Mental health
Mental health services
Last updated:
Why collect data about mental health services?
This page provides an overview of a range of data sources that are used across the mental health site to describe mental health services in Australia.
Information about services, and the people who access those services, provides insights into how the mental health system operates. Data collected consistently over time can reveal how services are responding to changing population needs and events, such as the COVID-19 pandemic, natural disasters and policy changes.
For more information and data, go to Data sources.
Use of mental health services
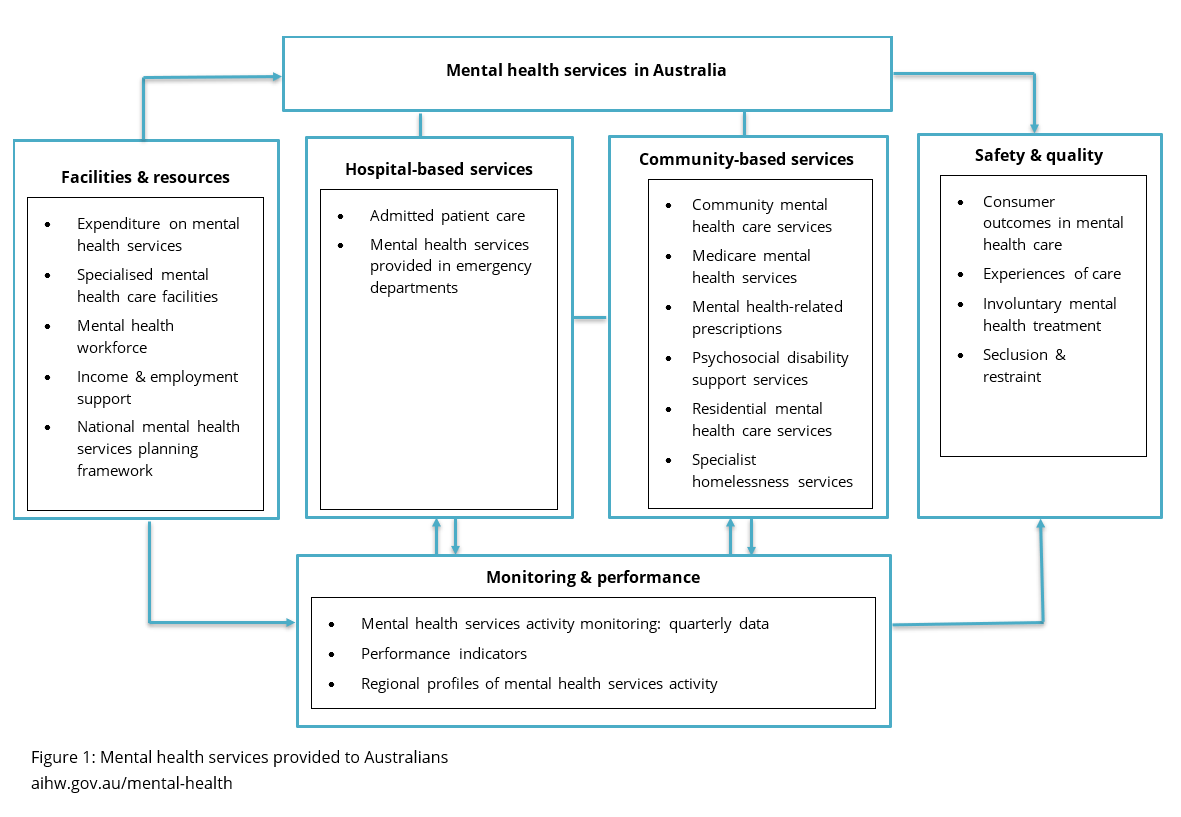
Mental health services provided to Australians are reported as a topic of Australia's health. Services are broadly categorised into hospital-based and community-based services with specific related topics illustrated in Figure 1. This section provides an overview of the data on mental health service activities in Australia in the latest available year.
Figure 1: Mental health services provided to Australians
 Hospital-based services
Hospital-based services
For some people, managing their mental health requires more intensive support that can only be provided in a hospital setting. This might include staying in a hospital ward for ongoing care, visiting an emergency department during a crisis, or attending appointments at an outpatient clinic for regular treatment and follow-up.
