Conceptual overview
Use (or non-use) of primary health care is the end result of a complex set of interacting individual, community and health system factors that incorporates the perceived needs for health care, the ability and capacity of the system to meet those needs, and individuals’ ability to access the system (Andersen 2008; Bharmal et al. 2015; Gulliford et al. 2002).
Statistics on the use of primary health care services (as seen in associated administrative data) reflect the interaction between these individual and systemic factors. This interaction was particularly highlighted by changes in the use of primary health care during the early part of the COVID-19 pandemic (AIHW 2022).
Understanding these factors is critical for highlighting gaps or areas for improvement (as well as recognising where services/the health system does well). Conceptual frameworks that explicitly lay out the key factors and their relationships provide a visual guide that can be used to drive the selection of variables and methodologies for empirical research projects, both qualitative and quantitative.
In 2013, Levesque and colleagues published their conceptual framework of health care access (the Framework) (Levesque et al. 2013), which highlighted the steps people generally go through in seeking and obtaining care; it also explicitly illustrated how each step is affected by individual and systemic factors (Figure 2.1). The Framework has since been widely used by other researchers (for example, Corscadden et al. 2016; Gordon et al. 2020). See Cu et al. 2021 for a review of studies using the Framework.
There are 2 other main conceptual models of health care use that also consider the importance of both individual/family and contextual/structural/policy factors:
- Andersen’s behavioural model of health service use (Andersen 2008; Artuso et al. 2013; Lederle et al. 2021; Travers et al. 2020)
- ecological models (Akbar et al. 2020; Kennedy et al. 2021; O’Keefe et al. 2022).
Both of these models are also valid, and there is a great deal of overlap in the key concepts across all 3 conceptual frameworks. Levesque’s model (Figure 2.1) was selected for this report as being the most useful from a practical perspective because of how it highlights the decision points along the way – from identifying a health care need through to using health care (and then the potential impact the experience of using that care has on a person’s health status and future health care use). Their work also provide examples of the details underpinning each of the concepts visually within the Framework.
The Framework shows that there are a range of systemic characteristics that can help to facilitate or hinder access to and use of health care, and that they may affect different points along the pathway. These include being approachable, acceptable, available, affordable and appropriate. Characteristics that indicate an individual’s ability to interact with health care include the ability to perceive, seek, reach, pay and engage with health care, and there is interaction between the individual and systemic factors (Millar et al. 2023).
Figure 2.1: Model of health service access

Source: Levesque et al. 2013.
From a practical perspective, according to the Framework, in order for a person to get to the point of using health care:
- a health care need must exist (which could be as diverse as an injury, symptoms of an acute or chronic illness, chronic disease management items such as blood tests, being due for preventive care measures, and so on)
- the person must both perceive that this need exists and want to access care to resolve it (which may be affected by their and their community’s previous experiences with health care)
- if the person does want to seek care, they need to know where and how to access it (Do they ring to make an appointment? Do they need a referral?)
- the person then needs to be able to access that health care – logistically and financially (while this includes transport, it also includes other aspects such as whether the person is able to get time off work or whether child care is available if needed)
- if the person is then able to use that health care when needed, the expectation is that there will be improvements in health. Although presented as a linear process, the person’s experience with that care may also influence if/when/how they seek care in the future.
These 5 stages are affected by a person’s individual and family circumstances as well as by the ways in which the health system itself is structured. For example, health promotion activities can make people aware of the need for preventive health care as well as how to access it, while health care costs are affected by government policies and funding. Individuals’ health literacy, beliefs, and previous experiences with the health system can affect both how the person defines their own health needs and the type of health care they would prefer to attend. As originally conceived, the individual and system factors are paired at each point.
While the Framework was developed from a mainstream perspective, the key elements are applicable to Aboriginal and Torres Strait Islander people (with some adjustments and added perspectives). In 2016, Davy and colleagues used the Framework to guide their review and synthesis of literature on Aboriginal and Torres Strait Islander people’s access to Aboriginal and Torres Strait Islander primary health care services, adding insights into the ways in which the individual and systemic factors operated as barriers or facilitators in each of the 5 stages (Davy et al. 2016).
These authors recommended 2 changes to the Framework – explicitly including the broader health system that sits behind and influences the local health care available to people in their own communities, and redrawing the Framework to make it clear that there are interactions between individual and systemic factors at all 5 stages. For example, their review found that some of the systemic factors (such as cost) have an effect throughout the stages, not just at the point of ‘affordability’. In other words, there were not any issues with the elements themselves, but more with how they were defined for Aboriginal and Torres Strait Islander people and how they interact.
Another expansion of the Framework was recently published by Szymczak et al. (2023), with an explicit focus on the dynamic nature of the 5 stages along the primary health care pathway and the impact of systemic factors. Their framework (which was done for the United States) has been adapted to illustrate the key factors for Aboriginal and Torres Strait Islander people.
