Data source: National Perinatal Mortality Data Collection
The National Perinatal Mortality Data Collection (NPMDC) is a collection of data regarding the deaths of babies in hospitals and in the community, and includes all neonatal deaths and stillbirths of a baby at least 20 weeks’ gestation or at least 400 grams birthweight, during pregnancy, birth or within 28 days of birth. Perinatal deaths (stillbirths and neonatal deaths) include deaths following a termination of pregnancy.
The NPMDC commenced with the 2013 birth cohort and builds on information collected in the NPDC. Common identifier fields in the NPDC and NPMDC allow demographic information regarding perinatal death records in the NPMDC to be retrieved from the NPDC for reporting.
There are 33 data items collected in the NPMDC. Of these, 8 form the Perinatal Mortality National Best Endeavours Dataset (PM NBEDS), a program of national perinatal data development that involves the revision of existing NPMDC items to ensure they are nationally standard. The PM NBEDS program has been undertaken to improve data provision and reporting. The remaining 25 data items are voluntary items.
The data are supplied by state and territory health authorities using a standard de-identified extract to the AIHW on an annual basis. Data specifications supplied to jurisdictions for collection are included in the related data tables.
Detailed information on completeness, accuracy, and other aspects of data quality for the NPMDC, including information on the PM NBEDS, is available in the data quality statement.
National Maternal and Perinatal Mortality Clinical Expert Group
The National Maternal and Perinatal Mortality Clinical Expert Group (NMPMCEG) provides expert clinical advice regarding all components of the National Maternal and Perinatal Mortality Data Collections.
Data timeliness
Data for the NPMDC are provided to the AIHW annually. The data for a calendar year cannot be finalised until all jurisdictional mortality review committee reports that apply to that period are complete. Jurisdictions coordinate and facilitate data collection procedures from service providers and the updating of records.
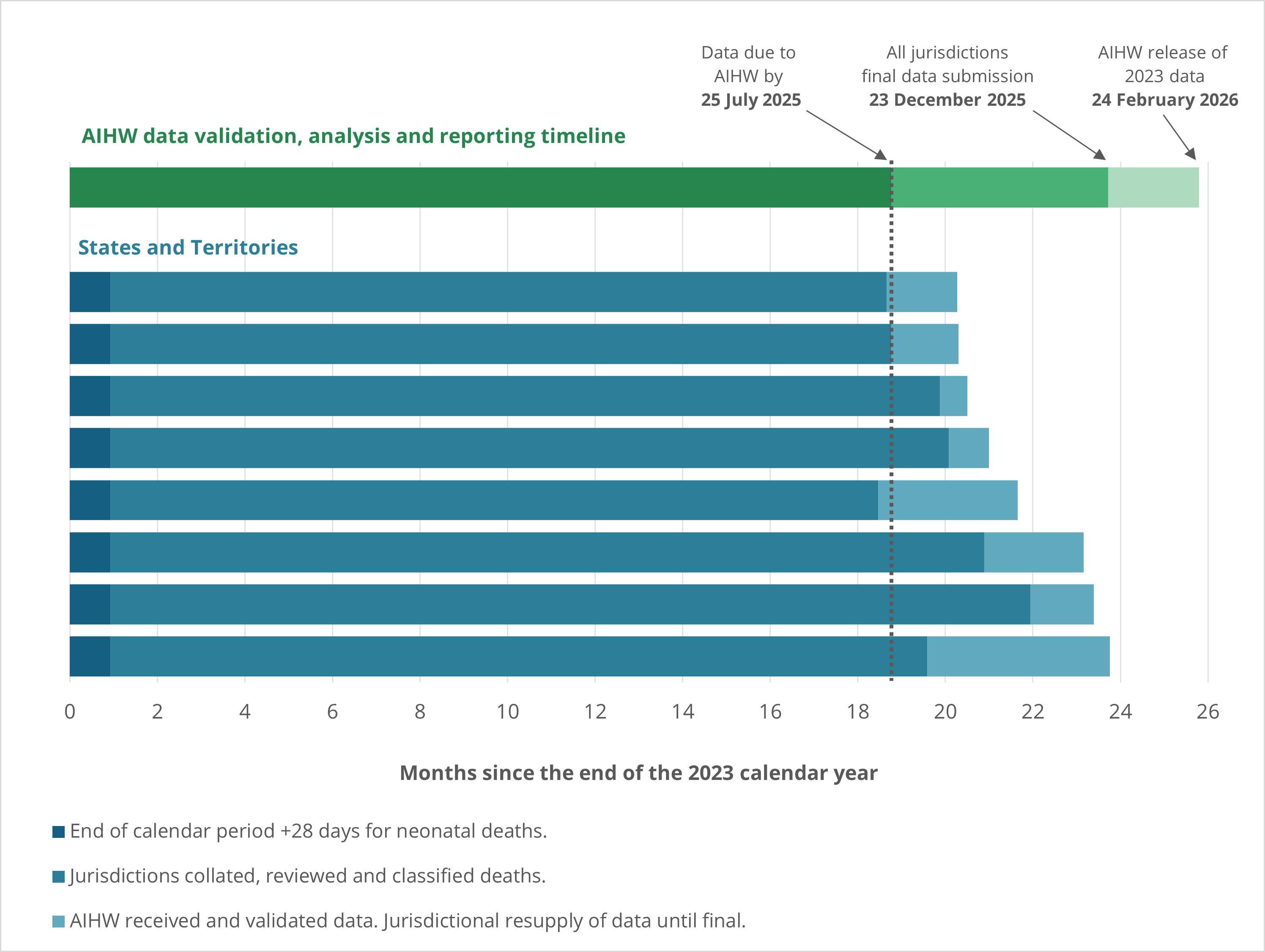
