Data source: National Perinatal Data Collection
The National Perinatal Data Collection (NPDC) began in 1991 and collates data on pregnancy and childbirth. The NPDC collects national information on the pregnancy and childbirth of mothers, and the characteristics and outcomes of their babies. A standard de-identified extract is provided from states and territories to the Australian Institute of Health and Welfare (AIHW) on an annual basis to form the NPDC.
The NPDC supports a range of reports and products, including:
- Australia’s mothers and babies
- National Core Maternity Indicators reports and data visualisations
- First Nations mothers and their babies reports
- Maternal and perinatal outcomes during the 2020 and 2021 COVID-19 pandemic
- Maternal deaths in Australia
- other specialist reports, indicator-based reports and customised data requests.
Detailed information on completeness, accuracy and other aspects of data quality for the NPDC is in the data quality statement and information on data availability at the national and state/territory level can be found in the NPDC data availability resource.
Collection of perinatal data by states and territories
Perinatal data are collected after each birth, usually by midwives or other birth attendants using information obtained from the mother, from clinical and administrative records and information systems, including records of antenatal care, the care provided during labour, and the delivery and care provided after the birth. Each state and territory has its own form and/or electronic system for collecting data, which are forwarded to the relevant state and territory health departments to form the state or territory perinatal data collection. See the section on State and territory perinatal data collections for state and territory contact details and the most recent state and territory perinatal reports, which contain more detailed information about data collection in each jurisdiction.
Structure of the National Perinatal Data Collection
Data supplied for the NPDC consist of the Perinatal National Minimum Data Set (Perinatal NMDS) and additional data items.
Figure 1: Structure of the National Perinatal Data Collection
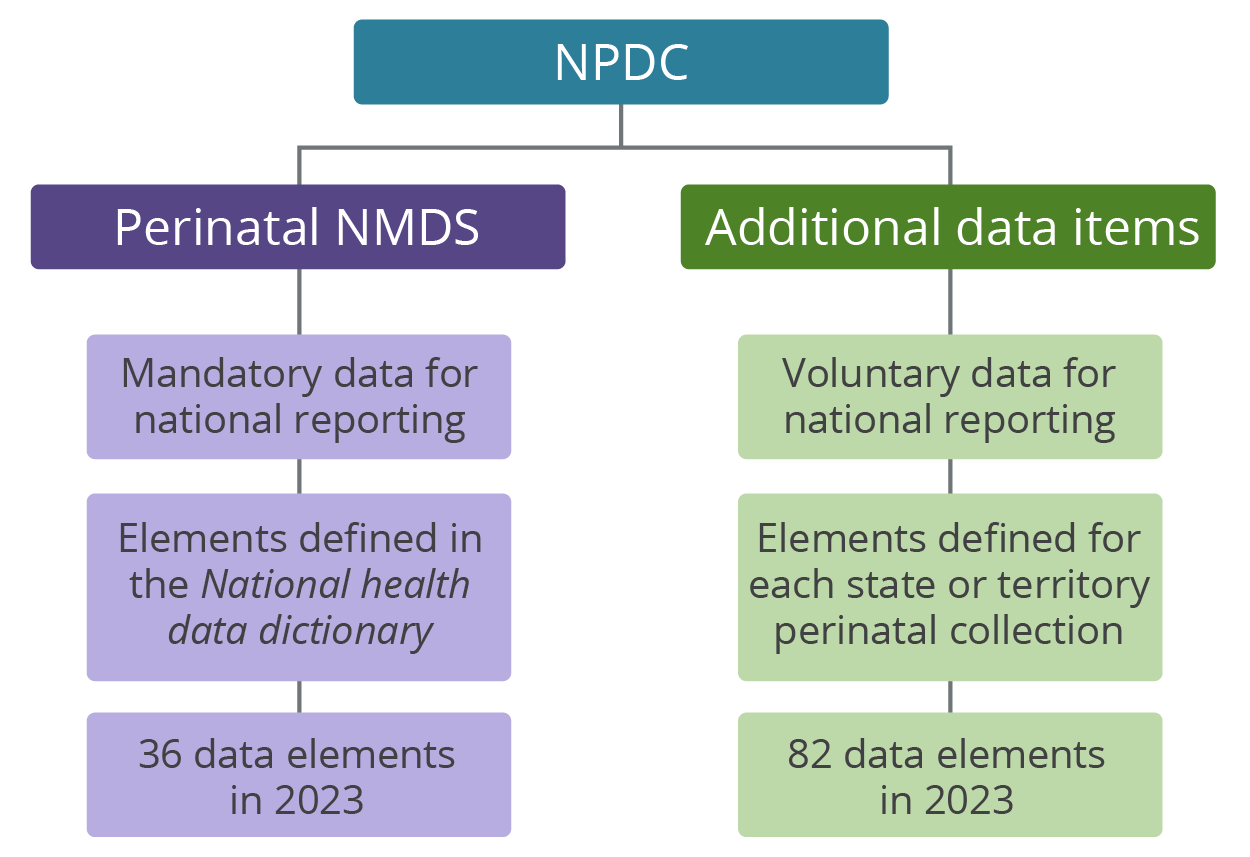
The Perinatal NMDS was first specified in 1997 and is an agreed data set for national reporting (COAG 2012). An NMDS is an agreed set of standardised data elements for mandatory supply by states and territories to support national reporting. Standardisation ensures that there is consistent meaning for data collected at different times or in different places.
For reporting of NPDC data for the 2023 birth cohort, items were supplied for the NPDC from 2 sets of Perinatal NMDS:
