An overview of colorectal cancer in Australia
Cancer data commentary number 12
Colorectal cancer, often referred to in Australia as bowel cancer, was the most commonly diagnosed cancer in 2000 but in 2024 is estimated to be the 4th most commonly diagnosed cancer in Australia. This commentary provides an overview of colorectal cancer in Australia. Trends and rates by site, type, sex and age are among the items discussed.
This first section provides the main overview of colorectal cancer trends and rates. The following sections look deeper into different aspects of colorectal cancer.
Colorectal cancer incidence rates have decreased more than any other cancer
In 2024, there is an estimated risk that 1 in 21 people will be diagnosed with colorectal cancer by the time they are 85 (1 in 19 for males and 1 in 23 for females). In 2000, at a time when colorectal cancer incidence rates were higher than the estimates for 2024, the risk of being diagnosed by the age of 85 was 1 in 15 (risk figures are adjusted for competing mortality).
Crude incidence rates for colorectal cancer increased from 46 cases per 100,000 people in 1982 to a peak of 69 cases per 100,000 people in 2007. By 2024, the crude incidence rates are estimated to decrease to 57 cases per 100,000 people. The increase of crude rates between 1982 and 2024 is entirely due to the ageing population (that is, with people living to older ages, proportionally more of the population is older today than in the 1980s and at ages of higher colorectal cancer risk).
When adjusted for age, colorectal cancer incidence rates increased from 74 cases per 100,000 people in 1982 to a peak of 86 cases per 100,000 in 2001. The incidence rate has since decreased to an estimated 57 cases per 100,000 people in 2024 (Figure 1). This is an estimated 33% decrease of age-adjusted incidence rate between 2001 and 2024. The reduction in colorectal cancer age-adjusted incidence rates since 2000 is greater than any other cancer.
The most significant decreases of colorectal cancer incidence rates this century coincided with the introduction of the National Bowel Cancer Screening Program (NBCSP). The NBCSP was introduced in Australia in 2006 and colorectal cancer age-standardised incidence rates have been steadily decreasing since 2007 (Figure 1). One of the aims of the NBCSP is to reduce morbidity and mortality from colorectal cancer through early detection of pre-cancerous lesions (polyps and adenomas) some of which can develop into cancer. These polyps can be removed before developing into cancer thereby reducing the incidence of colorectal cancer (AIHW, 2024).
Figure 1: Colorectal cancer, incidence counts and age-standardised rates, persons, 1982 to 2024

Notes
- Rates are standardised to the 2024 Australian population.
- Various cancers recorded a decrease in cases diagnosed in 2020; a year where COVID-19 restrictions were in place and impacted access to medical services.
- 2021 to 2024 are projections for incidence and age-standardised rates.
Source: AIHW Australian Cancer Database 2020
The number of colorectal cancer cases diagnosed each year has remained relatively stable in recent years
In 2000, when colorectal cancer age-adjusted incidence rates were near the peak, there were around 12,400 cases of colorectal cancer diagnosed. After years of age-adjusted incidence rates decreasing, it is estimated that about 15,500 new cases of colorectal cancers will be diagnosed in 2024. From 2010, the number of colorectal cancer cases diagnosed each year has generally been around 15,000 cases. In 2010, colorectal cancer accounted for 13% of all cancer cases diagnosed and in 2024, it is estimated to account for 9%.
The stability in the number of colorectal cancer cases diagnosed while age-adjusted rates are decreasing is due to the decreasing rates being offset by population growth and an ageing population. The ageing population impacts cancer cases due to greater proportions of the population living to older ages and cancer rates being higher in older ages.
Figure 2: Colorectal cancer and all cancers combined, number of cases diagnosed, persons, 2010 to 2024

Notes
- 2021 to 2024 are projections.
- Various cancers recorded a decrease in cases diagnosed in 2020; a year when COVID-19 restrictions were in place and impacted access to medical services.
