Approach
This project adopted a conceptually-based, multi-faceted approach by bringing together Aboriginal and Torres Strait Islander people’s own lived experiences of primary health care use and their unmet needs (as reflected in the survey data) with an analysis of the current patterns of where primary health services are located relative to where Aboriginal and Torres Strait Islander people live. An overview of the 2 streams of work are presented in figures 1.1 and 1.2.
Overview of the analysis of the 2018–19 NATSIHS
Figure 1.1: Steps for the analysis of the 2018–19 NATSIHS data
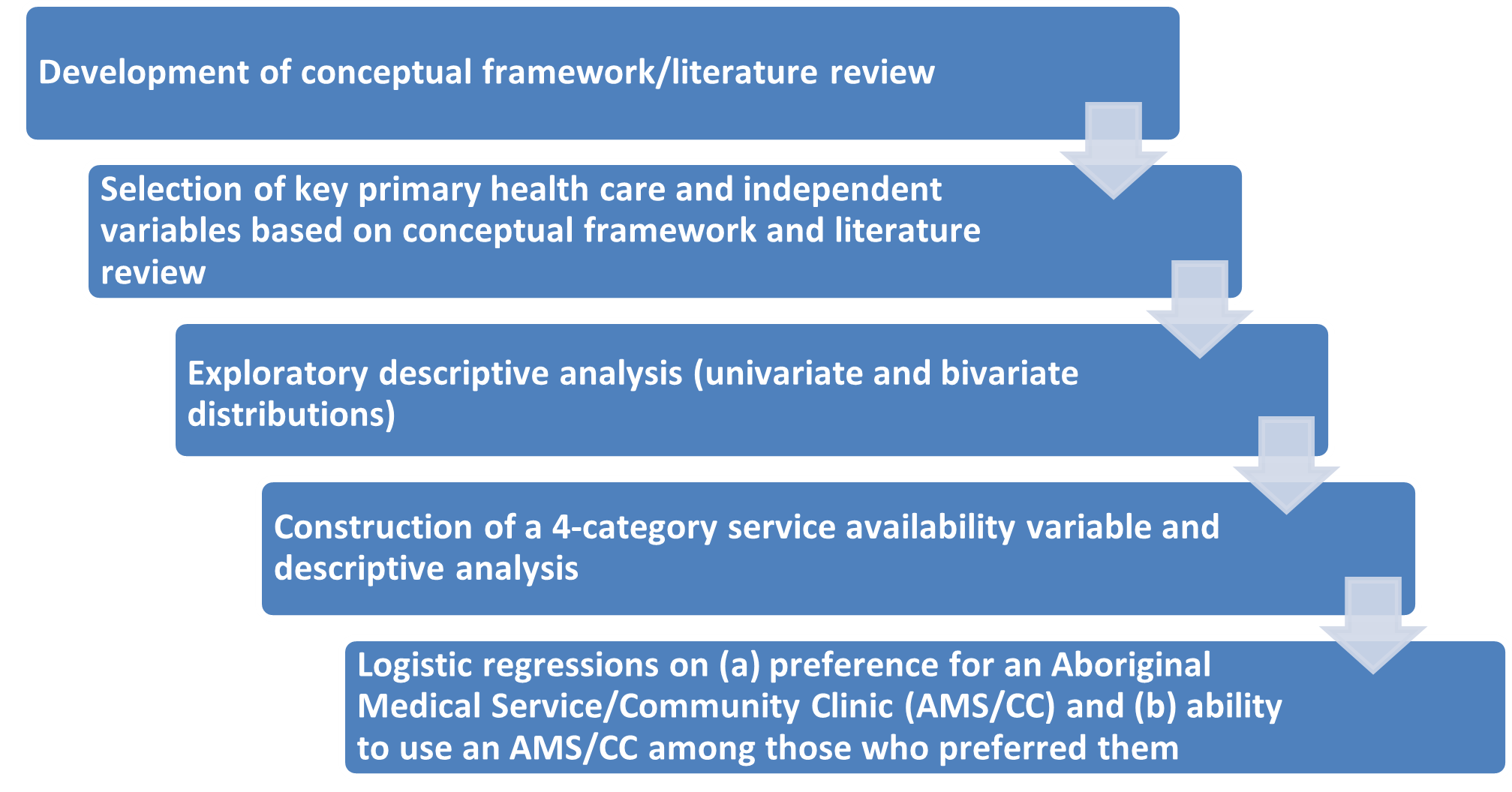
The conceptual framework and literature review were used to drive the selection of the primary health-care variables and independent variables to include in the analyses. Univariate and bi-variate analyses were undertaken using the ABS’s TableBuilder.[1]
One of the key variables in this project is the availability of primary health care services. The 2018–19 NATSIHS asked respondents to tick which ones from a selected list of health services[2] were available in their local area (noting that respondents defined their local areas themselves). This question thus captures perceived availability.