- Perinatal NMDS 2022–23 (1 January 2023 to 30 June 2023)
- Perinatal NMDS 2023–24 (1 July 2023 to 31 December 2023).
Each state and territory collects more information than is specified in the Perinatal NMDS, and the AIHW requests some of these additional items. These data items are at different stages in the process of standardisation. Some items have had national data standards developed, but have not yet been included as data elements in the Perinatal NMDS because they could not be implemented immediately in all jurisdictions.
In contrast, there are other data items – for which there are, as yet, no common definitions or categories for collecting the data or which are not collected in all jurisdictions – that are also provided to inform the future development of nationally standardised data.
Which births are counted?
This report presents information from the NPDC about births in Australia, including births in hospitals, in birth centres and in the community. Freebirths may be included in the NPDC if they are in scope of the data collection, and the mother or baby present to hospital following birth, or the birth is registered with the Registry of Births, Deaths and Marriages. However, this differs by state and territory.
The Australian National health data dictionary defines a ‘live birth’ as the complete expulsion or extraction from its mother of a baby, of any gestation, that shows signs of life; and a ‘stillbirth’ is the complete expulsion or extraction of a baby, of at least 20 weeks’ gestation or weighing at least 400 grams at birth (the weight expected of a baby at 20 weeks’ gestational age), which shows no signs of life.
The Perinatal NMDS and the NPDC require that either the birthweight or the gestational age conditions are met for both live births and stillbirths. This means that the very small number of live births occurring before 20 weeks’ gestation and weighing less than 400 grams are not included in the NPDC, although they may have been included in jurisdictional perinatal data collections. Data for babies whose gestational age and birthweight were not recorded are also not included in the NPDC, but may have been included in jurisdictional perinatal collections. Live births and stillbirths include termination of pregnancy after 20 weeks. Stillbirths can include fetus papyraceous and fetus compressus (products of conception recognisable as a deceased fetus). In Victoria and Western Australia, data were included for both live births and stillbirths of at least 20 weeks’ gestation or, if gestation was unknown, the birthweight was at least 400 grams. South Australian data may not include all terminations of pregnancy for psychosocial reasons after 20 weeks’ gestation where birthweight was not recorded.