Source: AIHW Australian Cancer Database 2020
Colorectal cancer survival rates have improved consistently over time
In 1991–1995, 56% of people diagnosed with colorectal cancer survived 5 years or more (unless otherwise stated, all survival rates are relative survival rates). By 2016–2020, the 5-year survival rate had improved to 71%. The 5-year survival rate for females was slightly higher than males (72% compared to 70% in 2016 – 2020) (Figure 3).
Figure 3: 5-year relative survival rates, by males, females and persons, colorectal cancer, 1991–1995 to 2016–2020
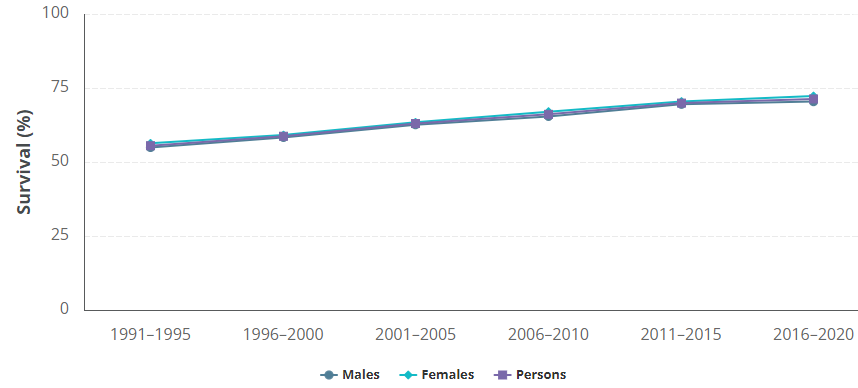
Source: AIHW Australian Cancer Database 2020
Colorectal cancer mortality rates are decreasing but not the number of deaths
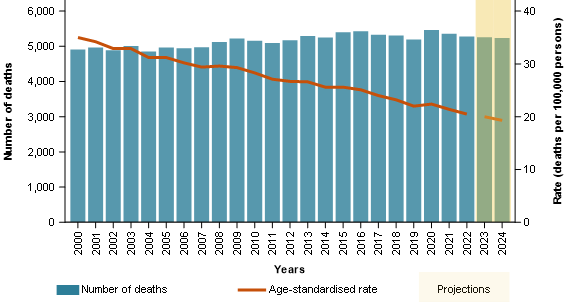
Consistent with incidence rates decreasing and survival rates increasing, colorectal cancer mortality rates have been decreasing. The crude mortality rate for colorectal cancer decreased from 26 deaths per 100,000 people in 2000 to an estimated 19 deaths per 100,000 people in 2024. The age-standardised mortality rate decreased from 35 deaths per 100,000 people in 2000 to an estimated 19 deaths per 100,000 people in 2024 (Figure 4).
Even with the decreasing mortality rates and improvements in survival, there have not been sustained decreases in the annual number of deaths from colorectal cancer. This is because the decreasing mortality rates are offset by population increases and the ageing population. Since 2000, the number of deaths from colorectal cancer have been increasing gradually but have become relatively more stable since 2015 (Figure 4).
The colorectal cancer incidence and mortality trends highlight the challenge that an ageing and increasing population presents. From 2000 to 2024, the Australian population has increased by 43% but the population aged over 70 increased by 98%. The change is even greater for males where the increase is 43% overall and 117% for the population aged over 70. Among people aged over 70, males have higher rates of colorectal cancer (271 cases per 100,000 males estimated in 2024 compared to 230 cases per 100,000 females).
Figure 4: Colorectal cancer, mortality counts and age-standardised rates, persons, 2000 to 2024
Notes
- Rates are standardised to the 2024 Australian population.
- 2023 and 2024 are projections for deaths and age-standardised mortality rates.
Source: AIHW National Mortality Database
Screening for colorectal cancer aims to decrease incidence and mortality among the at-risk population
As noted previously, the NBCSP was introduced in Australia in 2006. Originally it targeted people aged 55 and 65. In 2015, the age range was expanded to include all asymptomatic people aged between 50 and 74 with the expansion occurring on a rolling basis with full implementation by July 2020.