 Admitted patient mental health-related care
Admitted patient mental health-related care
Information on admitted patient mental health-related hospitalisations from Australian public and private hospitals are sourced from the National Hospital Morbidity Database (NHMD). It includes a collation of data on admitted patient care defined by the Admitted Patient Care National Minimum Data Set (APC NMDS).
In 2023–24, there was about 268,500 overnight mental health-related hospitalisations (79% in public hospitals) and 245,500 same day hospitalisations (77% in private hospitals).
For more information and data, go to:
- Admitted patient care – National data
- Admitted patient care – State and territory data
- Admitted patient care – Indicators
- Admitted patient care – Regional profiles
 Mental health services provided in emergency departments
Mental health services provided in emergency departments
Information on mental health-related emergency department are sourced from the National Non-Admitted Patient Emergency Department Care Database (NNAPEDCD). Data are available at the national, jurisdictional, and regional levels.
In 2024–25, there was about 318,200 presentations in public emergency departments.
For more information and data, go to:
- Mental health service provided in emergency departments – National data
- Mental health service provided in emergency departments – State and territory data
- Mental health service provided in emergency departments – Regional profiles
 Community-based services
Community-based services
Community-based services play a vital role in supporting people with mental illness by offering accessible, localised care. These services are typically delivered by government, not-for-profit organisations and Primary Health Networks.
 Community mental health care services
Community mental health care services
Mental illness is often treated in specialised community and hospital-based outpatient psychiatric services, which are referred to as specialised community mental health care (CMHC). Data to describe the care provided by CMHC services are from the Community Mental Health Care National Minimum Data Set (CMHC NMDS) that is compiled annually into the National Community Mental Health Care Database (NCMHCD).
In 2023–24, there were nearly 489,000 people who had 9.8 million service contacts with community mental health care services, an average of about 20 contacts each.
For more information and data, go to:
- Community mental health care services – National data
- Community mental health care services – State and territory data
- Community mental health care services – Indicators
- Community mental health care services – Regional profiles
 Residential mental health care services
Residential mental health care services
Residential mental health care (RMHC) services provide specialised mental health care on an overnight basis in a domestic-like environment. These facilities may provide a range of services including rehabilitation, treatment and extended care. Data from the National Residential Mental Health Care Database (NRMHCD), contributed by states and territories, are used to describe the care provided by these services.
In 2023–24, there were about 7,400 people in public residential mental health care who had 9,100 episodes of care, an average of 41 days per episode.
For more information and data, go to:
- Residential mental health care services – National data
- Residential mental health care services – State and territory data
 Mental health-related prescriptions
Mental health-related prescriptions
Statistics on mental health-related medications on subsidised prescriptions and under co-payment prescriptions (that is, prescriptions that cost less than the threshold for subsidy under the PBS) are sourced from the Pharmaceutical Benefits Scheme (PBS) and Repatriation Pharmaceutical Benefits Scheme (RPBS) data set.
In 2024–25, about 1 in 5 (19% of Australians) were dispensed mental health-related prescriptions with the majority of these issued by a General practitioner.
Approximately 10% of boys aged 5–17 years were dispensed psychostimulants, agents used for ADHD and nootropics nearly 3 times the proportion recorded in 2015–16.
For more information and data, go to:
- Mental health-related prescriptions
- ADHD medications dispensed 2004–05 to 2023–24
- Mental health-related prescriptions – Regional profiles
 Medicare mental health services
Medicare mental health services
Medicare-subsidised mental health services are delivered by Psychiatrists, General practitioners, Psychologists, and Other allied health professionals. These services are delivered in a range of settings – for example, hospitals, consulting rooms, home visits, and via telehealth – as defined in the Medicare Benefits Schedule (MBS). Information is provided on both patient and service provider characteristics and is limited to Medicare-subsidised services only.
In 2024–25, about 2.8 million Australians (10% of the population) received 13.0 million Medicare mental health services, representing a 7% increase from 2015–16.