International comparisons
Care is needed when comparing Australian birth statistics with those from countries that have different gestational age or other criteria for defining live births and stillbirths. In many other countries, pregnancies must continue to 22, 24 or even 28 completed weeks of gestational age for a fetal death to be counted as a stillbirth. The inclusion in Australia of more births at lower gestations will affect the distributions of several key baby outcomes – in particular, rates of perinatal mortality, low birthweight, low Apgar scores (a measure of a baby’s wellbeing at birth) and admission to a special care nursery or neonatal intensive care unit. For live births, the Perinatal NMDS and NPDC definition is more restrictive than the World Health Organization definition that specifies a live birth as a baby born showing signs of life irrespective of gestation (WHO 1992).
National Perinatal Data Development Committee
The National Perinatal Data Development Committee has a key role in improving data quality. The committee comprises representatives from each state and territory health authority and the AIHW, with temporary members invited as their expertise is required. The committee works in consultation with clinical reference groups. It improves data provision, revises existing Perinatal NMDS items, develops existing perinatal data items in METEOR (AIHW’s Metadata Online Registry) and contributes to the development of new perinatal data items.
Data timeliness
The NPDC has almost 120 data items and contains around 300,000 records per year for both mothers and babies. Data for all states and territories are checked for completeness, validity and logical errors before the NPDC is deemed final for a calendar year.
Some states and territories need 12 months or more to undertake data entry, validation and linking with hospitals data as required after the end of the data collection period. The process to finalise data for the national collection can then require multiple rounds of data validation by the AIHW and resupply of data from states and territories.
NPDC data for 2023 was requested from states and territories on 29 August 2024 for submission to the AIHW in a staged supply between 23 September 2024 and 18 November 2024. Data for 2023 were final for all states and territories by 1 July 2025 and were published on 31 July 2025.
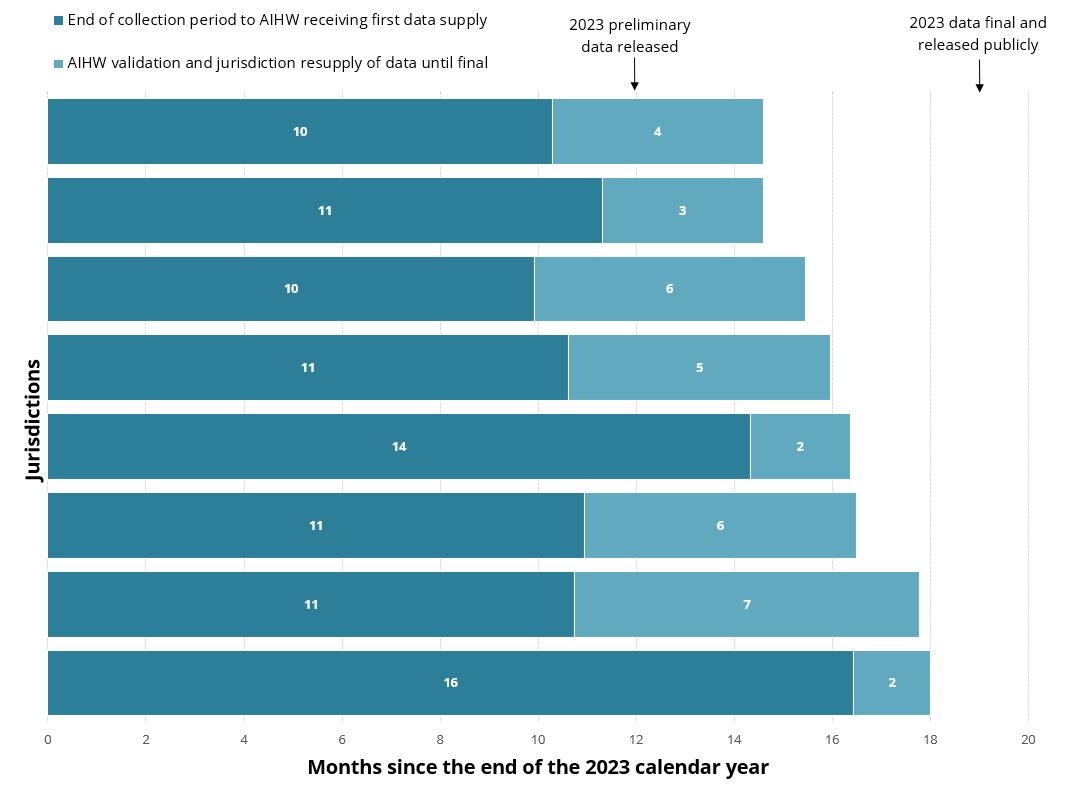
Timelines for reporting 2023 NPDC data are outlined in Figure 3. Preliminary 2023 NPDC data (for 5 of 8 states and territories) was reported within 12 months of the end of the collection period and final data was reported within 19 months of the end of the collection period.