The symptoms of colorectal cancer often appear in the later stages of the disease, when fewer treatment options are available. The NBCSP involves using the at-home immunochemical faecal occult blood test (iFOBT) every two years. It is a non-invasive test that can detect microscopic amounts of blood in a sample from a bowel motion. This may indicate precancerous polyps and adenomas, and early-stage cancers (AIHW, 2023). Early diagnosis of colorectal cancer can improve survival. Removal of polyps and adenomas also reduces their risk of developing into cancer.
The AIHW’s National Bowel Cancer Screening Program monitoring report (2024) notes that the national participation rate increased from 39% of invited people in 2014–2015 to 44% in 2019–2020, then reduced to 40% in 2021–2022. While the NBSCP was not suspended during the COVID-19 pandemic and bowel cancer screening was not directly impacted, the reduction in screening participation rate in 2020–2021 may be because people were less willing to visit medical practitioners or complete the at-home screening whilst under restrictions. About six percent of people, who participated in the NBCSP in 2022, received a positive screening result that warranted further assessment (AIHW, 2024).
Colorectal cancer in the population under 50
Colorectal cancer incidence rates are decreasing in the older population but increasing in the under 50s
The colorectal cancer incidence rate for the population 50 years and older has been decreasing over the past 20 years. Between 2000 and 2024, it decreased from 213 to an estimated 142 cases per 100,000. While colorectal cancer in this age group is being diagnosed less frequently, which may at least partly be due to prevention through NBCSP’s early detection of pre-cancerous polyps and adenomas, the number of cases diagnosed in the population aged under 50 more than doubled over this time from 960 cases in 2000 to an estimated 2,045 cases in 2024.
Increasing rates of colorectal cancer are occurring in the younger population in several high-income countries, including Australia. Despite the widespread increase in the incidence of early-onset colorectal cancer, the factors causing this increase are not clear. Diagnosis in younger people may be delayed as the symptoms may be attributed to other causes, particularly given that colorectal cancer is more commonly associated with older age groups (AIHW, 2021). Early-onset patients are also more likely to be diagnosed in the later stages when it is more difficult to treat (Bowel Cancer Australia, 2020).
Early-onset colorectal cancer, often defined as that occurring in people under the age of 50, still accounts for only a fraction of the total cases but the incidence rate has been increasing. Between 2000 and 2024, the incidence rate increased from 7 to an estimated 12 cases per 100,000 people. In 2024, around 13% of colorectal cancer cases are estimated to be diagnosed in the population under 50 years of age, an increase from 8% in 2000.
Early-onset colorectal cancer affects both males and females; however, more females under the age of 50 are estimated to be diagnosed with colorectal cancer (an estimated 1,062 cases in females and 983 cases in males in 2024). Younger females are estimated to have a slightly higher incidence rate of 12 cases per 100,000 females compared to 11 cases per 100,000 males in 2024.
The rise in incidence, coupled with an increase in population, has led to an increase of 35% in the number of deaths from early-onset colorectal cancer between 2000 and 2024. Over the same time, the number of deaths from colorectal cancer increased by 5% in the population over 50 years of age. To further distinguish between the differing trends, the population increase for people aged under 50 was 29% between 2000 and 2024 while for the population over 50 it was 77%.
In 2024, colorectal cancer is estimated to be the leading cause of cancer death among men aged under 50 (estimated 164 deaths) and the second leading cause of cancer death in women aged under 50 (estimated 153 deaths for colorectal cancer following an estimated 266 deaths for breast cancer).
The increase in colorectal cancer diagnoses in the younger population has coincided with the lowering of the screening age in many countries, including Australia. In 2021, at-risk people in the USA were recommended to be screened for colorectal cancer starting at age 45, rather than the previous recommendation of 50 (Carethers, 2022). In 2024, the Australian Government lowered the starting age of the NBCSP to include eligible people between the ages of 45 and 49 (Department of Health, Disability and Ageing, 2024).