NPMDC data for 2023 were requested from states and territories on 23 June 2025 for submission to the AIHW by 25 July 2025. Data from 3 jurisdictions were received by this date. Data suppliers in some jurisdictions have given feedback that a request for data 17 months after the end of the collection period is unachievable as some data (particularly pertaining to PSANZ classification codes and contributory factors) take longer than 17 months to finalise.
Timelines for reporting 2023 data on perinatal deaths are outlined in Figure 1. The NPMDC data for 2023 were reported 25 months after the end of the collection period.
Figure 1: Months since the end of the 2023 calendar period and public reporting of data from the National Perinatal Mortality Data Collection, by state and territory
Data availability
Information on completeness for data items in the NPMDC is available, at the national level, in the interactive data visualisation below (Figure 2) for 2013 to 2023.
Definitions for the terms used to quantify completeness:
Supplied: supplied an appropriate value for a proportion of records for the data item during specified collection year/s.
Not supplied or not stated: proportion of values supplied as not stated or missing, where a jurisdiction has either supplied appropriate values for a portion of records or did not supply any value for all records for the data item during the specified collection year/s.
Figure 2: Availability of data in the National Perinatal Mortality Data Collection
The data visualisation shows a bar chart of the availability of data items in the National Perinatal Mortality Data Collection for the period 2013 to 2023

Preliminary data on perinatal deaths
Preliminary data on perinatal deaths are available from the National Perinatal Data Collection (NPDC). The AIHW established the separate, enduring National Perinatal Mortality Data Collection (NPMDC) to obtain complete information on these deaths.
Data on stillbirths and neonatal deaths are provided to the NPDC by jurisdictions as a subset of the larger cohort of all babies born in the same collection period. These preliminary data on stillbirths and neonatal deaths are made available to the public approximately 18 months after the end of the collection period.
Because these data are often supplied to the AIHW prior to completion of all Jurisdictional Mortality Review Committee reports, the data are not as comprehensive as those supplied to the NPMDC, particularly pertaining to PSANZ classification regarding the cause of death and contributory factors.
