less likely than non rough-sleeping clients to be female (relative risk is 0.55) or present with child(ren) (RR 0.72).
![The interactive risk ratio plot shows the differences in the characteristics or reasons for presenting between the rough sleeping and non rough-sleeping cohorts, these associations are presented as relative risks. Relative risks for Australia are displayed. The regression model contains client characteristics and as well as reasons for seeking support in the defining study period. The model also examines associations between reasons and sex. The figure shows that rough sleeping clients were more likely to have inadequate or inappropriate dwelling conditions as a reason for seeking support (relative risk [RR] 1.58), being itinerant as a reason (RR 1.43), or having owned a home (RR 1.27).Much less likely than non rough-sleeping clients to be female (relative risk is 0.55) or present with child(ren) (RR 0.72).](https://viz.aihw.gov.au:443/t/Public/views/ROUGH_1618/Figure_7RiskRatio-Sex.png?%3aembed=y&%3ashowVizHome=no&%3adisplay_spinner=no&%3ahost_url=https%3a%2f%2fviz.aihw.gov.au)
The interactive risk ratio plot shows the characteristics or reasons for presenting that are associated with rough sleeping clients’ need for SHS support in the past (retrospective) or future (prospective period), these associations are presented as relative risks. Relative risks for all states and territories and Australia can be selected and displayed (where there was sufficient sample size). Two regression models can be selected, Model 1 contains client characteristics and experiences in the defining period, Model 2 contains client characteristics and the reasons for seeking support in the defining study period. For both past and future SHS support the associations were similar. Nationally, being unemployed or not in the labour force during the defining study period had the strongest association (107% greater likely) with past or future SHS support. Other significant associations include transitioning from custody (40% more likely), having mental health or problematic drug or alcohol issues (35% and 32% more likely respectively), and being Indigenous (37% greater likelihood).
For Model 2, rough sleeping clients who indicated the reasons, housing crisis (25% greater) and financial difficulties (22%) were particularly associated with ongoing SHS support.