Sites and subsites of colorectal cancer
Colon is the most commonly diagnosed site of colorectal cancer
The colorectal region of the body includes the colon and rectum as well as the rectosigmoid junction which joins the two. Colon cancer represented 66% of all colorectal cancers in 2000 while 26% were diagnosed in the rectum and 8% were diagnosed in the rectosigmoid junction. The majority of colorectal cancer cases continue to be diagnosed in the colon (estimated 71% in 2024), followed by the rectum (estimated 22% in 2024) and the rectosigmoid junction (estimated 7% in 2024).
Overall, the incidence rate of colorectal cancer in the three sites has been decreasing (Figure 5). The age-adjusted colon cancer incidence rate increased from 49 cases per 100,000 people in 1982 to a peak of 57 cases per 100,000 in 2001 and is estimated to continue to decrease to 41 cases per 100,000 people in 2024. Rectal cancer incidence rates have been decreasing from 2007 (22 cases per 100,000 people in 2007) and are estimated to decrease to 13 cases per 100,000 people in 2024. Figure 5 contrasts the crude and age-specific rates for colorectal cancer diagnosis by site, overall and for the 0 to 49 and 50 and above age groups.
While the incidence rate of colorectal cancer in the three sites is on the decline in the population aged 50 years and over, it is increasing in the population aged under 50 (Figure 5). Most of the increases in colorectal cancer in the young are due to colon cancer. Since 2000, the number of colon cancer cases diagnosed in people aged under 50 years more than doubled from 585 cases to an estimated 1,352 cases in 2024. Colon cancer rate increases for 30–39-year-olds were from 4 cases in 2000 to an estimated 11 cases per 100,000 people, the 40–49-year-olds rates increased from 14 to an estimated 18 cases per 100,000 people while the rate for the population under 30 increased from 1 to an estimated 2.8 cases per 100,000 people. More than 85% of the colorectal cancer cases diagnosed in people aged under 30 years occurred in the colon (Figure 6).
The proportion of colorectal cancer cases that occur in the rectum and rectosigmoid junction increase with age with the greatest proportions occurring between the ages of 45 and 59, then declining in the older age groups. In 2020, about 35% of colorectal cancers diagnosed in people aged 45 to 59 years occurred in the rectum and 8% occurred in the rectosigmoid junction. Rectal cancer is not commonly diagnosed in the younger age groups; however, its incidence rate in 30–39-year-olds increased from 2.1 to an estimated 5.2 cases per 100,000 people from 2000 to 2024.
Figures 5: Age-specific incidence rates of colon, rectosigmoid junction and rectal cancers, persons, by all ages, 0 to 49 years and 50 years and older age groups, 2000 to 2024
 Notes
Notes
- Rates for all ages are crude. Rates for age-groups are age-specific.
- 2021 to 2024 are projections for age-specific incidence rates.
Source: AIHW Australian Cancer Database 2020
Figure 6: Proportion of colorectal cancer cases, persons, by site and age groups, 2020

Source: AIHW Australian Cancer Database 2020
The proportion of deaths due to colorectal cancer diagnosed in the rectum has increased in the young since 2007
Consistent with an overall decreasing incidence rate and increasing 5-year survival rate (63% in 2001–2005 to 71% in 2016–2020), the age-adjusted mortality rate for colon cancer has decreased since 2007 from 20 deaths to an estimated 13 deaths per 100,000 people in 2024. An estimated 6% of the deaths from colon cancer in 2024 occurred in people under the age of 50 years.
Similarly, the age-adjusted mortality rate of rectal cancer almost halved from 7.7 deaths per 100,000 people in 2007 (1,319 deaths) to an estimated 4.2 deaths per 100,000 people in 2024 (estimated 1,149 deaths). In 2007, about 6% of the deaths due to rectal cancer occurred in people aged under 50; however, this proportion is estimated to have increased to about 9% in 2024. The overall 5-year survival rate of rectal cancer has improved from 64% in 2001–2005 to 73% in 2016–2020.