These preliminary data may also not include neonatal deaths for babies transferred to another hospital, re-admitted to hospital after discharge or who died at home after discharge.
Data provided to the NPMDC may vary from the preliminary data reported by the NPDC due to a variety of factors. Such factors include the inclusion of babies transferred to another hospital, re-admitted to hospital after discharge or who died at home after discharge; or cases where not enough detail was able to be provided by the jurisdiction to enable linkage of a particular death in the NPMDC back to the corresponding record in the NPDC.
Reporting Indigenous status
Indigenous status is a measure of whether a person identifies as being of Aboriginal and/or Torres Strait Islander origin. Unless otherwise stated, data for babies are based on the Indigenous status of the mother. However, the outcomes of babies of First Nations women remain a key data resource for assessing provision of antenatal care in pregnancy and other interventions before or during pregnancy.
Comparing NPMDC data with Victorian Consultative Council on Obstetric and Paediatric Mortality and Morbidity data
The Victorian stillbirth data reported by the AIHW have historically differed to data reported by the Victorian Consultative Council on Obstetric and Paediatric Mortality and Morbidity (CCOPMM). In previous years, including for births in 2022, CCOPMM applied the following exclusions to stillbirth reporting:
- Stillbirths at 20 or more weeks’ gestation but where the birthweight was less than 150 grams
- Stillbirths at 20 weeks’ gestation or more but where a fetal death in utero was diagnosed before 20 weeks (e.g. fetal death in utero (FDIU) diagnosed by ultrasound at 19 weeks’ gestation, but where birth occurred at or after 20 weeks’ gestation)
- Stillbirths resulting from termination of pregnancy for psychosocial indications.
For births from 2023 and onwards, for the purposes of better aligning to national reporting by the AIHW, CCOPMM reduced exclusions and reported all stillbirths of at least 20 weeks’ gestation, or of at least 400 grams birthweight if gestation was unknown, excluding only terminations for psychosocial indications. This definition of stillbirth is different to that used by the AIHW for reporting, which is all stillbirths where babies are of at least 20 weeks’ gestation, or at least 400 grams birthweight regardless of gestational age.
In 2023, the AIHW reported 702 stillbirths for Victoria at a rate of 9.5 per 1000 births. CCOPMM reported the same unadjusted stillbirth rate and also reported:
- An adjusted stillbirth rate of 7.4 per 1000 births (549 adjusted stillbirths) excluding terminations of pregnancy for psychosocial indications
- An adjusted stillbirth rate of 5.1 per 1000 births excluding terminations of pregnancy for psychosocial indications and for congenital anomalies.
Comparing NPMDC data with the Queensland Perinatal Data Collection
The data reported from the Queensland Perinatal Data Collection (QPDC) have historically differed from the data reported by the AIHW from the NPDC and NPMDC. These differences are due to differences in the scopes of the three collections, and affect the numbers of total births and perinatal deaths that are collected and reported.
The NPDC collates information on all births in Australia, including births in hospitals, birth centres, and the community, where the baby is at least 20 weeks’ gestation or birthweight is at least 400 grams. The NPMDC builds on information collected in the NPDC and collects data on all neonatal deaths and stillbirths where the baby is at least 20 weeks’ gestation or at least 400 grams birthweight. The NPMDC collects information on stillbirths occurring during pregnancy or birth, and on neonatal deaths occurring within 28 completed days of birth (i.e. 28 twenty-four-hour periods from time of birth).
This is different to the scope of the QPDC, which includes all live births regardless of the baby’s gestational age or birthweight. The QPDC also collects information on neonatal deaths occurring up to and including the 28th day after birth. This expanded scope results in the QPDC collecting and reporting a higher number of births and perinatal deaths than the NPDC and NPMDC.