Figure 2.2 highlights that access to and use of primary health care is an ongoing process throughout a person’s life. Although these cycles are experienced by individuals, the aggregate effect of them can affect population health outcomes. The model developed by Szymczak and colleagues also illustrates that, on the ground, each episode of health care use involves an interaction with a person, not just a system. The care-seeking cycle also shows that, on some occasions, care is not reached (that is, a person was unable to get the care they needed).
Further, Figure 2.2 shows that all 5 stages of the process along the primary care pathway are affected by broader social, historical, economic, and cultural contextual factors which in turn affect individuals’ own health, health behaviours, access to resources, and health service use (or non-use).
For Aboriginal and Torres Strait Islander people, discussions of health status/health needs and the other stages in the health care journey cannot be separated from the historical and policy context. The long-term effects of colonisation and its ongoing impact on matters such as self-determination, the disruption of ties to land, and the adverse impact of direct and systemic racism (Osborne et al. 2013; Reading and Wien 2009; Thurber et al. 2021) all continue to have an impact on Aboriginal and Torres Strait Islander people’s health and wellbeing. Experiences of racism and discrimination within the health system and by individual health workers make people less able or willing to engage with the system (Bailie et al. 2015; Baker et al. 2021; Li 2017; McInman 2000).
Figure 2.2: Process model of health care access, quality and safety
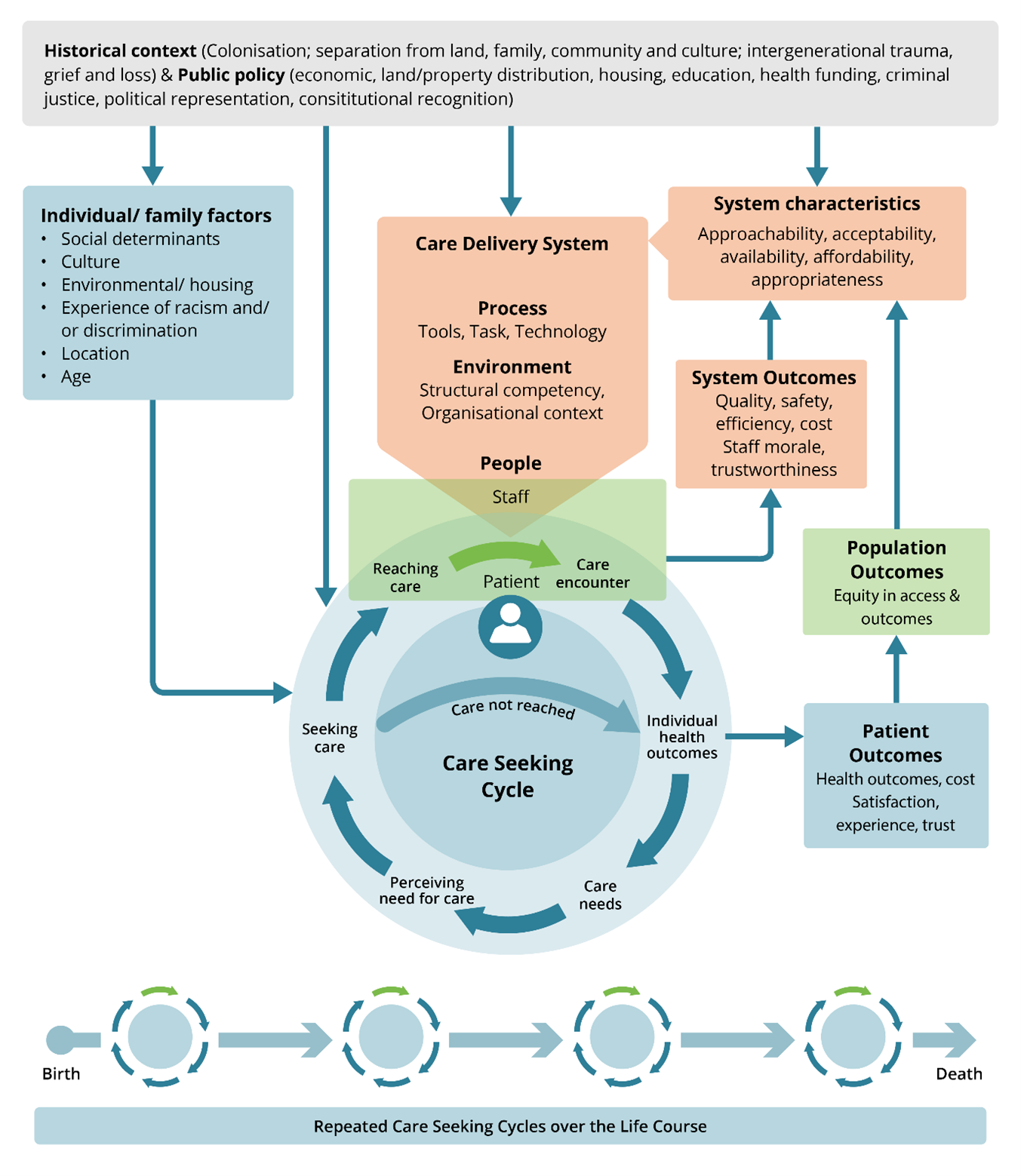
Source: Adapted from Szymczak et al. 2023.