For more information and data, go to:
- Medicare mental health services
- Medicare mental health services – Regional profiles
 Psychosocial disability support services
Psychosocial disability support services
People with serious mental illness may also have a psychosocial disability – a disability that results from mental illness. Information on specialist disability support services are provided under the National Disability Insurance Scheme (NDIS) to participants with a psychosocial primary disability and participants with a psychosocial secondary disability whose primary disability is not categorised as psychosocial.
As at 30 June 2025, people with a psychosocial primary disability formed the 4th largest primary disability group in the NDIS, totalling about 65,300 participants or 9% of all NDIS participants.
For more information and data, go to Psychosocial disability support services.
 Specialist homelessness services
Specialist homelessness services
Information on clients who accessed specialist homelessness services (SHS) agencies and were identified as having a current mental health issue is sourced from data provided by SHS agencies.
In 2023–24, of the clients SHS agencies assisted, 32% (or around 88,300 clients) had a current mental health issue.
For more information and data, go to Specialist homelessness services.
 Treatment use
Treatment use
People who experience mental illness or poor mental health can access a range of clinical and non-clinical mental health care and support services from across Australia’s mental health system. Data on treatment service use are sourced from the 2021 Household Income Labour and Dynamics in Australia (HILDA) survey.
In 2021, an estimated 11% of people aged 15 and over reported seeing a mental health professional in the previous year and 42% of those who reported being diagnosed with a mental health condition saw a mental health professional.
For more information and data, go to:
 Facilities and resources
Facilities and resources
There are numerous mental health services provided in Australian to support the mental health of Australians. Each service is funded and resourced to deliver effective mental health care.
 Expenditure on mental health services
Expenditure on mental health services
Information on recurrent expenditure, health expenditure, and health funding for mental health-related services in Australia are derived from a variety of sources.
In 2023–24, $14.5 billion was spent on mental health-related services, or an average of $537 per person.
For more information and data, go to:
 Specialised mental health care facilities
Specialised mental health care facilities
Specialised mental health care is delivered in and by a range of facilities including public, and private psychiatric hospitals, psychiatric units or wards in public acute hospitals, community mental health care services and government-operated, and non-government-operated residential mental health care services. Information on specialised mental health care facilities is drawn primarily from the National Mental Health Establishment Database (NMHED).
In 2023–24, there were about 1,670 specialised mental health care facilities with almost 7,080 public specialised mental health hospital beds.
For more information and data, go to:
 Income and employment support
Income and employment support
Income and employment support is available for people experiencing mental illness and their carers, and these include Disability Support Pension (DSP), Disability Employment Service (DES) and income support for carers.
As of June 2023, the Psychological/Psychiatric category made up 37% of all DSP recipients and about 110,000 people with a psychiatric primary disability were DES participants.
For more information and data, go to Income & employment support.
 Mental health workforce
Mental health workforce
Health care workers provide treatment, care, and support to people in mental health services.
Over the decade from 2015 to 2024, population rates (per 100,000 population) increased for all 5 specialist mental health professions.
In 2024, there were about 28,300 mental health nurses, 36,900 psychologists, 3,100 mental health occupational therapists, 3,400 accredited mental health social workers and 4,500 psychiatrists working.
For more information and data, go to Mental health workforce.
 National mental health services planning framework
National mental health services planning framework
The National mental health services planning framework (NMHSPF) is a comprehensive model designed to help plan, coordinate, and resource mental health services. The NMHSPF model brings together the best available evidence and expert opinion on:
- the prevalence of mental illness and need for mental health services
- the types and levels of mental health care required for different need groups
- efficient standards of health service operation to deliver this care.
For more information and data, go to National Mental Health Service Planning Framework.
 Safety and quality
Safety and quality
A safe and high-quality health system provides the most appropriate and best-value care, while keeping patients safe from preventable harm.
 Experiences of care
Experiences of care
Patient-reported experience measures (PREMs) are important tools in monitoring the safety and quality of the Australian mental health care system and driving service improvement. PREMs collect patients’ views about their experience of health services they received and the impact or outcomes of those services. In the reporting year 2023–24 in Australia:
- the Your Experience of Service (YES) survey showed between 49% and 83% of survey respondents indicated a positive experience in public mental health services.
- the Australian Private Hospital Association Patient Experience of Care survey found that 83% of survey respondents indicated a positive experience of overnight inpatient care in private hospital mental health services.