Figure 2: Months since the end of the 2023 calendar period and public reporting of data from the National Perinatal Data Collection, by state and territory
Data quality and availability
Detailed information on completeness, accuracy and other aspects of data quality for the National Perinatal Data Collection (NPDC) is in the data quality statement, and information on data availability at the national and state/territory level can be found in the NPDC data availability resource.
Tabulated data in this report are based on births in each state and territory in 2023 that meet the criteria for inclusion in the Perinatal NMDS. Due to data editing, subsequent updates of state and territory databases, and differences in scope for inclusion, the numbers may differ slightly from those in reports published by the states and territories. For state and territory exclusions, see Table 1.
| Topic | Exclusion |
|---|---|
| Patient classification at hospital of birth | New South Wales in 2023 (data not provided) |
| Smoking at any time during pregnancy | Australian Capital Territory in 2023 (data not available(a)) |
| Smoking during the first 20 weeks of pregnancy | New South Wales in 2021 and 2022 (data not provided) Australian Capital Territory in 2023 (data not available(a)) |
| Smoking after 20 weeks of pregnancy | New South Wales in 2021 and 2022 (data not provided) Australian Capital Territory in 2023 (data not available(a)) |
| Alcohol consumption during the first 20 weeks of pregnancy | New South Wales (data not provided) Australian Capital Territory in 2023 (data not available(a)) |
| Alcohol consumption after 20 weeks of pregnancy | New South Wales (data not provided) Australian Capital Territory in 2023 (data not available(a)) |
| Duration of pregnancy at first antenatal visit | Australian Capital Territory in 2023 (data not available(a)) |
| Number of antenatal visits | Australian Capital Territory in 2023 (data not available(a)) |
| Diabetes status | Victoria in 2018 and 2019 (data not available) Australian Capital Territory in 2023 (data not available(a)) |
| Hypertension status | Victoria in 2018 and 2019 (data not available) Australian Capital Territory in 2023 (data not available(a)) |
| Body mass index (BMI) | New South Wales between 2011 and 2015 (data not provided) Australian Capital Territory in 2023 (data not available(a)) Northern Territory in 2011 and 2012 (data not provided) |
| Previous caesarean section(b) | Australian Capital Territory in 2023 (data not available(a)) |
| Analgesia administered to relieve the pain of labour | Australian Capital Territory in 2023 (data not available(a)) |
| Anaesthesia administered for operative delivery | Australian Capital Territory in 2023 (data not available(a)) |
| Antenatal length of stay(b) | New South Wales in 2023 (data not provided) |
| Postnatal length of stay | Australian Capital Territory in 2023 (data not available(a)) Western Australia (data not provided on baby’s mode of separation(b) from the birth hospital which is required for analysis of this topic) |
| Admission to a SCN/NICU(b) | New South Wales (data not provided) Western Australia (data not provided) Northern Territory in 2021 (data not provided) |
| Baby length of stay in hospital | Australian Capital Territory in 2023 (data not available(a)) Western Australia (data not provided on baby’s mode of separation(b) from the birth hospital which is required for analysis of this topic) Northern Territory in 2021 (data not provided) |
- For more information, see the 'Australian Capital Territory, 2022 and 2023 data' section below.