Most commonly diagnosed subsite of colon cancer varies by age
Overall, when considering colon cancer incidence, the composition of diagnosis by cancer subsite changes with age. There are ten subsites of colon cancer including the caecum, appendix, ascending colon, hepatic flexure, transverse colon, splenic flexure, descending colon, sigmoid colon, overlapping lesion of colon and unspecified colon cancer. The colon cancer subsites more commonly diagnosed for younger populations completely contrast the composition for older ages.
One of the main subsites for the increase in colon cancer in people under 50 years of age is appendiceal cancer. In 2000, appendiceal cancer accounted for 1% of colorectal cancers diagnosed in people of all ages and by 2024 it is estimated that it will account for 6% of colorectal cancers. Although rare within the population overall, it is the most common colon cancer subsite for people under the age of 30; for people aged under 15, it is estimated to account for almost all colon cancers diagnosed in 2020 (Figure 7). As age groups increase, it becomes more likely that colon cancer will be diagnosed in sites other than the appendix.
Colon cancer occurs across all subsites for 30–39-year-olds. In 2020, the most commonly diagnosed subsite in this age group was the sigmoid colon (29%), followed by the appendix (26%). Sigmoid colon is closer in proximity to the rectum. Similar to how rectal cancer represents proportionally more cases of colorectal cancer for the 45 to 59 age groups, the sigmoid colon represents proportionally more cases of colon cancer for these ages (Figure 7). Sigmoid colon cancer is more commonly diagnosed between the ages of 45 and 59 years. The proportion of colon cancer diagnosed in this subsite increases from 4% in the 20 to 24 age group to a peak of 43% in the 50 to 54 age group before decreasing to 17% in the 90+ age group. The 90+ age group has higher rates where a specific subsite cannot be identified during diagnosis therefore the proportion diagnosed in other sites may be understated to some extent.
The proportion of appendiceal cancer declined with increasing age groups. In contrast, the proportion of caecum, ascending colon and transverse colon cancers were more likely to increase with increasing age groups, occurring more frequently in people aged 65 years and older. The caecum is a pouch that connects the small intestine to the colon, which is a part of the large intestine. The subsite next to the caecum in the colon is the ascending colon. In 2020, about 1,500 caecum cancer cases and 1,450 ascending colon cancer cases were diagnosed among people aged 65 years and over. These subsites made up about 44% of all colon cancers diagnosed in the older age groups combined.
Figure 7: Proportion of colon cancer, by subsites and age groups, persons, 2020

Source: AIHW Australian Cancer Database 2020
Screening and improving survival rates for colorectal cancer
Screening for colorectal cancer may have contributed to Australia’s improving survival rates for colorectal cancer because one of the aims of the National Bowel Cancer Screening Program is to detect cancers at an earlier stage, which is associated with better survival. The survival rate of people diagnosed with colorectal cancer between 1986 and 1990 generally decreased for increasing age groups. While this is still generally true for people diagnosed between 2011 and 2015, 50–59-year-olds had a higher survival rate (76%; 95% CI:75.3–77.0) than 40–49-year-olds (73%; 95% CI:72.0–74.8) (Figure 8). This trend is observed again in 2016–2020 as 50–59-year-olds had a slightly higher survival rate (76%; 95% CI: 75.4–77.2) than 40–49-year-olds (75%; 95% CI:74.2–76.8). This improvement in survival rate in 50–59-year-olds could possibly reflect the impact of the screening program.
For people diagnosed with caecum cancer in 2011–2015, the survival rate decreased from 68% for 30–39-year-olds to 66% in 40–49-year-olds, then increased to 68% in 50–59-year-olds and 72% in 60–69-year-olds before continuing to decrease with increasing age groups. This general trend is seen again in 2016–2020 except that the survival rate continues an upward trend until the 70 to 79 age group before it starts to decrease with increasing age groups. This increase in survival rate may indicate a cohort effect due to the introduction of the NBCSP in 2006 for people aged 55 and 65
A similar trend of lower survival rates for 40–49-year-olds than 50–59-year-olds is also seen across all the other the subsites of colon cancer between 2016 and 2020, except for appendiceal cancer. Of all the colon subsites, appendiceal cancer has the overall highest survival rate (85% in 2016–2020)–this rate decreased for increasing age groups. Appendiceal cancer cannot be reliably detected through current bowel cancer screening test (Moffitt Cancer Center, 2024). Many people are incidentally diagnosed with appendiceal cancer after appendix removal for appendicitis (Van de Moortele, M., et al. 2020).