While the analysis in TableBuilder highlights how many people had each type of service in their local area, it cannot be used to look at whether there was more than one type of service in their area.
Using the unit record level data in the ABS’s DataLab environment, a variable was created which assigned respondents to one of 4 categories focusing on the types of GP services in their area:
- AMS/CC[3] only
- mainstream GP (other doctor/GP not from AMS or hospital) only
- both AMS/CC and mainstream GP
- neither AMS/CC nor mainstream GP[4] (no primary health services).[5]
This variable is designed to capture not only the distribution of service availability, but how much choice respondents have in what type of primary health service they use.
Building on the descriptive analyses (which focused on the relationships between individual variables and the primary health variables), the final step used multivariate logistic regression to examine the relative impact of a subset of these variables on 2 selected outcomes:
- preference for an AMS/CC
- whether the respondent was able to use an AMS/CC (among those who expressed a preference for one).
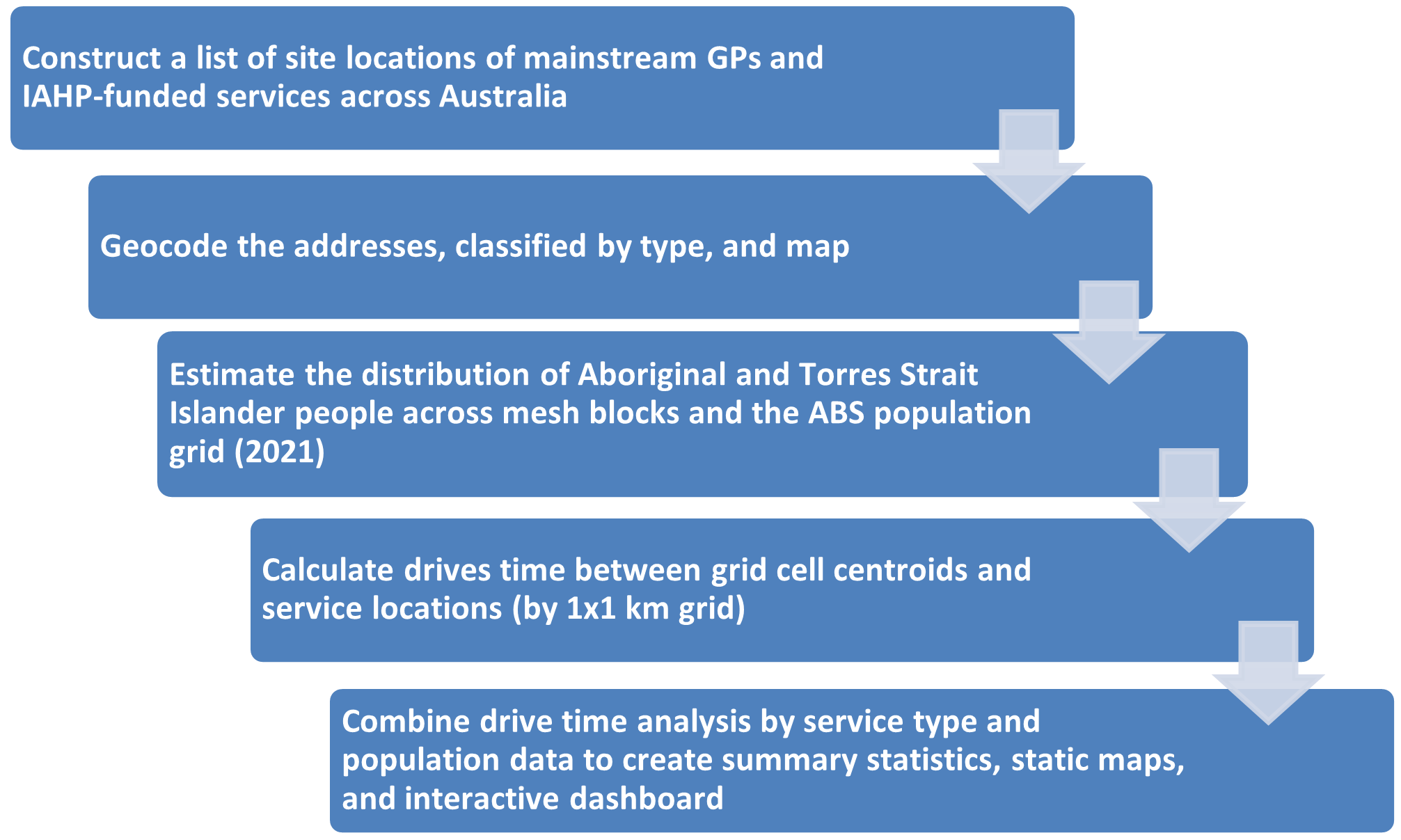
Overview of the spatial analysis
Figure 1.2: Steps for spatial analysis of primary health care services[6]