- These data items are not currently part of the Perinatal NMDS and are not mandated for provision to the NPDC.
Unless otherwise stated, the data in this report and related supplementary tables relate to the state or territory where births occurred in 2023, rather than to the state or territory of usual residence of the mother.
Due to rounding, percentage totals may not add to 100 and subtotals may not sum to the percentages for the categories.
Reporting Indigenous status
Indigenous status is a measure of whether a person identifies as being Aboriginal, Torres Strait Islander, or both Aboriginal and Torres Strait Islander. Indigenous status of the mother has been a mandatory data item for the Perinatal NMDS since its inception in 1997. Indigenous status of the baby was also added to the NMDS for collection for the first time in the 2012–13 reference year (from 1 July 2012).
This item, when used in conjunction with the mother’s Indigenous status, is a better baseline measure of health for all First Nations children. However, the outcomes of babies of First Nations mothers remain a key data resource for assessing antenatal care in pregnancy and other interventions before or during pregnancy, aimed at improving the health of mothers and babies.
Unless otherwise stated, data for babies are based on the Indigenous status of the mother.
Table 2 shows the relationship between Indigenous status of the mother and Indigenous status of the baby in 2023. Most babies (96%) had the same Indigenous status as their mother while only a small proportion had a different Indigenous status recorded (4.5%). However, of the 20,439 babies reported as First Nations in the NPDC in 2023 (7.2% of all babies), about one-quarter (28%) were born to non-Indigenous mothers.
| Indigenous status of the mother | First Nations baby | Non-Indigenous baby | Not stated baby | Total |
|---|---|---|---|---|
| First Nations mother | 14,757 | 1,105 (0.4%) | 205 (0.1%) | 16,067 (5.6%) |
| Non-Indigenous mother | 5,661 (2.0%) | 257,716 (90.3%) | 4,712 (1.7%) | 268,089 (94.0%) |
| Not stated mother | 21 (0.0%) | 620 (0.2%) | 508 (0.2%) | 1,149 (0.4%) |
| Total | 20,439 (7.2%) | 259,441 (90.9%) | 5,425 (1.9%) | 285,305 (100.0%) |
Australian Capital Territory, 2022 and 2023 data
The ACT only provided partial data for 2022 due to a major change in the collection of ACT’s health data, implemented in early November 2022. Therefore, to enable national reporting of 2022 data on mothers and babies, the AIHW constructed a dataset using complete 2022 data for 7 jurisdictions and a compilation of data for the ACT. The ACT’s data consists of their 2022 data for January to October, supplemented by their 2021 data for November and December.
As 2023 was the first full year of data extracted from ACT’s new digital health system, some of ACT’s data are currently unavailable or may not have complete coverage. Care should be taken if comparing data across time and jurisdictions.
Australian Capital Territory, births to non-residents
The Australian Capital Territory data contain a relatively high proportion of New South Wales residents who gave birth in the Australian Capital Territory. The proportion of mothers who gave birth in the Australian Capital Territory who were residents elsewhere was about 16% in 2023.
When interpreting the data, it is important to note that these births to non-residents may include a disproportionate number of high-risk and multi-fetal pregnancies associated with poorer perinatal outcomes. This is because women with high risk pregnancies may be more likely to be transferred from smaller centres in New South Wales (that do not have the facilities to manage such births safely) to the Australian Capital Territory to give birth.
Therefore, percentages or rates such as those for pre-term births and perinatal deaths may be inflated for births that occur in the Australian Capital Territory. Reporting by state or territory of usual residence of the mother helps to address this issue.
References
COAG (Council of Australian Governments) 2012. National Healthcare Agreement 2012. Intergovernmental agreement on federal financial relations. Canberra: COAG. Viewed 31 March 2020.
WHO (World Health Organization) 1992. International Statistical Classification of Diseases and Related Health Problems, 10th Revision. Geneva: WHO.