Figure 8: Colorectal cancer survival rates, by site and age groups, 1986–1990 to 2016–2020 (data visualisation)
Data visualisation (Tableau) provides the observed and relative survival rates 1 to 5 years after colorectal cancer diagnosis by site and 10-year age groups. Data is provided for the periods 1986-1990, 1991-1995, 1996-2000, 2001-2005, 2006-2010, 2011-2015 and 2016-2020. The survival rates improved over time for all sites but survival decreases with age.

Colorectal cancer histology
Majority of colorectal cancers are adenocarcinomas, but the incidence rate has been gradually decreasing
Histology describes the type of cells in which the cancer originates. Adenocarcinoma is a type of cancer that starts in mucus-producing cells. It can develop in any organ that has these types of cells. About 90% of all colorectal cancers are adenocarcinomas. There are different types of adenocarcinomas including adenocarcinomas not otherwise specified (NOS), mucinous adenocarcinoma, adenocarcinoma in tubulovillous adenoma, adenocarcinoma in adenomatous polyp and adenocarcinoma in villous adenoma.
The incidence rate of colorectal adenocarcinomas has decreased–from 61 cases per 100,000 people in 2001 to 41 cases per 100,000 people in 2020. The incidence of colorectal adenocarcinomas increases with increasing age groups. In 2020, almost all colorectal adenocarcinomas (about 96%) were diagnosed in people aged 40 years and over (Figure 9). The overall five-year survival rate for colorectal adenocarcinomas was 73% for the 2016–2020 period.
The incidence rate of colorectal neuroendocrine neoplasms is increasing
Neuroendocrine neoplasms (NENs) are tumours that form in neuroendocrine cells. As part of the neuroendocrine system, these cells make hormones and release them into the bloodstream to control normal body functions such as digesting food. Neuroendocrine cells are found throughout the body, but mainly in the gastro-intestinal tract, pancreas, and lungs.
In 2020, there were 804 cases of colorectal NENs. This made up 5.5% of all colorectal cancer cases. Although rare, the incidence rate of colorectal NENs tripled from 1.3 cases per 100,000 people in 2001 to an estimated 3.0 cases per 100,000 people in 2020. The number of colorectal NENs diagnosed in people aged under 40 increased from 60 cases in 2001 to 294 cases in 2020, which was about a 4-fold increase. The number of colorectal NENs diagnosed in people aged 40 and over increased from 190 cases in 2001 to 510 cases in 2020, which was about a 2- to 3-fold increase.
Besides a true increase in the incidence of this malignancy, the steady rise of NEN diagnoses over the years may also be at least partly explained by various factors such as improvements in imaging technologies, increased use of endoscopy and colonoscopy, increased awareness in clinical practice and the introduction of the 2010 World Health Organisation classification for neuroendocrine tumours (Wyld D et al. 2019).
There are three main types of NENs: neuroendocrine tumours (NETs), neuroendocrine carcinomas (NECs) and mixed neuroendocrine and non-neuroendocrine neoplasms. Between 2001 and 2020, 83% of colorectal NENs were NETs, 13% were NECs and the rest were mixed neuroendocrine and non-neuroendocrine neoplasms.
Unclassifiable carcinomas and other histology types were diagnosed more frequently in older age groups. Other histology types include squamous cell carcinoma, sarcoma, and unclassifiable malignant neoplasms. These histology types, combined, made up less than 10% of all colorectal cancer cases in 2020.