For more information and data, go to:
- Experiences of care
- Consumer experiences in public mental health services
- Patient experiences in private hospital mental health services
 Consumer outcomes in mental health care
Consumer outcomes in mental health care
The National Outcomes and Casemix Collection collects information using outcome measures completed by clinicians and consumers about a person’s clinical status during their mental health care in public specialised mental health services.
In 2023–24, clinician ratings using standardised measures showed Significant Improvement for patients in completed admitted (inpatient) care: at 61% (aged 11–17), 75% (aged 18–64) and 74% (65 and over) of episodes.
For more information and data, go to:
 Seclusion and restraint
Seclusion and restraint
Reducing and, where possible, eliminating the use of seclusion and restraint in Australian mental health care is a policy priority and has been supported by changes to legislation, policy and clinical practice (RANZCP 2021).
In Australian public hospital mental health care, the national seclusion rate (events per 1,000 bed days) has more than halved from 2009–10 to 2024–25. The physical restraint rate has been steady between 9 and 12 events per 1,000 bed days since 2015–16; the rate was 9 events in 2024–25.
For more information and data, go to:
- Seclusion and restraint
- Seclusion and restraint – Indicators
 Involuntary treatment in mental health care
Involuntary treatment in mental health care
Involuntary treatment is the compulsory assessment or treatment of people in mental health services without the person’s consent being given. This is a form of restrictive practice and can be legally approved under certain conditions.
During 2023–24, involuntary treatment was used in Australian public mental health services for about 15% of community care contacts, 17% of residential care episodes, 27% of non-acute and 46% of acute hospitalisations.
For more information and data, go to:
 Monitoring and performance
Monitoring and performance
Mental health services activity monitoring provides early insights into service usage and outcomes across regions to assess system performance. Performance indicators and regional profiles help identify trends, disparities, and areas for improvement, supporting data-driven planning and policy decisions.
 Mental health service activity monitoring: quarterly data
Mental health service activity monitoring: quarterly data
Reporting on mental health service activity offers early insights into how Australia’s mental health system delivers care and adapts to unexpected changes in population needs, including events like the COVID-19 pandemic and natural disasters.
During the September quarter 2025 (Q3), more than 3.4 million mental health MBS services were processed nationally and almost 257,000 phone calls were made to Lifeline.
For more information and data, go to Mental health service activity monitoring: quarterly data.
 Performance indicators
Performance indicators
A number of different mental health indicator sets have been developed over time to measure the performance and progress in the delivery of services across the mental health sector. Indicators that are used to measure safety and quality in the mental health care system under Australian and international frameworks include:
- positive patient-rated experiences of care
- positive change in consumers’ clinical outcomes after care
- low or no use of restrictive practices, such as seclusion, restraint, and involuntary treatment
- other indicators relating to expenditure on mental health, specialised facilities, treatment use, admitted patients and community mental health care services.
For more information and data, go to Performance indicators.
 Regional profiles of mental health service activity
Regional profiles of mental health service activity
The National Mental Health and Suicide Prevention Agreement emphasises the importance of making detailed data available by local geographies to more effectively plan services, and monitor progress and outcomes to achieve this goal.
An interactive data tool has been designed to present integrated regional profiles of mental health service activity. It currently includes data on admitted care, emergency care, community care, Medicare services, and prescriptions by region, sex and age group for 2018–19 to 2023–24. Future releases will expand the tool to include additional information.
For further information about the tool and how it can be used, refer to Regional profiles of mental health service activity.
Where can I find more information?
The AIHW’s Mental health website describes the activity and characteristics of Australia’s health and social care services accessed by people for mental health-related concerns.
For more information about:
- mental health and the impact of mental illness and distress, go to Prevalence and impact of mental illness, Stress and trauma, and Physical health of people with mental illness
- mental health services, go to Australia’s mental health system and various Topic areas of the AIHW Mental health online report site
- safety and quality indicators of mental health services, go to Mental health performance indicators.
If you or someone you know needs help, these resources are available:
- Lifeline (Phone 13 11 14)
- Kids Helpline (Phone 1800 551 800)
- Beyond Blue (Phone 1300 224 636)
- Medicare Mental Health