Comparing NPMDC data with ABS registrations of death data
Perinatal death data reported by the Australian Bureau of Statistics (ABS) are not directly comparable with the NPMDC and NPDC data contained in this report. Differences in the number of perinatal deaths reported by the ABS and NPMDC can be seen in Table 1. For example, the number of stillbirths based on the NPMDC is consistently and notably higher than reported by the ABS.
While the definitions of stillbirth (referred to as fetal death in ABS reporting) and neonatal death are the same as the NPMDC, the data sources differ. ABS data are largely sourced from state and territory registrars of Births, Deaths and Marriages. For 2024 data, the ABS expanded the scope of their perinatal deaths data collection to include Medical Certificates of Cause of Perinatal Death (MCCPDs) as the primary source of data for Victorian stillbirths, improving the quality and accessibility of their perinatal death statistics. The expanded scope was used to revise data back to 2020 for Victoria. Data from the NPMDC and NPDC contained in this report are sourced from midwives, and other staff, who collect information from mothers and perinatal administrative and clinical record systems. Moreover, ABS data are reported by the year in which the death was registered with the state or territory registry. This excludes stillbirth data for Victoria from 2020, for which data are reported by the year the MCCPD data was received. See the ABS’ Perinatal deaths methodology for more detail. NPMDC data are reported by the year in which the birth occurred.
It is the responsibility of the parents to register a birth with Births, Deaths and Marriages, however some perinatal deaths may not be recorded when notifications are not registered by the parents. A delay in registrations is often seen, particularly for stillbirths, with the date of death often being many years prior to the date of registration. This means the accuracy of the number of perinatal deaths reported by the ABS for a particular year often improves over time.
Year | NPMDC Stillbirths | ABS Stillbirths | NPMDC Neonatal deaths | ABS Neonatal deaths |
|---|---|---|---|---|
2014 | 2225 | 1727 | 796 | 743 |
2015 | 2149 | 1727 | 688 | 694 |
2016 | 2114 | 1668 | 751 | 704 |
2017 | 2174 | 1726 | 800 | 763 |
2018 | 2116 | 1600 | 718 | 706 |
2019 | 2183 | 1656 | 714 | 700 |
2020(a) | 2273 | 2063 | 731 | 706 |
2021(a) | 2278 | 1999 | 738 | 745 |
2022(a) | 2380 | 2044 | 696 | 695 |
| 2023(a) | 2491 | 2035 | 687 | 660 |
(a) The scope of the ABS' perinatal deaths collection was expanded to include Medical Certificates of Cause of Perinatal Death (MCCPDs) as the primary source of data for Victorian stillbirths from 2020–2024. Care should be taken when comparing the number of stillbirths over time.
Note: ABS stillbirths and neonatal deaths are reported by the year in which the death was registered. For Victorian stillbirths from 2020 onwards, data are presented by year of receipt (ABS 2025, Perinatal deaths).
For more information on perinatal deaths data collected by the ABS, visit the perinatal deaths page at the Australian Bureau of Statistics.
Definitions used in reporting perinatal deaths
Various definitions are used for reporting and registering perinatal deaths in Australia. The National Perinatal Mortality Data Collection (NPMDC) collects data and reports using the following definitions:
Figure 3: Definitions of perinatal death
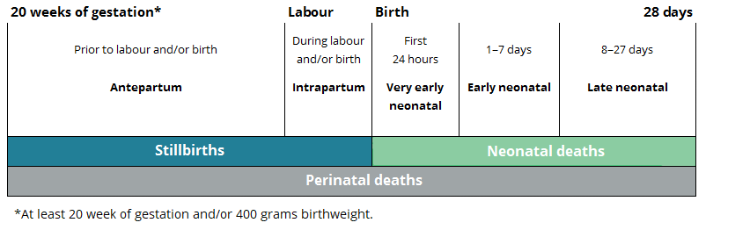 Chart: AIHW
Chart: AIHW
Stillbirth: a fetal death prior to birth of a baby of 20 or more completed weeks of gestation or of 400 grams or more birthweight.