Figure 9: Proportion of colorectal cancer, by histology and age groups, persons, 2020

Source: AIHW Australian Cancer Database 2020
Colorectal cancer histology differs considerably by age
Most of the colorectal cancer cases diagnosed in the population aged up to 24 years were neuroendocrine neoplasms (Figure 9). The proportion of neuroendocrine neoplasms decreased for increasing age groups and they represented less than 1% of colorectal cancer cases diagnosed for people aged 85 years or more. The proportion of colorectal NENs, especially in the younger population, increased over the years. For example, the proportion of colorectal cancers that were NENs increased from 73% in 2007 to 94% in 2020 among 15–19-year-olds. The incidence rate increased by around four-fold for those aged 30–39 from 0.8 to 3.3 cases per 100,000 people from 2007 to 2020, and the mortality rate remained low over this period. Besides a true increase in NENs, this increase may be due at least in part to improvements in diagnostic procedures and increased awareness in clinical practice over this period.
Most subsites of colon cancer had a similar distribution of histology where more than 90% of cases diagnosed were adenocarcinomas and less than 3% were neuroendocrine neoplasms. In contrast, appendiceal cancers were predominantly diagnosed as NENs; representing 47% of all appendiceal cases in 2007 and increasing to 58% in 2020. More females are diagnosed with appendiceal NENs than males, regardless of age. In 2020, the incidence rates for appendiceal NENs were 1.7 cases per 100,000 females and 1.2 case per 100,000 males.
The majority of colorectal NENs are NETs, which have high 5-year relative survival rates (97% in 2016–2020). In contrast, colorectal NECs are an aggressive type of colorectal cancer and have a much lower survival rate (44% 5-year relative survival in 2016–2020). Although they are not as commonly diagnosed as colorectal NETs, the number of colorectal NEC cases has increased from 23 in 2007 to 154 in 2020, with incidence rates increasing for the same period from 0.1 to 0.6 cases per 100,000 people.
The proportion of colorectal cancers diagnosed as adenocarcinomas decreased between 2007 and 2020 in younger age groups. In 2007, around 71% of colorectal cancers diagnosed among those aged 25–29 were adenocarcinomas. By 2020, this proportion had decreased to around 43% (Figure 10).
Overall, the incidence and mortality rates of colorectal adenocarcinomas are decreasing. However, for the 30–39 age group, incidence rates increased from 6.7 in 2007 to 11.3 cases per 100,000 people in 2020 and the mortality rate increased from 1.4 to 2.2 deaths per 100,000 people over the same period (Figure 10). Many of these cases were diagnosed in the rectum and colon, specifically the sigmoid colon.
Over 80% of colorectal cancer deaths are associated with a diagnosis of a colorectal adenocarcinoma. The overall mortality rate of colorectal adenocarcinomas decreased from 26 to 18 deaths per 100,000 people between 2007 and 2020; however, it increased over the same period in people aged between 30 and 49 years. Despite the increase in mortality rate, the survival rate for colorectal adenocarcinoma in age groups between 30 and 49 improved. For example, the survival rate for people aged between 35 and 44 years increased from 69% in 2006–2010 to 74% in 2016–2020.
In 2020, the majority of colorectal adenocarcinomas were adenocarcinoma, NOS (67%), followed by mucinous adenocarcinoma (7.1%), adenocarcinoma in tubulovillous adenoma (6.1%) and others. Although there were slight changes in the proportions over the years (e.g. 68% adenocarcinoma, NOS, 7.6% mucinous adenocarcinoma and 8.0% adenocarcinoma in tubulovillous adenoma in 2007), the types of colorectal adenocarcinomas diagnosed have mostly remained the same. The proportions of deaths by the types of colorectal adenocarcinoma follow the same pattern as the cases diagnosed.
Figure 10: Colorectal cancer incidence rates and proportions, and mortality rates and proportions, by site and histology, 2007 to 2020 (data visualisation)
Data visualisation (Tableau) provides the incidence and mortality rates of colorectal cancer and its sites, and subsites by cancer type from 2007 to 2020 for 5-year and 10-year age groups. All rates are expressed as per 100,000 persons. Age-specific rates, crude rates and rates age standardised to the 2001 and 2024 Australian Standard Populations are provided. Figure 10.2 provides the cancer type as a percentage of the selected cancer cases and deaths from 2007 to 2020.