Neonatal death: the death of a live born baby of 20 or more completed weeks of gestation or of 400 grams or more birthweight within 28 days of birth.
Perinatal death: stillbirth or neonatal death of a baby from 20 or more completed weeks of gestation to 28 days following birth or of 400 grams or more birthweight.
Antepartum death: fetal death occurring prior to labour and/or birth.
Intrapartum death: fetal death occurring during labour and/or birth.
Very early neonatal death: death of a live born baby within the first 24 hours after birth.
Early neonatal death: death of a live born baby within 1–7 days after birth.
Late neonatal death: death of a live born baby within 8–28 days after birth.
Live birth: the birth of a baby who shows signs of life such as voluntary muscle movement, pulsating of the umbilical cord or presence of a heartbeat at birth, regardless of whether the placenta is still attached or the umbilical cord has been cut.
Terminations of pregnancy: performed at 20 or more weeks of gestation may be included and recorded either as stillbirths or, in the unlikely event of showing evidence of life, as live births. There are variations in legislation regarding termination of pregnancy between states and territories, and recording of terminations is likely to be incomplete.
Note: following consultation with a range of stakeholders, a standardised definition of termination of pregnancy was finalised by the AIHW in November 2024, with agreement from all states and territories. The AIHW and jurisdictional perinatal custodians are assessing when the new definition will be implemented.
World Health Organization (WHO) definitions
To allow for international comparisons, the WHO recommendation regarding reporting perinatal mortality, taken from the 2006 Neonatal and perinatal mortality: country, regional and global estimates report has been used. The report recommends publication of rates of fetal death of babies weighing 1,000 grams or more, and/or born at 28 weeks’ gestation or more.
This differs from the standard definition used for stillbirths by the WHO, which is the loss of a baby during pregnancy at or after 22 completed weeks of gestation, or if gestational age is not available, with birthweight of 500 grams or more (WHO 2022).
Cause of death classification
The Perinatal Society of Australia and New Zealand (PSANZ) Perinatal Mortality Classification System is used in Australia and New Zealand to classify the causes of stillbirths and neonatal deaths. It is applied to all perinatal deaths, including terminations of pregnancy.
The PSANZ Mortality Classification System includes the PSANZ Perinatal Death Classification (PSANZ-PDC) and PSANZ Neonatal Death Classification (PSANZ-NDC). The PSANZ-PDC system classifies all perinatal deaths into one of 12 categories by the single most important factor seen as the antecedent cause of death. In addition, for neonatal deaths, the PSANZ-NDC system is used to identify the single most significant condition occurring in the neonatal period which resulted in the death.
The PSANZ Perinatal Death Classification is an integral part of the PSANZ Perinatal Mortality Guidelines, developed for optimal standards in investigating, classifying and auditing of perinatal deaths. The classification is recorded as part of each state and territory’s perinatal mortality review process following completion of investigations and at the end of a multi-disciplinary review of the perinatal death. The National Perinatal Mortality Data Collection (NPMDC) includes data on causes of death according to different versions of the PSANZ classification system, based on the year the birth occurred:
- Births occurring between 2013 and 2018 are classified according to the PSANZ Perinatal Mortality Classification System, version 2.2
- Births occurring between 2019 and 2024 are classified according to the PSANZ Classification System for Stillbirths and Neonatal Deaths, version 3
- Births occurring from 2025 onwards will be classified according to the PSANZ Classification System for Stillbirths and Neonatal Deaths, version 5.
The other classification system used in Australia to classify perinatal deaths is the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). This classification system is based on the registered cause/s of death on the Medical Certificate of Cause of Perinatal Death, assigned by the treating medical practitioner shortly after death without access to any subsequent investigations.
The National Maternal and Perinatal Mortality Clinical Expert Group (NMPMCEG) (formerly the National Maternal and Perinatal Mortality Advisory Group (NMPMAG)) has concluded that the PSANZ-PDC and PSANZ-NDC classifications are the most appropriate for national reviews. The ICD classification of cause of death is not collected in the NPMDC.
PSANZ-PDC primary classification groups
Congenital anomaly: deaths in which a congenital anomaly in the baby (whether structural, functional or chromosomal) is considered to have been of major importance in the cause of the death.
Perinatal infection: primary infections occurring in term and preterm neonatal and fetal deaths and secondary infections in term infants (such as Group B Streptococcus and Cytomegalovirus).
Hypertension: deaths where a hypertensive disorder in the baby’s mother, such as pre-eclampsia or pre-existing high blood pressure, is considered to have led to the death.
Antepartum haemorrhage: all perinatal deaths where the primary factor leading to the death was bleeding from the placental bed in the woman’s uterus.
Maternal conditions: deaths where a medical condition (for example, diabetes) or a surgical condition (for example, appendicitis) or an injury in the mother (including complications or treatment of that condition) is the cause.
Complications of multiple pregnancy: deaths of one or more babies in a multiple pregnancy related to the pregnancy being multiple, including complications of the fetal circulations interconnecting (Twin to twin transfusion syndrome) and umbilical cords becoming entangled where the babies are in only one amniotic sac.
Specific perinatal conditions: deaths of normally formed, appropriately grown babies, in which a specific perinatal condition, such as cord entanglement or a blood group incompatibility, was the main underlying cause.
Hypoxic peripartum deaths: deaths from acute or chronic inadequate oxygen supply from the placenta of normally formed babies, typically of >24 weeks’ gestation or >600 grams birthweight.
Placental dysfunction or causative placental pathology: deaths where the placenta is demonstrated to have been poorly functioning, either by post-mortem microscopic examination of the placental or by ultrasound testing of placental and umbilical artery blood flow.
Spontaneous preterm labour or rupture of membranes: deaths of normally formed, appropriately grown preterm babies following spontaneous onset of preterm labour or spontaneous rupture of membranes, irrespective of whether labour was subsequently induced and mode of delivery.
Unexplained antepartum fetal death: deaths of normally formed fetuses prior to the onset of labour where no predisposing factors are considered likely to have caused the death.
Neonatal death without obstetric antecedent: includes Sudden Infant Death Syndrome (SIDS), postnatally acquired infection (such as Newborn Intensive Care Unit-acquired septicaemia from an intravenous line), accidental asphyxiation and other accidents, poisoning or violence.
PSANZ-NDC primary classification groups
The PSANZ-NDC classification system is applied only to neonatal deaths and classifies them by the most significant condition present in the baby, in the neonatal period, leading to the death.
Congenital anomaly: deaths in which a congenital anomaly in the baby (whether structural, functional or chromosomal) is considered to have been of major importance in the cause of the death.
Periviable infants: neonatal death in infants deemed too immature for resuscitation or continued life support beyond the delivery room (typically infants of gestational age ≤24 weeks or birthweight ≤600 grams).
Cardio-respiratory disorders: neonatal deaths in which a cardio-respiratory condition (such as respiratory distress syndrome or meconium aspiration syndrome) is considered to have been the major contributor to the death.
Infection: neonatal deaths in which infection is considered to have been the major contributor (such as early onset Group B Streptococcus sepsis, pneumonia).
Neurological: neonatal deaths in which asphyxial brain damage (hypoxic ischaemic encephalopathy) or intracranial haemorrhage was considered to have been the major contributor.
Gastrointestinal: primarily includes neonatal deaths related to necrotizing enterocolitis (a medical condition where a portion of the bowel dies).
Other: includes Sudden Infant Death Syndrome (SIDS), multisystem failure, trauma and treatment complications.
References
CCOPMM (Consultative Council on Obstetric and Paediatric Mortality and Morbidity) (2025) CCOPMM 2024 annual report – For births and perinatal, maternal and child and adolescent deaths in Victoria in 2023, CCOPMM, Victorian Government, accessed 5 February 2026.